










Services on Demand
Journal
Article
 text in
text in  Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
Print version ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.23 no.2 Medellín Jan./June 2012
ORIGINAL ARTICLES DERIVED FROM RESEARCH
Dental caries and treatment needs in 12-year-old schoolchildren from public institutions of the municipality of Rionegro (Antioquia, Colombia), 20101
Annie Vivares Builes2; Andrés F. Saldarriaga Saldarriaga2; natalia Muñoz Pino2; Marisol Miranda Galvis2; Kelly Colorado Colorado2; Yenny P. Montoya Zuluaga 2; Yomaira Viñas Sarmiento3; Andrés Agudelo Suárez4
1 Research project carried out as an academic exercise at the
Universidad de Antioquia's Dentistry Graduate Program by the first
six authors
2 Senior students at the Universidad de Antioquia's Dentistry Graduate
Program
3 Dentist, MA in Public Health, Assistant Professor, Facultad de
Odontología, Universidad de Antioquia. E-mail address: yoma.udea@gmail.com
4 Dentist, Specialist in Health Services Administration, PhD in Public
Health, Assistant Professor, Facultad de Odontología, Universidad de
Antioquia. Medellín, Colombia. E-mail address: oleduga@gmail.com
SUBMITTED: NOVEMBER 8/2011 16/2011 - ACCEPTED: FEBRUARY 14/2011
Dental caries and treatment needs in 12-year-old schoolchildren from public institutions of the municipality of Rionegro (Antioquia, Colombia), 2010.
ABSTRACT
INTRODUCTION: analyzing dental caries conditions of 12-year-old population allows verifying how much of the oralhealth
related goals have been achieved. The objective of this study was to describe the experience and prevalence of dental caries and
treatment needs of 12-year-old school children in the municipality of Rionegro.
METHODS: this was a cross-sectional descriptive study
on 808 schoolchildren aged 12 years from public schools of the municipality of Rionegro. Both traditional (T) and modified (M) decayed,
missing and filled teeth indexes (DMFTT and DMFTM) were used, as well as the Significant Caries Index (SiC). The obtained data were
analyzed according to gender, education level, place of residence, and health insurance status.
RESULTS: the DMFTT value among the
studied population was 1.70 (± 1.63) and the DMFTM was 2.19 (± 1.92). The prevalence of cavitated caries lesions was 59.9%, and
for all the lesions it was 70.8%. Caries experience for the DMFTT was 69.9%, and 77.8% in the case of DMFTM. The SiC measured according to the DMFTT was 3.60, and 4.42 for DMFTM. Significant differences were observed in terms of experience, prevalence and
treatment needs, especially in relation to gender and school grade.
CONCLUSIONS: these values indicate accomplishment of the goals
set by the WHO and by Colombian standards. Nevertheless, they also reveal some inequalities that must be considered when planning
promotion, prevention and attention programs aimed at this population.
Key words: dental caries, schoolchildren, DMFT standards, Significant Caries Index.
INTRODUCTION
Dentists make many efforts to prevent, treat, and control dental caries. This is a complex multifactorial disease affecting people at any age, regardless of race and sex, and it is therefore considered a public health issue all around the world due to its high prevalence.1, 2 Also, this oral disease produces numerous effects including pain, distress, function deterioration, and a reduced quality of life, that may be enormous and costly.1-3 The cost of oral diseases treatment is thought to be between 5 to 10% of industrialized countries public health expenses, and it is beyond the resources of many underdeveloped countries.1-4 Therefore, detailed information on the oral health conditions at the national, regional and international levels seems to be important as it would allow assessing changes and tendencies over time; also, performing epidemiological monitoring would provide solid bases for definition and evaluation of public health policies at the local, regional, national and international levels 4, 5
In Colombia, scientific evidence on dental caries indexes among 12-year-old population has demonstrated an evident decrease according to the international goals set by the WHO and the FDI,6 as well as by the standards of Estudios Nacionales de Salud Bucal (Oral Health National Studies) and their figures of dental caries prevalence and history (DMFT), which show a decrease in the last 40 years from 7.1 in 1966,7 to 4.8 in 1977,8 and 2.3 in 19989 for this population. This implies reinforcing oral health public policies in the country. The oral health situation in Colombia is similar to that of other Latin American countries.10-14
Nevertheless, the diverse studies and official reports also point out that there exist some specific population groups with poorer oral health conditions in comparison to the general population, evidencing inequalities related to life standards, access to oral health services and, in general, to the social determinants of health.15, 16 Some reports refer to concepts such as polarization of dental caries,17 as 75% of the cases occur in 25% of the population, although with some differences among age groups.18
Specifically in the municipality of Rionegro, its Health Department has established some guidelines included in the city's 2008-2011 Development Plan,19 in agreement with Decree 3039 of 2007, which states the National Plan of Public Health.20 Its baseline is the oral health situation of 12-year-old population as it is a group in which all permanent teeth have already erupted thus allowing assessments based on the goals set by the Plan, which include, for instance, achieving an average DMFT index of 2.3 by the age of 12, and maintaining 60% of permanent teeth in the population over 18.20
The objective of this study was then to describe the experience and prevalence of dental caries and the treatment needs of 12-year-old schoolchildren in the municipality of Rionegro.
METHODS
This was a cross-sectional descriptive study. The data were obtained from the Health Department of the municipality of Rionegro during the year 2010. The information was gathered by means of epidemiological screenings in 16 official schools by a dentist who was standardized by the same Department in order to perform the field work. This study mainly took into account the goals of Rionegro's 2008-2011 Development Plan,19 in which oral health is one of the ten top health priorities, considering the importance of health promotion and disease prevention actions, closely connected to municipal competences of the National Plan of Public Health in 2007.20
The following variables were considered for this study: 1) decayed, missing and filled teeth index (DMFT) by Klein and Palmer,21 either traditional (DMFTT) or modified (DMFTM)—modification consisted on including active non-cavitated lesions;22 2) significant caries index (SiC);23 analysis of the dental caries situation in many countries has demonstrated the existence of biased DMFT distribution. This is why the SiC was included, as it consists on calculating the average DMFT in the most affected third of the population, which in this case was calculated based on the DMFTT and the DMFTM, by means of spreadsheet formulas available at: http://www.mah.se/ CAPP/Methods-and-Indices/for-Caries-prevalence/ Significant-Caries-Index/Online-Calculation-of- DMFTdmft-and-SIC-Index-/; 3) both dental caries prevalence and dental caries experience were calculated by means of the DMFTT and DMFTM index (for all the lesions and the cavitated ones). Sociodemographic variables included: sex, school grade (first to fifth grade of primary school, and sixth grade of high school); area of residence (urban-rural), and access to public health system (Sistema General de Seguridad Social en Salud, SGSSS).
Uni- and bivariate analyses were performed: calculations of averages (standard deviation) and absolute/ relative frequencies were performed both in a general way and for each of the socio-demographic variables. Mann-Whitney and Kruskal Wallis nonparametric U tests were conducted as well as Chisquared tests for difference in proportion, in order to observe statistical significance among the variables. Data analysis was carried out by means Excel® for Windows®, SPSS® 18.0 (Chicago IL.USA) and EPIDAT 3.1® (Dirección Xeral de Innovación e Xestión da Saúde Pública, Xunta de Galicia, España, Organización Panamericana de la Salud e Instituto Superior de Ciencias Médicas de La Habana).
This research project complied with the ethic requirements in health research by Resolution 008430 of Ministerio de la Protección Social (former Ministerio de Salud - Colombia), making use of the protocols of dental examination, informed consent, protection of the children's identity, and veracity of the information.
The present analysis made use of secondary data from the municipality of Rionegro Health Department. This research project was approved as an academic exercise of the six first authors in the Dentistry Undergraduate Program at Universidad de Antioquia, Medellín, Colombia.
RESULTS
Table 1 shows the variable distribution of the studied population as well as the DMFT index and its different components. In general, females present a higher average of non-cavitated caries; on the contrary, cavitated caries are more common in males. In both cases the differences were statistically significant (p < 0.05). In terms of the DMFTT average, it is higher in males. Regarding school grade, a tendency towards a decrease in the average of decayed teeth (both cavitated and non-cavitated) was observed as the grade increases. No significant average differences were found regarding place of residence (in relation to the average of cavitated decayed teeth, non-cavitated decayed teeth and DMFT). The analysis showed that the average of non-cavitated decayed teeth, cavitated decayed teeth and DMFT (both traditional and modified) is higher in those children who are not covered by social security, although the differences were not significant.
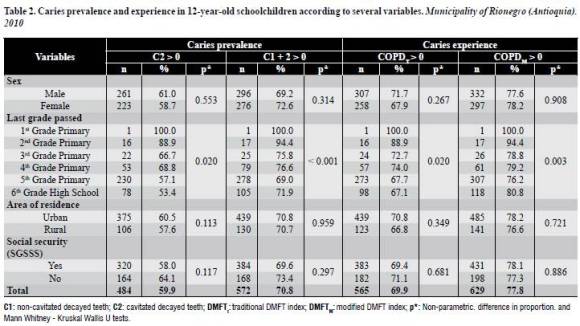
Analysis of dental caries prevalence and experience among this population (table 2) shows that prevalence of dental caries, including non-cavitated lesions, is 71 and 60%, taking into account only teeth with cavitated caries. Caries experience is 70% or greater. Lower dental caries prevalence and experience were observed in higher school grades, with statistical significant difference (p < 0.05). No significant differences were observed by gender, area of residence or access to public health services: nevertheless, both prevalence and experience were slightly higher in urban areas and in kids who are not covered by the SGSSS.
Analysis of the average DMFT in the most affected third of the population (SiC — table 3), shows that the average is 3.61 when calculated based on the DMFTT, and 4.42 in the case of DMFTM.
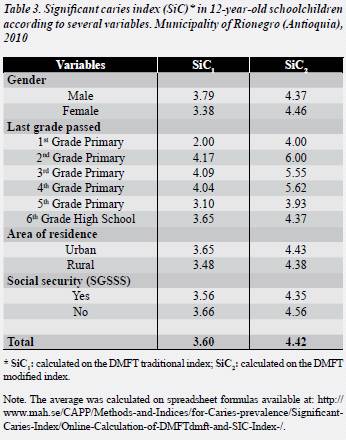
The same tendencies are observed in the presentation of these variables; the SiC measured based on the DMFTT is greater in men, and when calculated based on the DMFTM it is greater in women. The SiC decreases as the school grade increases, being second grade the one with the most prevalence (4.2 and 6.0 for DMFTT and DMFTM, respectively). Finally, the SiC index was greater in kids living in the rural area and in population without social security coverage.
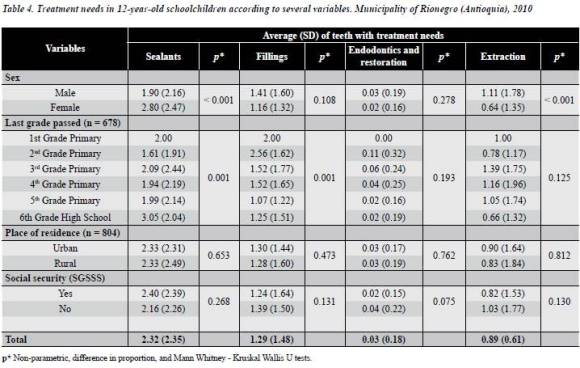
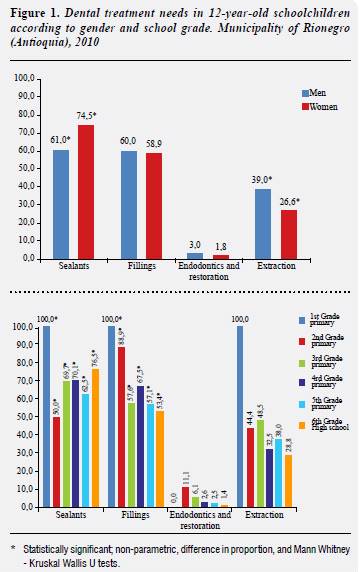
Concerning treatment needs among this population (table 4 and figure 1) , the analysis showed that the number of teeth in need of filling, endodontic treatment and extraction is greater in males (with significant difference in the case of extractions). Females presented greater need of sealants than males and significant differences were observed (p < 0.05). No significant differences of this kind of needs were found regarding place of residence or access to social security (SGSSS). As school grade increases the needs of sealants increase and the needs of fillings decrease.
DISCUSSION
The results of this study show significant differences in terms of the DMFT index regarding sex and school grade, and non-significant differences in relation to place of residence and social security coverage (SGSSS). The same situation occurred with respect to dental caries prevalence and experience and treatment needs. As school grade increases treatment needs decrease; differences were found by sex, and the most prevalent treatment need was preventive restorations and other kinds of restorative treatment.
This information allowed making national and international comparisons on the oral situation of kids of the municipality of Rionegro in relation to different socio-demographic factors.
Comparisons of the data obtained in the municipality of Rionegro and the III Estudio Nacional de Salud Bucal9 with the goals set by the WHO and international standards1, 2, 6 showed that both DMFTT and DMFTM are lower in the evaluated population. Nevertheless, comparisons of the baseline screening of the DMFT indicator of 12-year-old kids conducted in 2009 by the municipality of Rionegro with the support of Empresa Social del Estado Hospital Gilberto Mejía Mejía24 shows an increase in two of the parameters: caries (non-cavitated and cavitated) and restored teeth. Non-cavitated caries shows an average of 0.07 in comparison to the current 0.49.
Cavitated caries showed an average of 0.14 in contrast to 1.26 in 2010. Thirdly, restored teeth presented an average of 0.32 against 0.44 in the present study. Conversely, the variable of teeth loss because of caries does not vary (0.01). All these changes in the variables analyzed lead to an increased total DMFT index in time, arising from 0.54 in 2009 to 2.19 in 2010. Current results for the urban area (DMFTT of 1.74 (± 1.63) were slightly higher than in another study carried out in the urban area of Rionegro in 1999 (DMFT 1.23 IC95% 1.14-1.32).25
Some inequalities may be observed for some groups when analyzing other variables such as SiC, which was 3.6 measured from DMFTT and 4.4 based on DMFTM (values greater than 3, which is the objective of the WHO for the year 2015). In the case of Significant Caries Index (SiC), big differences were found when comparing the data of the 12-year-old population under study with that of other countries, for example: SiC of 2.5 in Brazil,26 4.1 in Nicaragua,11 2.3 and 19.8 in two localities of Mexico,27 and 1.8 in Spain.28
Although some differences in socio-demographic characteristics were observed, the results must be carefully interpreted. It would be necessary to perform further analysis with multidisciplinary approaches including not only structural determinants but also oral health components in different populations; some other aspects such as culture, history and politics of the country and its different regions should also be included.15, 16
The absence of significant differences in dental caries variables among schoolchildren in the urban and rural areas in the municipality of Rionegro may suggest that social structure and resource distribution between these populations is equitable. In some cases, the variables were better in rural areas; it is then important to include, as part of the explanation, the availability of a diet with higher contents of sugars in urban areas.29, 30Another possible explanation may be related to previous specific prevention programs in Rionegro, where programs and strategies of intervention in oral health have been promoted in rural areas.19, 31
Differences in caries distribution between males and females were found, with higher prevalence of lesions of incipient caries in females and cavitated caries in males. Further studies would require analysis by sex in order to incorporate new variables that allow analyzing diverse determinants such as gender32, 33or social class.34-36 The differences observed in terms of education level may be explained by the capacity of school children to better understand the oral component of the healthdisease process thus reinforcing self-care practices.37 Finally, access to oral health services and global coverage of the curative and preventive programs carried out by the SGSSS in Colombia plays an important role in dental caries prevalence, as it is higher in those schoolchildren without coverage.5
It is important to mention the strengths and limitations of this study. It included a sufficient sample of 12-year-old schoolchildren from official schools of the municipality of Rionegro, which allowed having enough knowledge of the global context of both dental caries situation and treatment needs of the schoolchildren under study. It is also important to point out that the data were collected by trained professionals, and that several variables were analyzed in order to interconnect them with the social determinants of health. The limitations of this study have to do with numeric representation of some variables, such as education level, so the results may be under- or overestimated. Also, no information from private schools of Rionegro was available, which would have enabled comparisons and further analysis.
The information obtained in this study must be complemented with further studies that include other variables such as the parents' education levels, as well as knowledge, attitudes, practices, and nutritional evaluation. It should also assess other risk factors for caries, such as political factors or belonging to a given ethnic group, and include other age groups, in order to thoroughly approach the determinants that influence dental caries prevalence and experience. It is important to plan and carry out an oral health program that meets the treatment needs of the studied population, and to implement preventive strategies compatible with the results obtained in this study and the ones previously made in this town.
Finally, the knowledge on oral health must be improved by means of education programs in the schools, and strategies for improving oral health conditions among the school population must include not only prevention but also rehabilitation, monitoring and constant evaluation of oral health policies and strategies aimed at this population.
ACKNOWLEDGEMENTS
To the Health Department of the municipality of Rionegro for providing the data for this study. To professors Hugo Sánchez, Gonzalo Álvarez and Tomás Bernal for their intellectual contributions to the development of this research project.
CORRESPONDING AUTHOR
Annie Vivares Builes
Andrés A. Agudelo Suárez
Facultad de Odontología
Universidad de Antioquia
Calle 64 N.° 52-59
Teléfono: +57(4) 219 67 40
Medellín, Colombia
Correos electrónicos: annievivares@gmail.com
oleduga@gmail.com
REFERENCES
1. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ 2005; 83 (9): 661-669. [ Links ]
2. Organización Mundial de la Salud. World Oral Health Report 2003. Continuous improvement of oral health in the 21st century - the approach of the WHO Global Oral Health Programme. Ginebra: Organización Mundial de la Salud; 2003. [ Links ]
3. Edelstein BL. The dental caries pandemic and disparities problem. BMC Oral Health 2006; 15(6) supl. 1: S2. [ Links ]
4. Franco ÁM, Ochoa E, Martínez E. Reflexiones para la construcción de política pública con impacto en el componente bucal de la salud. Rev Fac Odontol Univ Antioq. 2009; 15(2): 78-90. [ Links ]
5. Agudelo-Suárez AA, Martínez-Herrera E. La salud bucal colectiva y el contexto colombiano: Un análisis crítico. Revista Gerencia y Políticas de Salud 2009; 8 (16): 91-105. [ Links ]
6. Organización Mundial de la Salud/Federación Dental Internacional. Metas de Salud Bucal para el año 2000. Ginebra: Organización Mundial de la Salud; 1979. [ Links ]
7. Colombia. Ministerio de Salud-Asociación Colombiana de Facultades de Medicina-Ascofame. Morbilidad Oral. Investigación Nacional de Morbilidad. Estudio de Recursos Humanos para la Salud y la Educación Médica en Colombia. Bogotá: El Ministerio, Ascofame; 1971. [ Links ]
8. Colombia. Ministerio de Salud-Instituto Nacional de Salud. Ascofame. Morbilidad Oral. II Estudio Nacional. Bogotá: El Ministerio, Instituto Nacional de Salud; 1980. [ Links ]
9. Colombia. Ministerio de Salud. III Estudio Nacional de Salud Bucal ENSAB III, 1998. Bogotá: Ministerio de Salud; 1998. [ Links ]
10. Villalobos-Rodelo JJ, Medina-Solís CE, Molina-Frechero N, Vallejos-Sánchez AA, Pontigo-Loyola AP, Espinoza- Beltrán JL. Caries dental en escolares de 6 a 12 años de edad en Navolato, Sinaloa, México: experiencia, prevalencia, gravedad y necesidades de tratamiento. Biomédica 2006; 26(2): 224-233. [ Links ]
11. Herrera MS, Medina-Solis CE, Maupomé G. Prevalencia de caries dental en escolares de 6-12 años de edad de León, Nicaragua. Gac Sanit 2005; 19(4): 302-306. [ Links ]
12. Márquez Filiú M, Rodríguez Castillo RA, Rodríguez Jerez Y, Estrada Pereira G, Aroche Arzuaga A. Epidemiología de la caries dental en niños de 6-12 años en la Clínica Odontológica La Democracia. Medisan 2009; 13(5): 1-5. [ Links ]
13. Colina Sánchez Y, García Alpízar B, Castillo Betancourt EM, Benet Rodríguez M, López Fernández R, Rodríguez Rodríguez M. Estudio epidemiológico de salud bucal en la población de 12 años del área VIII de salud de Cienfuegos. Medisur 2007; 5(2): 44-53. [ Links ]
14. Mejía Pineda M, Castro Rodríguez A, Watanabe Velásquez R, Chein Villacampa, Ventocilla Huasupoma M. Necesidades de tratamiento para caries dental en escolares de zonas urbano y urbano marginal de Lima. Odontol Sanmar 2000; 1(6): 26-32. [ Links ]
15. Borrell C, Malmusi D. La investigación sobre los determinantes sociales y las desigualdades en salud: evidencias para la salud en todas las políticas. Informe Sespas 2010. Gac Sanit 2010; 24 Supl. 1: 101-108. [ Links ]
16. World Health Organization. A conceptual framework for action on the social determinants of health. Geneva: World Health Organization; 2010. [ Links ]
17. Narvai PC, Frazão P, Roncalli AG, Antunes JLF. Cáriedentária no Brasil: declínio, iniqüidade e exclusão social. Rev Panam Salud Pública 2006; 19(6): 385-393. [ Links ]
18. Macek MD, Heller KE, Selwitz RH, Manz MC. Is 75 percent of dental caries really found in 25 percent of the population? J Public Health Dent 2004; 64(1): 20-25. [ Links ]
19. Municipio de Rionegro. Plan de Desarrollo para el periodo 2008-2011: Gobernar es Educar. [en línea] 2008 [fecha de acceso 26 de marzo de 2011] URL disponible en: http://www.rionegro.gov.co/images/stories/nuestra_administracion/plan_desarrollo_2008_2011.pdf [ Links ]
20. Colombia. Ministerio de la Protección Social. Decreto 3039 de 2007. Plan Nacional de Salud Pública. Bogotá: El Ministerio, 2007. [ Links ]
21. Klein H, Palmer CE; Knutson JW. Studies on Dental Caries, I, Dental status and Dental Needs of elementary school. Public Health Report 1938; 53: 751-765. [ Links ]
22. Pitts NB, Deery C, Fyffe HE, Nugent ZJ. Caries prevalence surveys a multi-country comparison of caries diagnostic criteria. Community Dental Health 2000; 17: 196-203. [ Links ]
23. Bratthall D. Introducing the significant caries index together with a proposal for a new global oral health goal for 12-yearolds. Int Dent J 2000; 50: 378-384. [ Links ]
24. Viñas Sarmiento Y, Álvarez Gómez MR. Programa de Salud Bucal Rionegro Antioquia. Revista Salud Vital 2010; 3: 24-27. [ Links ]
25. Sierra JL. Prevalencia de caries y fluorosis dental en escolares de 12 años zona urbana del municipio de Rionegro- 1999. [Trabajo de grado: Especialista en Epidemiología]. Medellín: CES; 1999. [ Links ]
26. Piovesan C, Mendes FM, Antunes JLF, Machado Ardenghi T. Inequalities in the distribution of dental caries among 12-year-old Brazilian schoolchildren. Brazilian Oral Research 2011; 25(1): 69-75. [ Links ]
27. Martínez-Pérez KM, Monjarás-Ávila AJ, Patiño-Marín N, Loyola-Rodríguez JP, Mandeville PB, Medina-Solís CE et al. Estudio epidemiológico sobre caries dental y necesidades de tratamiento en escolares de 6 a 12 años de edad de San Luis Potosí. Rev de Invest Clín 2010; 62(3): 206-213. [ Links ]
28. Tapias Ledesma MA, Martín-Pero L, Hernández V, Jiménez R, Gil de Miguel A. Prevalencia de caries en una población escolar de doce años. Av Odontoestomatol 2009; 25(4): 185-191. [ Links ]
29. Barroso Barbosa J, Guinot Jimeno F, Bellet Dalmau LJ, Barbero Castelblanque V. La importancia de la dieta en la prevención de la caries. Gaceta dental: industria y profesiones 2007; 181: 116-135. [ Links ]
30. Pereira SM, Tagliaferro EP, Pardi V, Cenci MS, Cortellazzi KL, Ambrosano GM et al. Sugar consumption and dental health: Is there a correlation? Gen Dent 2010; 58(1): e6-e12. [ Links ]
31. Santa Gaviria AM. Memoria institucional programa UNI Rionegro (Colombia) 1991-2002. [Trabajo de grado: Bibliotecología]. Medellín: Universidad de Antioquia; 2003. [ Links ]
32. Kunkel SR, Atchley RC. Why gender matters: being female is not the same as not being male. Am J Prev Med 1996; 51: 294-296. [ Links ]
33. Arantes R, Santos RV, Frazao P, Coimbra CE Jr.Caries, gender and socio-economic change in the Xavante Indians from Central Brazil. Ann Hum Biol 2009; 36(2):162-175. [ Links ]
34. Mansbridge J. The influence of social and economic conditions on the prevalence of dental caries. Arch Oral Biol 1960; 1(3): 241-253. [ Links ]
35. Dummer PM, Addy M, Hicks R, Kingdon A, Shaw WC. The effect of social class on the prevalence of caries, plaque, gingivitis and pocketing in 11-12-year-old children in South Wales. J Dent 1987; 15(5): 185-190. [ Links ]
36. Zurriaga O, Martínez-Beneito MA, Abellán JJ, Carda C. Assessing the social class of children from parental information to study possible social inequalities in health outcomes. Ann Epidemiol 2004; 14(6): 378-384. [ Links ]
37. Pereira SM, Tagliaferro EP, Ambrosano GM, Cortelazzi KL, Meneghim Mde C, Pereira AC. Dental caries in 12-year-old schoolchildren and its relationship with socioeconomic and behavioural variables. Oral Health Prev Dent 2007; 5(4): 299-306. [ Links ]
