










Services on Demand
Journal
Article
 text in
text in  Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
Print version ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.23 no.1 Medellín July/Dec. 2011
ORIGINAL ARTICLES DERIVED FROM RESEARCH
Skeletal, facial and dentoalveolar changes produced by treatment with acetate plates and Class III elastics in patients with skeletal and dental mesiorelation in early deciduous or mixed teething
Gabriel Espinal Botero1, John Jairo Betancur Pérez2, Ana María Blandón Uribe3, Paola Alejandra Ortiz Burgos4
1 Dentist. Specialist in Odontopediatrics, associated professor at
Universidad de Antioquia. E-mail: sasa@une.net.co
2 Dentist. Specialist in Teenager Integral Dentistry. Specialist in Health
Services Management: Marketing. Specialist in University Didactics.
Associated professor of the School of Dentistry at Universidad de
Antioquia, Medellín Colombia. E-mail: celba@une.net.co celba@une.net.co
3 Dentist. Specialist in Children Integral Dentistry and Maxillary Orthopedics,
Graduate student: Teenager Integral Dentistry and Orthodontics
4 Dentist. Graduate student to the Program Integral Dentistry in Children
and Maxillary Orthopedics
SUBMITTED: OCTOBER 6, 2009 - ACCEPTED: MAY 3, 2011
CORRESPONDENCIAGabriel Espinal Botero
Facultad de Odontología
Universidad de Antioquia
Correo electrónico: sasa@une.net.co
Espinal GE, Betancur JJ, Blandón AM, Ortiz PA. Skeletal, facial and dentoalveolar changes produced by treatment with acetate plates and Class III elastics in patients with skeletal and dental mesiorelation in early deciduous or mixed teething. Rev Fac Odontol Univ Antioq 2011; 23(1): 37-55.
ABSTRACT
INTRODUCTION: the purpose of this study was to establish the clinical and radiographic changes produced by using bimaxillary acetate plates with Class III elastics during one year for treatment of skeletal Class III in patients with early deciduous or mixed dentition.METHODS: a quasi-experimental prospective clinical study was carried out in 26 subjects, ages three to nine years. Lateral cephalometric radiographs and study models were taken at the beginning, six months, and one year of treatment; post-treatment changes were evaluated after three years in five subjects. During the statistical analysis descriptive measures were obtained, and the Anova test for repeated measures was used to determine changes over time; also, the nonparametric Wilcoxon test was used with a significance level of 0.005.
RESULTS: favorable skeletal changes were achieved in the mandible, especially at the SNB, facial and gonial angles, the pog distance perpendicular to N, the lower anterior facial height, and the Y axis; dentoalveolarly, there were improvements in both horizontal overbite and Witts, as well as in facial aesthetics, as evidenced by the decrease of the E-plane FH angle and lower lip protrusion. After three years of treatment, stability of the results was observed.
CONCLUSIONS: acetate plates with Class III elastics demonstrated to be a stable and effective therapy, according to evaluation three years after treatment, for facial improvement of skeletal Class III with anterior crossbite in early primary or mixed dentition.
Key words: Angle Class III malocclusion, orthopedic appliances, orthopedic appliances design.
INTRODUCTION
Mesiocclusion skeletal relationships are connected to an osseous alteration usually accompanied by Class III dental relationships and anterior crossbite.1 Such a disharmony may be the result of alterations in size (big mandible and small maxillary), or in the position of both structures (forward-oriented mandible and/or retropositioned maxilla).1, 2
Although the main etiologic factor of Class III malocclusions is the hereditary component, which appears early in life,2,3 this condition also exhibits a multifactorial etiology, that is, an interaction of genetics and environment.4
Therapy alternatives for this type of malocclusion include mainly: chin cup treatment,5, 6 maxillary protraction face mask,7, 8 and bimaxillary orthopedic apparatus.9,10 The choice will depend, among other factors, on the etiology and the patient´s biological age, but researchers generally agree that early orthopedic correction will favor further craniofacial development.2,11
In 1977, seeking early treatment of Class III malocclusions, Falconi et al12 suggested the use of two— maxillary and mandibular—acetate plates with complete occlusal coverage and vestibular hooks joining the plates together by means of Class III intermaxillary elastics. Later on, in 1998, Franchi and Baccetti13 reported two cases successfully treated with this type of appliances.
This work seeks to assess the dentoalveolar, facial and skeletal changes produced by a one-year treatment with bimaxillary acetate plates with smooth occlusal planes and Class III elastics as an alternative to early treatment of the skeletal mesiorelation, as proposed by Falconi et al.12 With this purpose, the size of the sample used in 2001 by Espinal et al14 was increased, and it was also used to determine post-treatment stability.
MATERIALS AND METHODS
A quasi-experimental prospective clinical study was performed, making interventions with bimaxillary acetate plates (which worked as anchorage for intermaxillary elastics with a Class III vector) in a sample of 26 individuals of both sexes, between 3 and 9 years of age, who were selected for convenience of the Dentistry Care Center of the Dentistry Department at Universidad de Antioquia following these inclusion criteria: between 3 and 9 years of age with skeletal mesiorelation cephalometrically confirmed, anterior crossbite or edge-to-edge bite, with or without posterior crossbite (uni- or bilateral). The criteria for exclusion were: previous maxillary orthopedic treatment, pseudo-Class III occlusion, skeletal or dental open bite, premature loss of teeth or early extractions, signs and symptoms of temporomandibular joint dysfunction, track record of maxillofacial trauma, congenital anomalies and maxillary development-related syndromes. Twenty one of them were new patients and five were taken from the study made in 2001 by Espinal et al,14 in order to assess their post-treatment stability.
After preparing a complete medical record, and once the diagnostics had been defined, an informed consent was signed, and the following steps were completed: upper and lower arch impressions were taken using Coe American Style® perforated trays, Jeltrate Kerr® impression material was prepared following the distributor´s directions (7 g of powder in 19 ml of water), and stone gypsum models were obtained (100 mg of powder in 28 ml of water) on which removable acetate plates were made on Dentsplay® acetate 0.8 mm thick (the models were taken after 6 and 12 months of treatment following the same specifications).
Construction of the plates followed the design proposed by Franchi and Baccetti;13 they were made by the same laboratory operator and verified by the main researcher. Each plate contained a hook made on Ormco® steel wire 0.03" located on vestibular in order to anchor the elastic in a position distal to the second upper deciduous molar, and mesial to the lower canine. The plates were made on smooth occlusal surfaces in order to allow free movement of the maxillaries; they were located distal to the second deciduous molars, covering all the teeth along the vestibular and lingual surface in order to achieve maximum anchorage and to prevent individual vertical or antero-posterior changes in dental structures (figure 1).
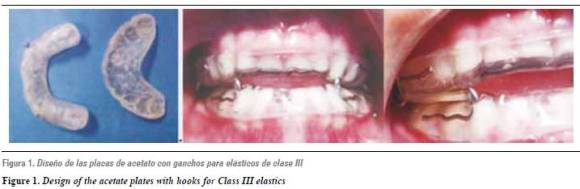
Once the plates had been installed, the patients and their parents were given directions on how to use intermaxillary elastics with a Class III vector, from the hook located in the molar region of the upper plate up to the hook located in the canine zone of the lower plate. The elastics were replaced each 24 hours and force application grew increasingly: three and a half ounces during the first three weeks; four and a half ounces the next three weeks, and six ounces from the ninth week on. Directions were given on how to use the appliances during most part of the day and all through the night (16 hours a day on average) and monthly controls were made to evaluate hygiene, motivate, verify the adequate use of the appliances, and to make adjustments in plate retention rebasing them with acrylic, if needed.
Radiographic evaluation: three lateral cephalic Xrays were taken in three different moments: T1 at the beginning of treatment for diagnostic purposes, T2 after six months of installation of the appliances, and T3 after one year of treatment (figure 2). Between T2 and T3, three of the 21 patients withdrew; therefore, the sample lowered to 18 individuals. For the post-treatment stability estimation, lateral cephalic X-rays were taken three years after finishing treatment (T4) to five patients with the same treatment conducted by Espinal et al in 2001.14

A Panorex equipment INSTRUMENTARIUM Mod. LL 100 910 series with the following features was used: 77 kW, 12 mA. Distance focus-film 165 mt. Distance focus-target 150 mt. Exposure time 0.5 sec. Film AGFA ORTHO CPG plus 20 x 25. Parallelism between the Frankfort plane and the floor was verified, taking into account the mirror method and verifying auricular pins placement on the head´s natural position. Estimated magnification for this equipment is close to 8%.
The radiographs were processed on an automatic developer Air Techniques 2000® Plus using developing/ fixing liquid Kodak RPX, Omat, following the manufacturer´s instructions. The technical staff was standardized in order to achieve similar results in terms of structure and tissue contrast at the time of exposure and in data gathering procedures.
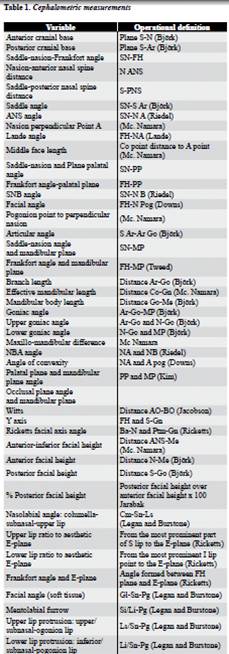
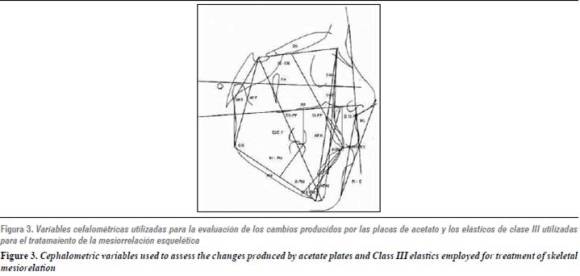
A mixed tracing was applied with measurements taken from different analyses (table 1, figure 3) . All the radiographs were drawn and measured by the same operator to whom the Pearson´s correlation test was applied in order to establish the error rate. The second radiographs from all patients were randomly selected as well as the SNB angle, resulting in a statistically significant calibration (coefficient r = 0.996, p < 0.05). For a more adequate approximation, the inter-class correlation coefficient (ICC) was applied, as it helps to assess general concordance between two or more measurement methods of different observations in continuous variables. The ICC was of 0.994, which allowed ensuring that reliability was adequate. The traces were drawn with a 0.5 mm propelling pencil on acetate paper 0.03" thick (Truvision Cephalometric Tracing Acetate).
For linear and angular measurements, an Ormco cepha (Ormco-SYBRON) cephalometric ruler was used. Both linear and angular measurements were approximate to the larger 0.5.
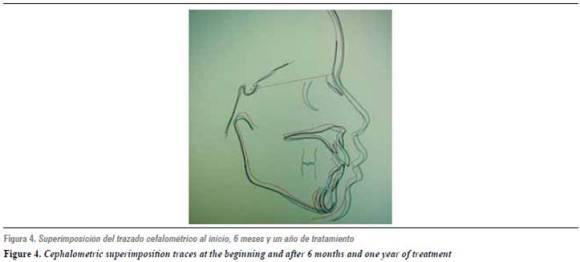
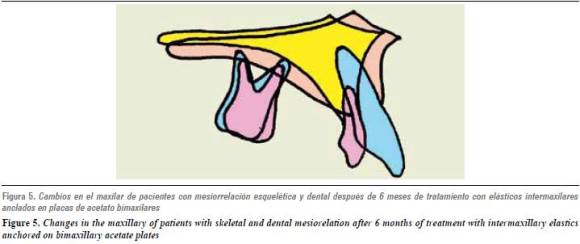
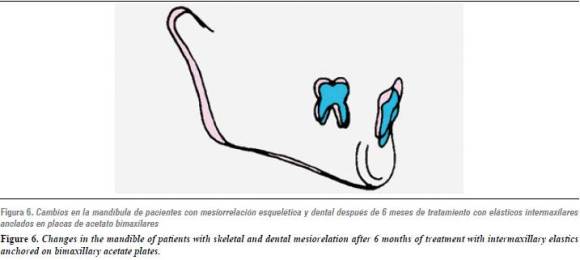
In order to establish the general growth pattern, a cephalometric superimposition of the initial radiograph was made after six months and at the end of treatment on the saddle-nasion plane (figure 4). In order to establish the individual behavior of maxillary and mandible, a superimposition on the palatal plane was made, as well as on the inferior dental nerve conduct and on the symphysis, respectively (figures 5 and 6 ).
Once the period of treatment ended, bionator-like devices were placed on the patients as a retention aid, to continue under supervision at the School´s clinics, depending on the specific characteristics of each case.
For the statistical data analysis, the Excel and SPSS 15.0 software were used. A descriptive analysis of the radiographic variables was made, as well as an independent representation of the behavior of each variable by means of the Anova test of repeated measurements to establish changes through time. A design of related samples was applied using the non-parametric Wilcoxon test to determine changes after six months and one year of treatment in relation to the beginning. The significance level considered for the tests was 0.005.
RESULTS
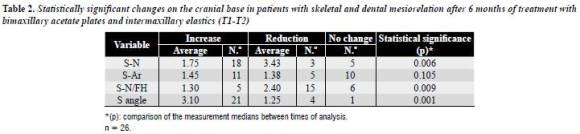
Table 2 displays the variations in the cranial base. The only statistically significant change observed (being p < 0.005) is the average increase (3.1°) in the saddle angle at the expense of posterior cranial base between T1 and T2 in 21 observed patients. The SN/FH angle was reduced or remained unchanged in all the 21 patients of the sample (table 2).
Concerning the maxillary in the sagittal plane, between T1 and T2 (table 3) a statistically significant increase was found in the middle face length (size) averaging 2.85 mm in 20 patients. The remaining changes were not statistically significant, and included lowered distance from A to the perpendicular of N in 16 patients (-1.8), Lande´s angle reduction (3.43°) in 17 patients and SNA angle increase (1.7°) in 11 out of 21 patients. After one year of treatment (T1/T3) there are no statistically significant changes.
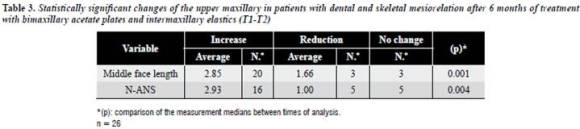
The maxillary showed an increase in the vertical plane in all the measurements between T1 and T2 (table 3) without a tendency to rotate within a defined direction. However, the only statistically significant change was the increase in the N-ANS distance observed in 16 patients with an average of 2.93. Between T1 and T3 the increase in vertical development continues, being more significant in the posterior region (distance S-PNS) with an increase of 2.43 mm in 16 patients.
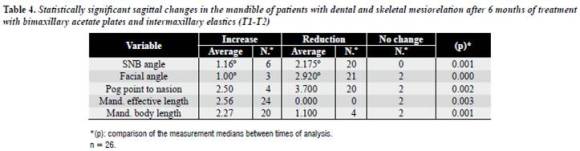
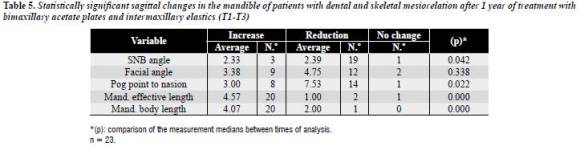
Concerning the mandible in the sagittal plane, all of the measurements showed statistically significant changes between T1 and T2 (table 4); an increase in effective length and in mandibular body length was observed along with a reduction in SNB angle, facial angle and pog point perpendicular to N. Between T1 and T3 (table 5), even though it was not statistically significant, facial angle decreased in 12 patients (4.75° on average) and the SNB angle was reduced in 19 of the 23 patients of the sample (2.39° on average) with an average increase of 4.57 mm in mandibular effective length and 4.07 mm in mandibular body length (20 patients).
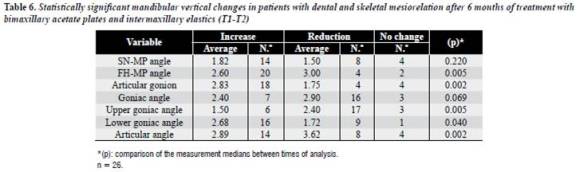
At the mandibular level in the vertical plane (table 6), statistically significant changes occurred during the first 6 months of treatment in the FH-MP angle measurements (clockwise rotation), the Ar-Go distance (branch length), the upper goniac angle and the Ar angle.
Concerning maxillomandibular relationships in the sagittal direction (table 7) an increase in Witts (3,4) was observed between T1 and T2 in the 21 patients, and between T1 and T3 (4,02) in 20 of the 21 patients, both being statistically significant and expressing a better relationship between maxillary and mandible. In the vertical plane (table 7), statistically significant changes are observed only between T1 and T2, given by an increase in the Y axis measurement, anterior facial height and lower antero-facial height.
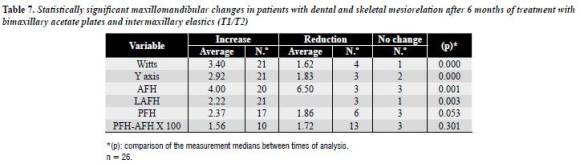
It is worth noting that, even though it didn´t reach statistical significance, a higher average increase occurs in the posterior facial height compared to the anterior facial height, both at six months and after one year of treatment (figures 1 and 2).
The cephalometric comparison of the post-treatment measurements between T3 and T4 revealed an increase with no statistical significance (p < 0.005) in SN, as well as mandibular effective length and maxillomandibular difference measurements in all the patients. On the superimposition, greater development in the sagittal direction was observed in the upper maxillary, while in the mandible the development was mainly in the vertical direction.
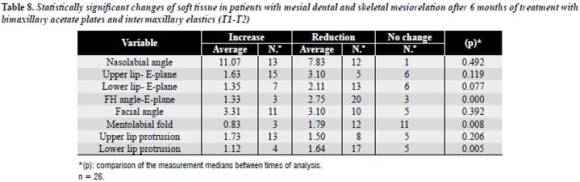
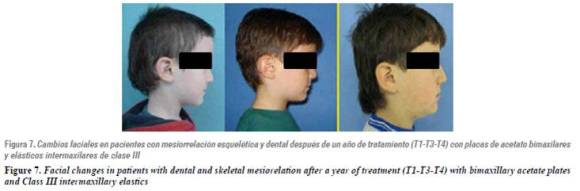
Concerning soft tissue (table 8), after 6 months of treatment (T1-T2) a statistically significant reduction was found in lower lip protrusion (1.64 mm) and in FH- E-Plane angle (2.75°), and a statistically significant increase in facial angle (4,15°) was observed after a year of treatment (T1-T3). It is worth mentioning that during the period of observation most patients exhibited an increase in the nasolabial angle (8.23°) and on upper lip protrusion (2.36 mm), as well as a reduction of mentolabial fold, which failed to achieve statistical significance (figure 7).
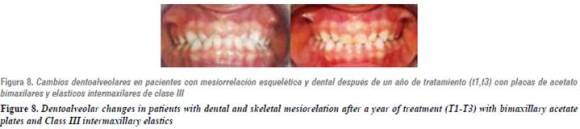
Changes in vertical and horizontal overbite clinically measured showed statistical significance between T1 and T3, exhibiting an overjet increase with 2.79 mm average in 22 of 23 patients and an overbite increase of 2.05 mm in 16 of 23 patients (figure 8).
In terms of canine relationships, an average change of 2.51 mm was found, moving from Class III relationships to Class II relationships in 12 patients and to Class I relationships in 10 patients. Concerning molar relationships, improvement was observed in 20 patients, moving from a mesial scale to a straight terminal plane averaging 2.43 mm.
In patients evaluated during the retention phase (T3/ T4), a vertical overbite increase was found in 3 of them in 0.9 mm average, and a lower increase in vertical overbite of 0.75 mm on average was found in 2 patients.
Sagittaly, between T3 and T4 a better relationship of horizontal overbite was achieved in 4 of 5 patients, with an average increase of 1.25 mm. Generally, stability of molar and canine relationships was observed after the treatment was finished; this agrees with the findings of the previous study.
DISCUSSION
Class III skeletal relationship is one of the occlusal diseases with the most complex diagnostic and treatment. Depending on the patient´s age, different kinds of treatment may be implemented, each featuring possibilities and drawbacks.
The early treatment approach has been recommended by several authors such as Mc Namara,9 Petit,15 Franchi and Baccetti.13 The latter suggest that the optimal period to improve Class III skeletal relationships with functional appliances is during early deciduous and mixed dentition. In some cases, it is even considered that early treatment may reduce the need of surgical interventions at later ages.10, 12, 16, 17.
The difficulties in assessing the findings of this study are related to the stages of growth of the population under observation, and to the lack of studies on the growth of patients with development disharmonies, which would allow comparisons. In this sense, Reyes´ study in 2006,3 in which untreated Class III growing patients were compared to patients with developing Class I skeletal relationships, revealed no differences in the maxillary sagittal position among the patients. However, the mandible of Class III patients displayed an effective length and anterior-inferior facial height increase significantly higher than those of class I.
In this study, the statistically significant change in the saddle angle (table 2), and the increase in the S-N distance prove that the population under study was undergoing, on average, a more active period of growth during the first 6 months of observation; this may explain why the changes found were mainly in terms of position rather than size.
According to Franchi and Baccetti,13 the orthopedic effect of Class III elastics used with acetate plates generates a line of action of a retrusive force on the mandible, passing through or right behind the center of the mandibular condyle. This produces in the long term a clockwise rotation in the mandible, accompanied by a reshaping and counterclockwise rotation of the lower dentoalveolar component because of the force vector passing over the centre of resistance of the dental component. In the maxillary, the line of action has the same magnitude, but a protrusive direction, which generates a counterclockwise rotation on the palatal plane. In the present study, this rotation (given by the reduction in FH-PP angle) was observed only in 11 patients and did not reach statistical significance in the first six months of treatment; paradoxically the N-ANS measurement is the only one showing a statistically significant increase (in opposition to the counterclockwise rotation), which may be explained by the period of vertical development undergone by the individuals of the sample and which is also observed in the posterior sector (S-PNS increase, showing a counterclockwise rotational tendency after six months of treatment).
On the contrary, in patients treated with a disjunctor and a protraction mask, authors like Nartallo- Turley,18 Da Silva et al.,8 Turley,19 and Major21 have found a clockwise rotation of the maxillary during treatment, which is explained, in this case, by the position of the elastic force vector located anterior to the center of resistance. These findings suggest that the use of this type of therapy should not be performed in patients with a tendency to anterior overbite.
The protrusive effect on the maxillary presents statistical significance in the first six months in the middle face length level, which increased in 20 out of 26 patients with a 2.85 mm on average.
Regarding the mandibular size, one would expect that the effective length remained stable as a consequence of the treatment under ideal conditions. However, an increase was observed in both the mandibular effective length (2.56 mm after 6 months and 4.57 mm after one year of treatment), and body length (2.27 mm after 6 months and 4.07 mm after one year); this is similar to the reports by Saadia et al17 and McNamara,22 who studied Class III patients treated with a protraction mask, which also failed to keep the length of the mandible stable, having an average increase of 4 mm.
In this study, a mandibular retro-positioning in the sagittal direction was found to be statistically significant in the first six months of treatment (SNB, facial angle and pog point perpendicular to N). This more posterior position of the mandible persisted all throughout the study, but with a small increase between T2 and T3, which explains the lack of statistical significance at the end of the observation period, and establishes a guideline for the achievement of goals in short-term treatments (6 months).
In the vertical plane, an increase of anteroinferior facial height occurred, as well as in the Y growth axis, and the goniac angle. This is an indication of downwards and backwards mandibular rotation, agreeing with the findings reported by Franchi and Baccetti,13 and Espinal et al.14 However, the increase in posterior facial height occurring in 17 patients after 6 months of treatment and in 12 patients at the end of the observation period demonstrates that patients are in a period of active vertical development not only anterior —as Reyes3 and Mitani23 mention—, but also posterior, which is clinically important to keep the proportions, even though it is not statistically significant.
Regarding maxillomandibular relationships in the sagittal plane, both ANB angle increase—also reported by Franchi and Baccetti—13 and Witts increase favor correction of the facial profile from the first period, and it is kept throughout the treatment.
Accordingly, an increase in the Y axis angle was also found, as well as in the anterior facial height and the lower-anterior facial height, indicating a vertical compensation of sagittal dysplasia similar to the one reported by Saadia17 in a study in 112 patients between 6 and 12 years of age, who were treated with maxillary expansion and face mask showing an increase in FH-MP angle, SN-MP angle, and in Ricketts facial axis, although, as explained above, the orthopedic effect might be different. This may be explained by the vertical growth pattern characteristic of Class III patients, which is common to both samples, regardless of the different age ranges (3-9 years and 6-12 years).
Dentoalveolar changes were significant, with an improvement of canine-molar relationship, moving in most cases (96%) from Class III to Class I relationships. In regards to horizontal overbite, all the patients experienced correction of anterior crossbite with changes of 2.79 mm on average, moving from negative to positive values in 22 of 23 patients. Regarding vertical overbite, an increase was found in 16 of 23 patients.
The reports by Nartallo-Turley,18 Saadia17 and Hickham24 concerning soft tissues include an upper lip forward movement, and a chin downward/backward movement. In this study, soft tissues showed improvement of the facial profile clinically and cephalometrically demonstrated, given by a more posterior position of the pogonion point and the lower lip and by a better expression in mentolabial fold and nasolabial angle, all of which contributes to facial aesthetic rehabilitation (figure 4).
In relation to long-term results in patients treated with this kind of appliances, dentoalveolar and facial skeletal stability was generally observed.
The most significant changes were represented by an increase in both anterior cranial base length and mandibular effective length, which agrees with the studies by Ferro et al.,20 who pointed out that longterm stability of this kind of treatment was related to the degree of intercuspidation achieved, and that recurrence was directly related to mandibular ramus growth after treatment.
It is also important to point out that during the observation period an increase in nasolabial angle (8.23°) and in upper lip protrusion (2.36 mm) was observed in most patients (13-15), as well as a reduction in mentolabial fold, which, even if it did not reached statistical significance, may have significantly contributed in a clinical way to improve the aspect of soft tissues of the population under study at the end of the observation period.
CONCLUSIONS
Acetate plates with Class III elastics proved to be an effective and stable therapy after three years of post-treatment assessment for both facial and dentalskeletal mesiorelation improvement in patients with deciduous and mixed dentition from the sample evaluated.
The main results are achieved in the first six months of treatment and are due to changes in mandibular position that are expressed both in the sagittal and the vertical planes (SNB and facial angle reductions accompanied by clockwise rotation) and an increase in middle face length, which is reflected in some Witts increase, higher vertical and horizontal overbites and a reduction in lower lip protrusion. Soft tissue facial angle increase is achieved after a year of treatment.
This therapy does not suppress the increase in mandibular effective length characteristic of patients with Class III skeletal relationships.
ACKNOWLEDGEMENTS
To the Universidad de Antioquia´s Facultad de Odontología. To Doctor Mónica Jones for her methodological contributions. To the patients for their participation and contributions.
1. Delaire J. Maxillary development revisited: relevance to the orthopedic treatment of Class III malocclusions. Eur J Orthod 1997; 19(3): 289-311. [ Links ]
2. Nakasima A, Ichinose M, Nakata S, Takahama Y. Hereditary factors in the craniofacial morphology of Angle's Class II and Class III malocclusions. Am J Orthod 1982; 82(2): 150-156. [ Links ]
3. Reyes BC, Baccetti T, McNamara JA Jr. An Estimate of craniofacial growth in Class III malocclusion. Angle Orthod 2006; 76(4): 577-584. [ Links ]
4. Nakasima A, Ichinose M, Nakata S. Genetic and environmental factors in the development of so-called pseudo- and true mesiocclusions. Am J Orthod Dentofacial Orthop 1986; 90(2): 106-116. [ Links ]
5. Graber LW. Chin cup therapy for mandibular prognathism. Am J Orthod 1977; 72(1): 23-41. [ Links ]
6. Sakamoto T, Iwase I, Uka A, Nakamura S. A roentgenocephalometric study of skeletal changes during and after chin cup treatment. Am J Orthod Dentofacial Orthop 1984; 85(4): 341-350. [ Links ]
7. Takada K, Petdachai S, Sakuda M. Changes in dentofacial morphology in skeletal Class III children treated by a modified maxillary protraction headgear and a chin cup: a longitudinal cephalometric appraisal. Eur J Orthod 1993; 15(3): 211-221. [ Links ]
8. Da Silva Filho OG, Macro AC, Capelozza Filho L. Early treatment of the Class III malocclusion with rapid maxillary expansion and maxillary protraction. Am J Orthod Dentofacial Orthop 1998; 113(2): 196-203. [ Links ]
9. McNamara JA Jr., Brudon WL. Tratamiento ortodóncico y ortopédico en la dentición mixta. 4.ª ed. Michigan: Needham Press; 1995. [ Links ]
10. Baccetti T, Tollaro I. A retrospective comparison of functional appliance treatment of Class III malocclusion in the deciduous and mixed dentitions. Eur J Orthod 1998; 20(3): 309-317. [ Links ]
11. Litton SF, Ackermann LV, Isaacson RJ, Shapiro BL. A genetic study of Class III malocclusion. Am J Orthod 1970; 58(6): 565-577. [ Links ]
12. Falconi P, Tenti FV, Melis MT. Precocious correction of cross bite of incisors by intermaxillary traction on removable masticatory plates. Mondo Ortod 1977; 19(3): 14-23. [ Links ]
13. Franchi L, Baccetti T. Splint therapy for skeletal class III maloclusión in the primary dentition. J Clin Pediatr Dent 1998; 22(2): 93-98. [ Links ]
14. Espinal G, Betancur JJ, Carrillo N, Piedrahita MT. Evaluación de los cambios esqueléticos y dentales producidos con el tratamiento con placas de acetato y elásticos de clase III en pacientes con mesio-relación esquelética y dental en dentición primaria o mixta temprana. Rev Fac Odontol Univ Antioq 2005; 16(1): 70-80. [ Links ]
15. Petit H. Adaptation following accelerated facial mask therapy. En: McNamara JA Jr., Ribbens KA, Howe RP. Clinical alterations of the growing face monograph. Craneofacial growth series. Ann Arbor: Center for Human Growth and development. University of Michigan; 1983. [ Links ]
16. Kapust AJ, Sinclair PM, Turley PK. Cephalometric effects of facemask/ expansion therapy in Class III children: a comparison of three age groups. Am J Orthod Dentofacial Orthop 1998; 113(2): 204-212. [ Links ]
17. Saadia M, Torres E. Sagittal changes after maxillary protraction with expansion in Class III patients in the primary, mixed, and late mixed dentitions: a longitudinal retrospective study. Am J Orthod Dentofacial Orthop 2000; 117(6): 669-680. [ Links ]
18. Nartallo-Turley PE, Turley PK. Cephalometric effects of combined palatal expansion and facemask therapy on Class III malocclusion. Angle Orthod 1998; 68(3): 660-680. [ Links ]
19. Turley P. Orthopedic correction of Class III malocclusion: retention and phase II therapy. J Clin Orthod 1996; 39(3): 313-324. [ Links ]
20. Ferro A, Perillo N L, Ferro F, Gallo C. Long-term stability of skeletal Class III patients treated with splints, Class III elastics and chincup. Am J Orthod Dentofacial Orthop 2003; 123(4): 423-434. [ Links ]
21. Major PW, Elbadrawy HE. Maxillary protraction for early orthopedic correction of a skeletal Class III maloclussion. Pediatr Dent 1993; 15(3): 203-207. [ Links ]
22. McNamara JA Jr. An orthopedic approach to the treatment of Class III maloclussion in young patients. J Clin Orthod 1987; 21(9): 598-608. [ Links ]
23. Mitani H, Sakamoto T. Chin cup force to a growing mandible long-term clinical reports. Angle Orthod 1984; 54(2): 93-122. [ Links ]
24. Hickham JH. Maxillary protraction therapy: Diagnosis and treatment. J Clin Orthod 1991; 25(2): 102-104. [ Links ]

