










Services on Demand
Journal
Article
 text in
text in  Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
Print version ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.23 no.1 Medellín July/Dec. 2011
REVIEW ARTICLE
Orthodontic treatment of deep bite1
Beatriz Magali Cruz Moreno2, Carmen Elena Muñoz Gaviria3
1 This article stems from the clinical academic activity (Thursday
sessions) of the Especialización Clínica en Ortodoncia, at Facultad de
Odontología Universidad de Antioquia.
2 Dentist. Student of V semester of the Especialización Clínica en
Ortodoncia, at Facultad de Odontología Universidad de Antioquia.
Medellín, Colombia. E-mail address: bmagalicruz@gmail.com
3 Dentist. Student of V semester of the Especialización Clínica en
Ortodoncia, at Facultad de Odontología Universidad de Antioquia.
Medellín, Colombia. E-mail address: cemgtam@yahoo.com
RECIBIDO: OCTUBRE 20/2009 - ACEPTADO: MAYO 13/2011
CORRESPONDENCIABeatriz Magali Cruz Moreno
Facultad de Odontología
Universidad de Antioquia
E-mail address: bmagalicruz@gmail.com
Cruz BM, Muñoz CE. Tratamiento ortodóncico de mordidas profundas. Rev Fac Odontol Univ Antioq 2010; 23(1): 158-173.
ABSTRACT
Adequate vertical overbite is an important purpose of the orthodontic treatment, in terms of the achievement of esthetic goals (tooth display) as well as functional, stable and long-lasting occlusal relations. Development of excessive vertical overbite is known as deep bite, and it is usually found in some maxillomandibular discrepancies, as in Angle Class II division 2 malocclusions. Deep bite orthodontic correction or camouflage can be achieved by means of biomechanics of posterior teeth extrusion, anterior teeth intrusion, and/or incisors labialization. Choosing the right mechanics depends on the patient’s specific facial, occlusal and functional characteristics. The purpose of this review is to summarize the aspects associated to the diagnosis and orthodontic treatment of deep bite.
Key words: tooth movement, malocclusion, orthodontic extrusion.
INTRODUCTION
Vertical overbite may be defined as the upper teeth vertically overlapping the lower teeth, and it is expressed by the percentage of lower crown length covered by the upper teeth. It is considered adequate when in a rank of 37,9 to 40%; when larger than that, it is called deep bite.1-3 The presence of deep bite may predispose the patient to the development of periodontal and functional problems, and to alterations of the maxillaries normal development (in growing patients).4, 5 Deep bite usually makes part of maxillomandibular discrepancies that also threaten the sagittal and transverse planes; it is more frequently associated to Angle Class II Division 2 malocclusions, and to the hypodivergent skeletal pattern.1, 6, 7
The first step to the right treatment of this type of malocclusion is identification of its origin, considering dental, skeletal and functional levels of involvement, in order to finally correct the discrepancy, and to obtain a functional occlusion in harmony with the patient’s esthetic characteristics and stable in the long term.
DEEP BITE TREATMENT PLAN
One of the objectives of the orthodontic treatment is to establish adequate and normal incisors vertical overbite, which may be obtained by intrusion of upper and lower incisors, leveling of the functional occlusal plane, extrusion of posterior teeth, and/or vestibularization of anterior teeth.1, 8-10
The factors that determine the treatment strategy are:
Etiology. Each case represents a unique situation; therefore, the therapeutic approach must respond to the nature of the problem and target, as much as possible, the origin of the discrepancy.11-13 Since vertical alterations are usually the consequence of discrepancies between vertical growth of the mandibular ramus and vertical dentoalveolar development, it is critical to verify whether deep bite is a consequence of vertical excess of the mandibular ramus, lack of vertical dentoalveolar development of the posterior teeth, excess of vertical dentoalveolar development of the anterior teeth, alteration of the incisors inclination, or a combination of all of the above.4, 8, 14
Age. In spite of the difficulties of predicting individual changes of the incisors vertical overbite through time,15 the studies on its natural development indicate that it increases between the ages of 9 and 12 years, and it remains relatively stable since the age of 12.16 The reason is that teeth eruption influences the level of vertical dentoalveolar development. This suggests that vertical control of anterior and posterior teeth eruption during the period of mixed dentition may be an adequate strategy for achieving an early and stable correction of deep bite, especially in patients with lower facial height reduction and counterclockwise mandibular rotation. Proceeding this way prevents significant alterations of the maxillaries’ tridimensional development, because anterior or posterior vertical control during growth favors the improvement of the maxillaries’ sagittal relationship. Additionally, early treatment reduces the performance of vertical orthodontic movements, which are more difficult to achieve and more unstable in adult patients.11, 17
Facial esthetics. According to the facial esthetics paradigm, the deep bite treatment plan must consider some aspects associated to facial profile and vertical skeletal pattern, as well as tooth display.
Facial profile and vertical skeletal pattern. in patients with concave profile, hypodivergent skeletal pattern, and reduced anteroinferior facial height, extrusive movements of the posterior teeth are suggested for deep bite correction. These movements must be done gradually to allow adequate neuromuscular adaptation and to reduce the risk of relapse.18
Conversely, in patients with convex profile, hyperdivergent skeletal pattern, vertical excess and increased display of the interlabial gap and incisors at rest, the orthodontic treatment must be focused on incisors intrusion and vertical control. Proceeding this way prevents posterior teeth extrusion, vertical dimension growth, backward retroposition of the mandible due to its clockwise rotation, and interlabial gap increase.8, 12, 18-20
Tooth display. the harmonious vertical projection of maxillary incisors is a fundamental objective of the orthodontic treatment, as it allows the conservation of an adequate lip-tooth relationship at rest and smile, according to the patient’s age and sex, keeping at the same time a consonant smile arch, where the anterosuperior teeth incisal edge follows the lower lip contour. As a general principle, it is often recommended to avoid deep bite correction by intrusion of the upper incisors, with preference for anteroinferior intrusion; this prevents reduction of the upper incisors display at rest—a situation that will be aggravated with age—. An exception to this is the increased display of incisors at rest and gingival smile, caused by true vertical dentoalveolar excess of the upper incisors and/or by a short upper lip.18, 19, 21-23
TREATMENT STRATEGIES
Extrusion of posterior teeth
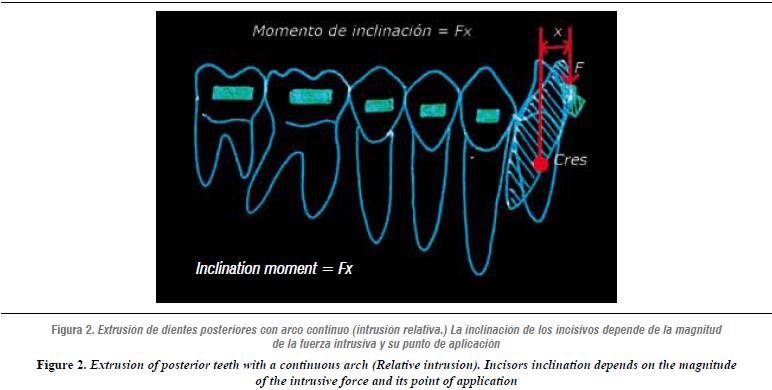
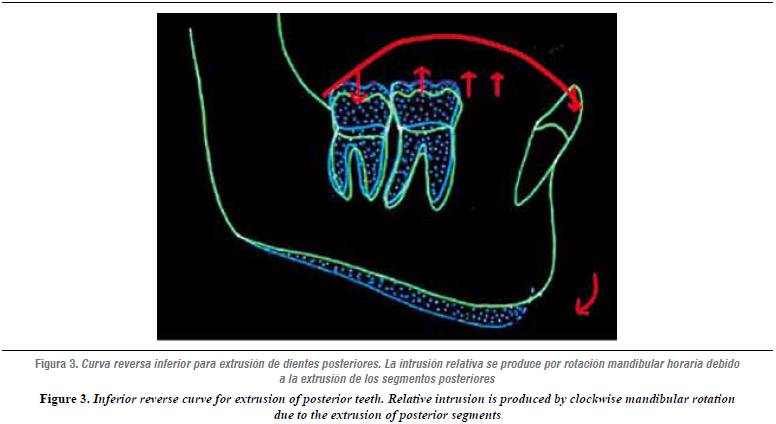
Continuous straight arches or arches with inferior inverse curve and superior accentuated curve. The result of continuous procedures is relative intrusion by a combination of posterior teeth extrusion and anterior teeth vestibularization, even if the arches are cinched.1, 11, 17, 29 The amount of vestibularization is proportional to the magnitude of the intrusive force28 (figures 2 and 3).
Extrusion arches. When only posterior extrusion is required, a biomechanics that minimizes incisors inclination during posterior extrusion must be used. This might be achieved with extrusion arches, which construction is identical to the intrusion ones, but offer greater forces and are usually made of steel.11, 27, 30-32 (figure 4).
Vestibularization of anterior teeth
Intrusion of anterior teeth
One of the methods used for deep bite correction is molar extrusion, as it is considered that 1 mm of posterior extrusion may be expressed in 1,5 to 2,5 mm of anterior vertical overbite reduction.18, 24 This approach is indicated for growing patients with reduced anteroinferior facial height, hypodivergency, increased Spee’s curvature, adequate or decreased display of incisors at rest, and redundant lips.
This biomechanics may also be considered as an alternative for patients who have stopped growing, although its application in adult patients is limited, due to the greater difficulty of achieving a true extrusive movement of posterior teeth, and because the strength of levator muscles may threaten stability.18, 24, 25
Even though the amount of extrusive movement that may be achieved is variable and greatly depends on the patient’s facial vertical dimension and its associated musculature, some authors point out that it may be between 1,47 and 2,8 mm.8, 26, 27
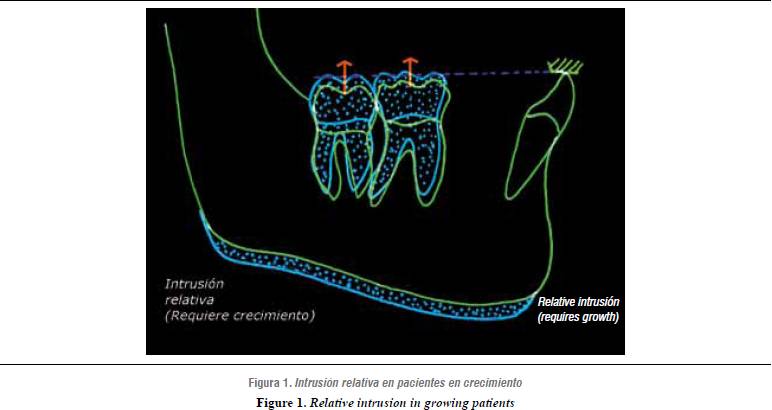
When used in patients with potential growth, posterior extrusion implies the use of anterior bite planes, which control eruption of anterior teeth while providing space for posterior teeth extrusion and thus for mandibular ramus growth, as well as clockwise mandibular rotation, a situation that favors leveling of the curve of Spee and increase of inferior facial height. These changes have been named relative intrusion.5, 9, 10, 19 (figure 1).
In permanent dentition, deep bite and a pronounced curve of Spee may also be corrected by posterior teeth extrusion. It is then necessary to use forces over 100 gr on each side, by using intermaxillary elastics, reverse curve arches or extrusion arches. Additionally, it may be useful to include anterior bite planes in order to unblock the posterior segment and facilitate extrusion.2, 11, 28
Posterior extrusive movements have been classified by Burstone like this: Type I when combined with counterclockwise rotation of the posterior segment (for example, when it is necessary to level a pronounced Curve of Spee) and Type II when the movement of posterior segments is completely parallel.11
The extrusive movement Type I may be achieved by means of two orthodontic mechanics:

On the other hand, the extrusive movement Type II may only be obtained by means of vertical intermaxillary elastics (or in the superior arch), combining extrusion arches with cervical (lower) extra-oral traction. In this situation, long and elevated lever-arm traction must be used so that the force’s line of action goes behind the center of resistance of the posterior segment, producing a moment in the opposite direction to the one produced by the extrusion arch; this way, the traction’s vertical vector and the extrusive arch produce parallel extrusion of the posterior teeth.
Vestibularization is an option that may result effective for the correction of mild to moderate deep bite with dental origin and with retroinclination of anterior teeth, as in the case of Class II division 2 malocclusion. In this case, incisor vestibularization reduces overbite, moving the contact point towards incisal.1, 5, 33 When vertical overbite is reduced by vestibularization, the incisors’ position and the interincisal angle must be kept at limits that allow balance of perioral muscles and the tongue, so that movement stability would not be threaten.2
Orthodontic correction of dentoalveloar deep bite by intrusion of the lower and/or upper incisors is indicated for cases presenting true overeruption of the incisors in patients with vertical dimension increase, excessive display of incisors at rest, gingival smile, or increased interlabial gap, it is, greater than 4 mm.5, 19
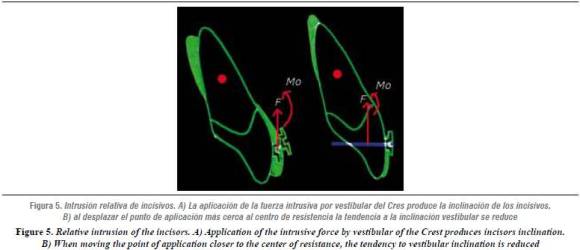
True intrusion is defined as the apical movement through the roots’ geometric center in relation to the occlusal plane.19 Even though intrusion is the adequate movement for correction of the deep bite associated with incisors overeruption, it is difficult to produce true intrusion and to calculate the amount of intrusive movement achieved, as only relative intrusion is usually obtained.12 This is explained by the difficulty of applying a vertical intrusive force that would pass through the incisors’ center of resistance and would produce its complete apical movement9 (figure 5).
Various studies have reported that intrusion of the incisors may be more efficient when using segmented arch techniques. Similarly, results of the meta-analysis published by Ng J in 2005 indicate that when using segmented techniques the possible amount of intrusion in the upper incisors is approximately 1,5 mm, and 1,9 mm in the lower ones.12 Moreover, other studies point out that it is possible to achieve up to 3 mm of intrusion.24, 29, 34, 35
The orthodontic procedure with segmented arches offers an advantageous alternative for intrusion of the anterior teeth, in comparison to the straight arch techniques, which may produce greater inclination of the incisors, as well as instability of the results.19
Different segmental techniques for anterior intrusion using auxiliary arches have been described by authors like Ricketts, Begg, Greig, and Burstone since the 1950s. In all of the cases, the auxiliary arches incorporate bends of crown inclination distal to the molars, thus exerting an intrusive force on the incisors.13, 19, 30, 31 In general, these authors suggest that the principal advantage of the intrusion arch is that it allows predicting the direction and magnitude of the forces on the teeth and their effects in the areas of action and reaction.19
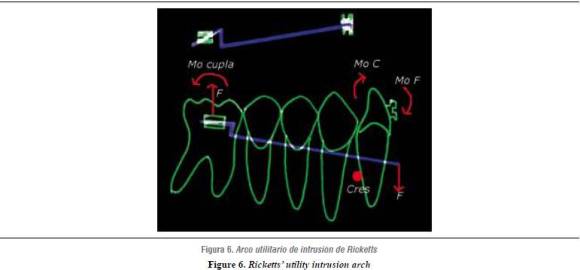
Since the 1970s, when it started to become popular, the utility arch described by Ricketts and its subsequent modifications have been used as an effective method of deep bite correction and Spee’s curvature leveling. Ricketts’ original design is made of stainless steel, it incorporates a bypass of premolars, and it is activated with a bend of distal inclination of crown (tip-back) over the molars. The difference with statically-determined intrusion systems is that Ricketts’ utility arch is adjusted inside the brackets slots, incorporating torques that may alter the expression of the vertical force and increase inclination of the incisors36 (figure 6).
STATICALLY-DETERMINED SYSTEMS OF INTRUSION
The systems of intrusion with segmented techniques consist of three elements: 1) Unit of posterior anchorage, which includes molars and premolars. Once the posterior segments have been aligned, they are stabilized with heavy arches and consolidated as a unit of anchorage. Transpalatal bars and lingual arches may also be used as part of anchorage or as extra-oral forces. 2) Anterior segment, consisting of the teeth to be intruded, and 3) auxiliary intrusion arch.19
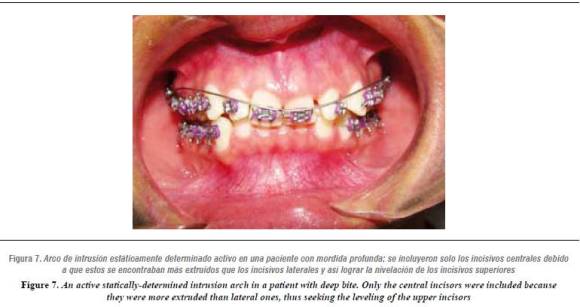
Intrusion arches are made of rectangular wires of steel or TMA. The latter allows elaboration of a simpler design and offers a greater working range thanks to its low load/deflection rate in comparison to steel.18 Design of the instrusion arch includes bends of inclination distal to the crown (tip-back) and mesial to the molars (approximately 2 mm from the auxiliary tube) to be pre-activated with an angle of 40-45°. With pre-activation, the arch inserted in the tubes remains passive at the anterior section at the level of the bottom of the sulcus; activation occurs when the arch is attached to the anterior segment, applying an intrusive force (figure 7).
Given that intrusion arches are not directly placed in the bracket slots, but apply their force at a specific point of the anterior segment, they are considered statically-determined systems, as they offer a greater control on the magnitude and direction of the applied forces.
A necessary condition for intrusion of the anterior segment is the teeth being aligned and leveled; nevertheless, when the incisors are not leveled and intrusion is required, the intrusive force must be applied selectively, only on the most extruded teeth, until leveling is achieved.11, 19
The statically-determined biomechanical intrusion system suggests several principles of movement control:1, 11, 19
Use constant forces with low magnitude: Intrusion is more efficient when using constant forces of lower magnitude; this can be achieved by using arches with low load-deflection rates. If the force magnitude is high, it may increase the rate of radicular resorption, as well as the effects of reaction in the anchorage area, it is, the tendency to extrude the posterior teeth altering the occlusal plane and constricting the maxillary arch.36 If the molar is used as the only anchorage unit, the unwanted reaction will be manifested as distal crown inclination. Recommended force magnitudes for intrusion are listed in (table 1).
Use contact points at the anterior region.
Control reaction using anchorage units at the posterior region.
Select the point of force application in relation to the center of resistance of the teeth to be intruded: In the case of the four incisors, the center of resistance is located distal to the lateral incisor. It is recommended to make canine intrusion individually, with a cantilever, because moving it requires increasing the force magnitude. Theoretically, intrusion forces going through the incisors’ center of resistance would produce intrusion, without a single change of the tooth’s axial inclination, but clinically the exact control of force application and its consequential movement are very complex. This is due to individual variability, which is defined by factors such as radicular anatomy and length, clinical crown/root proportion, periodontal support, and the tooth's axial inclination. This way, the spatial relation between the point of force application and the center of resistance may change according to the incisors inclination towards vestibular or lingual.11

Force steadiness is decisive for the efficiency of the intrusive movement and it depends on the system’s rank of work; this means that systems with a low load-deflection rate must be used, as they provide less force per millimeter of deactivation, and therefore require less activation.2, 13, 18, 19
Regarding force magnitude, a comparative study between Burstone’s intrusion arch and Rickkets’ utility arch found out that arches activated with a tipback of 45° generate forces at the physiological levels, while Burstone’s arches made of TMA (0,017 x 0,025) produce less force and less anterior moment than the utility arches made with the same alloy and dimensions37, 38
SYSTEMS OF INTRUSION WITH MINI-IMPLANTS
The use of mini-implants as anchorage for producing intrusive movements allows controlling the collateral effects on the anchorage produced by the continuous archwire and segmented archwire techniques.39, 40
Additional advantages of using mini-implants as anchorage include their simple installation and removal, which do not require surgical procedures, and their immediate insertion; also, the patient’s cooperation is reduced to adequate plaque control.40, 41 Furthermore, application of low and continuous forces when using segmented intrusion techniques with mini-implants has revealed low apical resorption rates (0,5-0,6 mm).42, 43
Due to the relatively new adoption of mini-implants as an orthodontic anchorage technique, most of the literature on its application consists on case reports; based on this information, we can conclude that the intrusion rate for the incisors is between 3 and 6 mm.44-48
There exist two basic mechanisms of intrusion with the use of mini-implants:
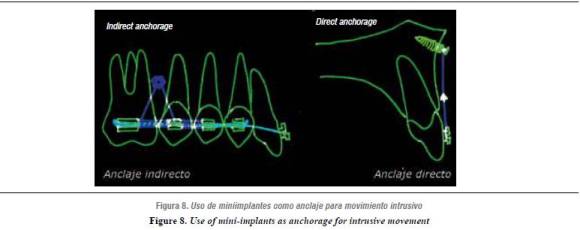
Direct anchorage. it applies a direct and unique force from the implant. This force may be supplied with elastomers or NiTi closed springs, and it is effective for achieving intrusive movement.49 Nevertheless, this mechanism produces uncontrolled inclination, therefore the incisors’ axial inclination, as well as the desired positioning of the radicular apex, must be carefully evaluated. Consequently, it is regarded as a useful alternative when attempting to intrude the incisors only, and when they are lingualized. If only the incisors need to be intruded, the implant must be placed between the central incisors, but if all the six anterior teeth are to be intruded, the mini-implants must be placed mesial to the canines, or distal to them if a retraction vector increase is required by making both movements simultaneously.Indirect anchorage. incorporating the implant to the anchorage unit is an adequate strategy for improving the efficiency of both the intrusion arch and the continuous arch systems, by controlling the reaction forces and their collateral effects. This technique implies the construction of an accessory of steel wire (0,016 x 0,022) that allows attaching the implant to the teeth of anchorage as a splint, opposing the anchorage’s extrusive movement (figure 8).
FINAL CONSIDERATIONS ON INTRUSIVE MOVEMENT
According to the studies by Burzin & Nanda, deep bite correction stability increases when intrusion is made at the maxillary arch with statically-determined systems. After an overbite reduction of 3,5 mm during treatment, a relapse of about 0,8 mm (22%) may be expected. Similarly, the studies made by Berg, Deck & Sinclair and Simmons agree with these findings by claiming that the percentage of relapse is about 20-40%.29 In general, deep bite correction with intrusion of the incisors is more stable than the ones that include leveling of the occlusal plane with extrusion of the molars.10
Evidently, the risk of relapse is variable and may increase depending on the level of proinclination produced during treatment, the remaining mandibular growth, the interincisal angle, the magnitude of the correction, and periodontal health.25 The latter is an important factor that may threaten control of the intrusive movement and its stability because, on the one hand, the intrusive movement may imply transportation of supragingival plaque towards the subgingival zone, and, on the other hand, in patients with periodontal support lost, intrusion might improve the relationship of the crown to the gingival margin, without this meaning improvement of the crown/root proportion at the level of the bony intersection, and therefore the risk of relapse increases and the periodontal disease progresses.50
CONCLUSIONES
- Orthodontic treatment of deep bite implies the application of three strategies: Posterior teeth extrusion, anterior teeth true or relative intrusion, and incisors vestibularization.
- The treatment approach must match each patient’s specific needs in terms of facial esthetics, dentoalveolar relationships, occlusal plane, and skeletal pattern.
- Esthetic evaluation of tooth display is a critical consideration at the time of planning the therapeutic strategy for deep bite correction.
- Stability of deep bite correction depends on the movement used during therapy: extrusion, proinclination, or intrusion. In general, the findings of most of the studies reveal certain level of relapse, regardless of the technique used.
ACKNOWLEDGEMENTS
To Doctor Diana Barbosa, professor of the Especialización Clínica en Odontología Integral del Adolescente y Ortodoncia, for her advice and support during the topic review and elaboration of this article.
1. Nanda R, Kuhlberg A. Manejo de la maloclusión de sobremordida profunda. In: Nanda R. Biomecánicas y estética. Amolca: Bogotá; 2007, pp.131-155. [ Links ]
2. Proffit W, Fields H. Ortodoncia contemporánea, teoría y práctica. Madrid: Harcourt; 2001. [ Links ]
3. Dermaut L, De Pau G. Aspectos biomecánicos de la mecánica de Clase II, con especial énfasis en la corrección de la mordida profunda como parte del objetivo de tratamiento. En: Nanda R. Biomecánica en ortodoncia clínica. Buenos Aires: Panamericana; 1998. pp. 79-89. [ Links ]
4. Bjork A. Prediction of mandibular growth rotation. Am J Orthod 1969; 55(6): 585-599. [ Links ]
5. Nanda R. The differential diagnosis and treatment of excessive overbite. Dent Clin North Am 1981; 25(1): 69-84. [ Links ]
6. Karlsen A. Craniofacial characteristics in children with Angle Class II div.2 malocclusion combined with extreme deep bite. Angle Orthod 1994; 64(2): 123-130. [ Links ]
7. Wong R. Combined orthodontic-dentofacial orthopedic treatment of a Class II Division 2 patient with severe deep bite. J Orthod 2002; 29(3): 181-188. [ Links ]
8. Parker C, Nanda R, Currier G. Skeletal and dental changes associated with the treatment of deep bite malocclusion. Am J Orthod Dentofacial Orthop 1995; 107(4): 382-393. [ Links ]
9. Proffit W. The first stage of comprehensive treatment. En Proffit W. Contemporary orthodontics. St Louis: Mosby, 2007. p. 570-576. [ Links ]
10. Al-Buraiki H, Sadowsky C, Schneider B. The effectiveness and long-term stability of overbite correction with incisor intrusion Mechanics. Am J Orthod Dentofacial Orthop 2005; 127: 47-55. [ Links ]
11. Burstone C, Steenbergen E, Hanley K. Deep overbite correction. En Burstone C, Steenbergen E, Hanley K. Modern edgewise mechanics & the segmented arch tecnhhique. USA: Ormco Corporation; 1995. p 33-48. [ Links ]
12. Ng J, Major P, Heo G, Flores-Mir C. True incisor intrusion attained during orthodontic treatment: a systematic review and meta-analysis. Am J Orthod Dentofacial Orthop 2005; 128: 212-219. [ Links ]
13. Nanda R, Marsban R y Kuhlberg A. The Connecticut intrusion arch. J Clin Orthod 1998; 32(12): 708-715. [ Links ]
14. Schudy F: The rotation of the mandible resulting from growth; its implications in orthodontic treatment. Angle Orthod 1965; 35: 36-50. [ Links ]
15. Moorrees C, Gron A, Lebret L, Yen P, Fröhlich F. Growth studies of the dentition: A review. Am J Orthod 1969; 55(6): 600-616. [ Links ]
16. Fleming H. Investigation of the vertical overbite during the eruption of the permanent dentition. Angle Orthod 1961; 31: 53-62. [ Links ]
17. Braun S. Biomechanical considerations in the management of vertical dimension. Semin Orthod 2002; 8: 149-154. [ Links ]
18. Nanda R. Correction of deep overbite in adults. Dent Clin North Am 1997; 41(1): 67-87. [ Links ]
19. Burstone CJ. Deep overbite correction by intrusion. Am J Orthod 1977; 72(1): 1-22. [ Links ]
20. Levin R. Deep bite treatment in relation to mandibular growth rotation. Eur J Orthod 1991; 13(2): 86-94. [ Links ]
21. Burstone C. Lip posture and its significance in treatment planning. Am J Orthod 1967; 53(4): 262-284. [ Links ]
22. Zachrisson B. Esthetic factors involved in anterior tooth display and smile: vertical dimension. J Clin Orthod 1998; 32(7): 432-445. [ Links ]
23. Lindauer S, Lewis Sh, Shroff B. Overbite Correction and Smile Aesthetics. Semin Orthod 2005;11: 62-66. [ Links ]
24. Otto R, Anholm J, Engle G. A comparative analysis of intrusion of incisor teeth achieved in adults and children acording to facial type. Am J Orthod 1980; 77: 437-446. [ Links ]
25. Burzin J, Nanda R. The stability of deep overbite correction. En: Burstone C, Nanda R. Retention and stability in orthodontics. Philadelphia: Saunders; 1993. p. 61-79. [ Links ]
26. Dahl B, Krogstad O. The effect of a partial bite-raising splint on the inclination of upper and lower front teeth. Acta Odontol Scand 1983; 41: 311-314. [ Links ]
27. Bernstein R, Preston Ch, Lampasso J. Leveling the curve of Spee with a continuous archwire technique: A long term cephalometric study. Am J Orthod Dentofacial Orthop 2007;131: 363-371. [ Links ]
28. Braun S, Hnat W, Johnson B. The curve of spee revisited. Am J Orthod Dentofacial Orthop 1996; 110: 206-210. [ Links ]
29. Dake M, Sinclair P. A comparison of the Ricketts and Tweed-type arch leveling techniques. Am J Orthod Dentofacial Orthop 1989; 95(1): 72-78. [ Links ]
30. Shroff B, Yoon W, Lindauer S, Burstone C.Simultaneous intrusion and retraction using a three-piece base arch. Angle Orthod 1997; 67(6): 455-461. [ Links ]
31. Burstone C. Rationale of the segmented arch. Am J Orthod 1962; 48: 805-822. [ Links ]
32. Weiland F, Bantleon HP, Droschl H. Evaluation of continuous arch and segmented arch leveling techniques in adult patients ,a clinical study. Am J Orthod Dentofacial Orthop 1996; 110: 647-652. [ Links ]
33. Ball J, Hunt N. The effect of Andresen, Harvold, and Begg treatment on overbite and molar eruption. Eur J Orthod 1991; 13(1): 53-58. [ Links ]
34. Gottlieb B. The effect of an intrusive base arch on tooth position: a radiographic study. [Tesis]. Farmington: University of Connecticut; 1979. [ Links ]
35. Greig D. Bioprogressive therapy: Overbite reduction with the lower utility arch. Br J Orthod 1983; 10: 214-216. [ Links ]
36. Davidovitch M, Rebellato J. Two couple orthodontic appliance system utility arches: two couple intrusion arch. Semin Orthod 1995; 1(1): 25-30. [ Links ]
37. Steenbergen E, Burstone J, Prahl-Andersen B, Aartman A. The Influence of Force Magnitude on Intrusion of the Maxillary Segment. Angle Orthod 2005; 75: 723-729. [ Links ]
38. Sifakakis I, Pandis N, Makou M, Eliades T, Bourauel C. Forces and moments generated with various incisor intrusion systems on maxillary and mandibular anterior teeth. Angle Orthod 2009; 79: 928-933. [ Links ]
39. Ohnishi H, Yagi T, Yasuda Y, Takada K. A mini implant for orthodontic anchorage in a deep overbite case. Angle Orthod 2005; 75: 393-401. [ Links ]
40. Lee J, Kim J, Park Y, Vanarsdall R. Vertical control: Anterior intrusión. En Lee J, Kim J, Park Y, Vanarsdall R. Applications of orthodontic mini-implants. Chicago: Quintessence 2007. p. 217-226. [ Links ]
41. Papadopoulos M, Tarawneh F. The use of miniscrew implants for temporary skeletal anchorage in orthodontics: A comprehensive review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007; 103: e6-e15. [ Links ]
42. Ari-Demirkaya A, Masry M, Erverdi N. Apical root resorption of maxillary first molars after intrusion with zygomatic skeletal anchorage. Angle Orthod 2005; 75: 761-765. [ Links ]
43. Carrillo R, Buschang P, Opperman L, Franco P, Rossouw E. Segmental intrusion with mini-screw implant anchorage: A radiographic evaluation. Am J Orthod Dentofacial Orthop 2007; 132: 576e1-576e6. [ Links ]
44. Creekmore T, Eklund M. The possibility of skeletal anchorage. J Clin Orthod 1983: 266-269. [ Links ]
45. Kanomi R. Mini-Implant for orthodontic anchorage. J Clin Orthod 1997; 31(11): 763-767. [ Links ]
46. Deguchi T, Takashi M, Kuroda S, Yabuuchi T, Kamioka H, Yamamoto T. Comparison of the intrusion effects of the maxillary incisors between implant anchorage and J-hook headgear. Am J Orthod Dentofacial Orthop 2008; 133: 654-660. [ Links ]
47. Paik C, Woo Y, Boyd R. Treatment of an adult patient with vertical maxillary excess using miniscrew fixation. J Clin Orthod 2003; 37: 423-428. [ Links ]
48. Carano A, Velo S, Incorvatti C, Poggio P. Clinical applications of the mini-screw anchorage system (MAS) in the maxillary alveolar bone. Prog Orthod 2004; 5: 212-235. [ Links ]
49. Cope J. Temporary anchorage devices in orthodontics: A paradigm shift. Semin Orthod 2005; 11: 3-9. [ Links ]
50. Melsen B. Intrusion of incisors in adult patients with marginal bone loss. Am J Orthod Dentofacial Orthop 1989; 96: 232-241. [ Links ]

