










Services on Demand
Journal
Article
 text in
text in  Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
Print version ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.24 no.1 Medellín July/Dec. 2012
ORIGINAL ARTICLES DERIVED FROM RESEARCH
Prevalence of malocclusions in a group of Mexican university students and its possible association with age, sex, and socioeconomic status, 2009
José Francisco Murrieta Pruneda1; Claudia Lorena Arrieta Ortega1; Lilia Adriana Juárez López2; Celia Linares Vieyra3; Martha Beatriz Gonz{alez Guevara4; Arcelia Meléndex Ocampo5
1 DMD, Full Professors, Zaragoza School of Higher Education,
Universidad Nacional Autónoma de México
2 Dental Surgery Intern, Zaragoza School of Higher Education,
Universidad Nacional Autónoma de México
3 MSc, Full Professor, Stomatology Undergraduate Program, Universidad
Autónoma Metropolitana Xochimilco
4 MSc in Public Health, Full Professor, Pathology and Oral Medicine
Graduate Program, Universidad Autónoma Metropolitana Xochimilco
5 MSc in Public Health, Full Professor, School of Dentistry, Universidad
Nacional Autónoma de México
SUBMITTED: AUGUST 12/2011-ACCEPTED: JULY 17/2012
Murrieta JF, Arrieta CL, Juárez LA, Linares C, González MB, Meléndez A. Prevalence of malocclusions in a group of Mexican university students and its possible association with age, sex, and socioeconomic status, 2009. Rev Fac Odontol Univ Antioq 2012; 24(1): 121-132.
ABSTRACT
INTRODUCTION: dental occlusion refers to the relationships of teeth at rest; it may be altered by a variety of factors. The purpose
of this study was to evaluate the prevalence of dental malocclusions and their possible relations to age, sex, and socioeconomic status
in a group of university students.
METHODS: : the epidemiological survey was conducted in two moments: application of a questionnaire,
and an oral examination. Two examiners were standardized for this purpose (Cr = 0.03, Ca = 0.89, k = 0.902).
RESULTS: 47.7% of the
students come from the middle class. 13.2% presented normal occlusion, and 86.8% had dental malocclusion. Their distribution per age,
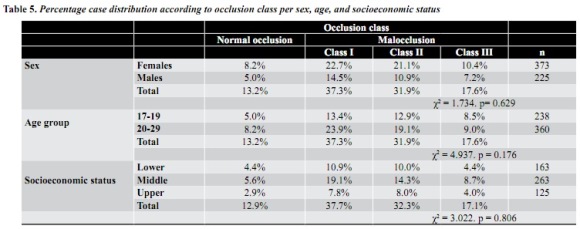
sex, and socioeconomic status did not show statistically significant differences. Concerning malocclusion classification, the most common
one was Class I (37.3%), a figure which happened to be lower than expected, in comparison to the same condition in similar populations.
CONCLUSIONS: the only conclusion drawn from this study is that socioeconomic status is not a factor associated to the frequency of dental
occlusion classification in this population, so there might be other factors to be evaluated, such as cultural and educational factors.
Key Words: dental occlusion, Angle classification, dental malocclusion, prevalence, socioeconomic status.
INTRODUCTION
Among the different factors that affect the oral cavity health, stability, and functioning is dental malocclusion, an alteration that occurs when dental arches do not comply with the correct and normal laws of lower-upper teeth relationships, in their transversal, anteroposterior, or vertical direction. In other words: it is the alteration of the relationships of teeth at rest. Due to its high prevalence among the population in general, it is considered to be the third cause of oral morbidity, and therefore is categorized as an oral public health issue; nevertheless, its importance rests not only on the number of people who suffer this alteration, but also on the harmful effects that it may produce in the oral cavity, as it alters functions such as mastication, deglutition, and speech, and its esthetical impact affects the patients' self-esteem and quality of life. 1-7
Prevalence of malocclusions worldwide is high, ranging from 65 to 89% of the affected population, as reported by Dacosta8 and Onyeaso9, 10 among Nigerians, Grando11 among Brazilians, and Oriel Orellana12 among Peruvians. Class I malocclusion is the most common one in these populations, in comparison to classes II and III (Angle classification), although in some cases this pattern varies, as reported by Segura, 13 Garibay14 and Galindo, 15 who observed a greater prevalence of class II malocclusion. Their behavior among Mexican population follow the same pattern; reports by Garibay, 14 Galindo15 and Aliaga, 16 to name just a few, suggest high prevalence rates in different population groups. Distributions by age and sex have demonstrated that dental malocclusions occur more frequently as age increases, basically due to the time of teeth exposure to several risk factors to develop this malformation. Similarly, the behavior by sex is very irregular, as pointed out by Grando, 11 Onyeaso, 9 Danaie,17 and Gelgör, 18 who have reported greater prevalence among males, in opposition to Montiel 19 and Robledo Yslas,20 who have found higher prevalence rates among females. Nevertheless, the studies by Gelgör, 18 Onyeaso, 21 Aliaga, 16 Robledo Yslas, 20 Talley, 22 and Silva23 all agree on stating that these differences are not significant, thus demonstrating that malocclusion prevalence is not connected to these two variables.
Concerning socioeconomic level, epidemiological evidence suggests that social determinants of the frequency and distribution of pathological events are hierarchically higher than biological determinants. This means that, in the generation of this condition, influence of socioeconomic status is more important than race, age, or sex. Currently, the field of epidemiology struggles to find scientific, objective, and operative statements to express the laws that govern this process both in an individual and collective basis. 24 Health is considered a social value related to the individuals' capacity to provide themselves the means to preserve it, taking into account the existence of substantial differences among diverse social groups due to socioeconomic status; consequently, it is possible to accept the existence of different epidemiological profiles in terms of the behavior of diseases. 24-26 The studies by Louis, 27 Heimer28 and Hebling29 express this association and prove that individuals with lower purchasing capacity do not present the same risks to develop malocclusion in comparison to the ones with greater economic capacity, and therefore the risks to get sick are different. Based on these conditions, an observational, descriptive, transversal, and prospective epidemiological study was conducted on 538 university students aged seventeen to twenty-nine years old, of both sexes, in order to assess dental malocclusions prevalence and their possible relation to sex and socioeconomic status.
MATERIAL AND METHODS
A descriptive, transversal, prospective study was conducted. The study population included students from Universidad del Valle de México at Tlalpan and from the UNAM's Zaragoza School of Higher Studies, whose ages ranged from seventeen to twenty-nine years old, of both sexes, living in the Distrito Federal and Estado de México, with no previous orthodontic treatment. They all accepted participating in this study by signing a consent form.
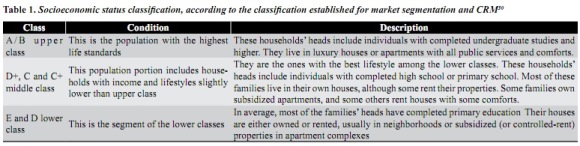
For the epidemiological survey, two interns of the Dental Surgery Program were standardized to perform as examiners. In order to make sure that concordance among the examiner's observations did not happen by chance, the Kappa and Cohen statistical value was calculated, yielding an almost perfect standardization (Cr = 0.03, Ca = 0.89, k = 0.902). The epidemiological information was obtained in two different moments: the first one implied applying a questionnaire to inquire about the interviewee's socioeconomic status, and the second one included oral examinations in order to diagnose each student's type of dental occlusion. For the first condition, socioeconomic status was set according to the classification established for market segmentation and CRM, 30 including aspects such as the family's head education level, family income, and type of house, public services, and social security (table 1). Oral examinations were performed on the students seated on a chair, by using mouth mirrors N.° 5 with no magnification and daylight. The obtained data were registered on an epidemiological sheet previously validated on a population with similar characteristics in order to guarantee that the instrument was really measuring the variable of interest in both its content and the applied criteria. Concurrent and predictive validity was evaluated by means of a correlation coefficient that would establish a possible diagnosis margin, whose value was 0.83. Similarly, careful attention was paid to asepsis, by using white robes, disposable gloves, and surgical masks; also, mouth mirrors were properly sterilized by dry heat.
To estimate dental occlusion class, students were asked to open their mouths in order to perform exploration from the right side to the left side. To evaluate type of dental malocclusion, the criteria established by Angle31 were used.
It was classified as normal occlusion when the mesiobuccal apex of the first permanent upper molar was occluding the mesiobuccal sulcus of its lower counterpart without altering the relationships between upper anterior teeth and lower teeth. Class I malocclusion was considered when the first upper permanent molar mesiobuccal apex was occluding the mesiobuccal of its permanent lower counterpart but the patient presented some kind of alteration in the relation of upper teeth and lower teeth at the anterior sextant. Class II malocclusion was considered when the first permanent lower molar mesiobuccal sulcus was not receiving the mesiobuccal apex of the first upper permanent molar but the contact point was located at its distobuccal apex or even more distal; and it was classified as class III malocclusion when the first permanent lower molar was occluding in a mesial direction the relation to the first upper permanent molar, it is, when the mesial apex of the upper one was occluding lower premolars. The statistical analysis was performed by means of the statistic package SPSS 15,0 Windows version. In order to evaluate malocclusion prevalence by age and sex, frequency measures were calculated. And to estimate possible malocclusion relations to age, sex, and socioeconomic status, the Pearson's and Mantel & Haenszel's X2 value was calculated when the cases were registered on tetrachoric contingency tables.
RESULTS
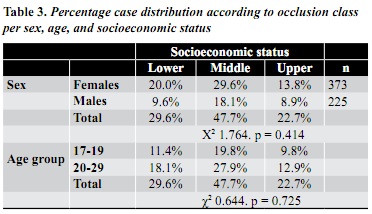
A total of 598 university students were examined. 39.8% of these students were seventeen to nineteen years old, while the remaining 60.2% were twenty to twenty-nine years old. Concerning sex, 62.9% were females and 37.6% were males (tabla 2).

Concerning students distribution by socioeco- nomic status and age group, the tendency was towards an intermediate category, that is, 47.7% of the students came from the middle class. In terms of sex distribution, in both categories the frequency per socioeconomic level was similar to the distribution observed per age (table 3).
Concerning case distribution according to dental occlusion class, 13.2% presented normal occlusion while 86,8% showed some kind of dental maloc- clusion.
The behavior by age, sex, and socioeconomic status showed some differences among the categories of each variable; however, they were not statistically significant (tabla 4).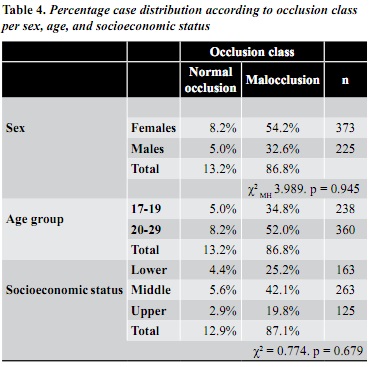
DISCUSSION
Malocclusions happen when maximum teeth in- tercuspation is altered so that teeth do not comply with the laws of normal and correct relationships between upper and lower teeth in transversal, antero-posterior, or vertical direction. 7 It is widely accepted that dental occlusion alterations are the third cause of oral morbidity worldwide. 3, 4-6 This situation was verified by the present study, in which dental malocclusions prevalence was very high—a similar behavior was observed in other Mexican population groups, in which a prevalence of at least 70% was observed among the studied population. 3-6
The results of this study in terms of malocclusion frequency following Angle's classification demons- trated that class I malocclusion was the one most frequently found, in comparison to normal occlu- sion, class II and class III malocclusions, agreeing with the reports by Onyeaso, 9, 10 Murrieta, 32 Cervan- tes, 33 and Pérez Meraz. 34 This finding is important because class I malocclusions include anomalies in the anterior sextant, where anteroposterior relation- ships of the dental arches, both upper and lower, are within normal ranges; however, there might be altered vertical or transversal relationships in the arches, where crowding and bad positions are clear evidences of class I malocclusion. 1, 3, 8
Now, class I malocclusion frequency happened to be lower than the one reported by Grando, 11 Onyeaso, 21 Dacosta, 8 Martínez, 1 Pérez Meraz, 34 and Cruz del Carmen, 35 similar to the reports by Gelgör 18 and Galindo, 15 and greater than the results by Garibay. 14 In relation to class II and class III malocclusion prevalence, they also happened to be similar to the reports by other authors. Similarly, class II malocclusion was always more frequent than class III; 4, 8-10, 12, 13, 18, 21, 22, 32, 36 however, in terms of the frequency of class II and class III malocclusions among the study population, the prevalence was higher than that reported by Hamamci 36 and Murrieta32 —differences that happened to be statistically significant (t = 4.824, p = 0.001 and t = 6.372, p = 0.000, respectively). One may actually think that these differences between class II and class III malocclusions were due to measurement issues; however, let`s bear in mind that only two examiners were in charge of the epidemiological survey, which makes bias less probable; on the other hand, the examiners were previously standardized (kappa = 0.902), and according to Cohen criteria, calibration was almost perfect (p = 0.000). Therefore, the only explanation to this behavior is that malocclusions frequency and distribution is highly variable due to its multifactorial condition, so that the factors that enable class II and class III malocclusions probably influence each person and population in different manners.
Concerning malocclusion distribution by sex, females presented a greater prevalence in our study, a behavior that agrees with the reports by Onyeaso, 21 Murrieta, 32 Martínez, 1 Montiel, 19 Silva, 23 and Robledo, 20 but contrary to the findings by Grando, 11 Galindo, 15 Danaie, 17 and Gelgör, 18 who observed higher malocclusion prevalence rates among males. Nevertheless, similarities and differences with previous studies and reports are not really relevant because the differences found among both sexes were not statistically significant. In fact, no theoretical model allows concluding that females in comparison to males, or vice versa, have different risk to develop any class of malocclusion. Therefore, this information is only useful to point out distribution of the disease.
In relation to a possible association between malocclusion prevalence and socioeconomic status, this was not statistically significant although a relation between both variables was expected. The only thing this result may suggest is that people's purchasing capacity is not the most relevant factor for the alteration of dental occlusion or for individuals requesting dental attention of a preventive nature to avoid suffering it, either by serial extractions, orthopedics, or by keeping dental arches gaps in the case of early primary teeth loss. Therefore, there is a new alternative to explain this condition by the influence of other factors of similar importance, such as factors of cultural and educational nature, as conditions that may move patients to seek dental attention, since the importance given to oral health is related to the referential framework that influences perceptions of the condition itself. This observation must be taken with careful consideration as it may explain how behavioral or influential co- dependencies may exist among the determining factors that influence health conditions, in particular oral health conditions. 27, 29, 37, 38
CONCLUSIONS
The conclusion to be drawn is that dental malocclusion prevalence in the study population was high and it was not associated to socioeconomic status. This condition may probably be associated to cultural and educational issues, as purchasing capacity does not influence the decision to seek preventive attention to avoid developing any type of malocclusion. Individuals may possess good purchasing capacity but if they do not value oral health they won't seek dental attention as oral health is not among their list of personal welfare priorities.
CORRESPONDING AUTHOR
José Francisco Murrieta Pruneda
Calzada de los Tenorios N.° 91 casa 24-D
Colonia Ex. Hacienda. Coapa. Tlalpan 14300
México, Distrito Federal. México
email address: francisco.murrieta@gmail.com
Phone number: 56 73 35 02, 56 23 07 01
REFERENCES
1. Martínez GR, Mendoza OL, Fernández LA, Pérez T. Características cefalométricas en la maloclusión clase II. Rev Odont Mex 2008; 12(1): 7-12. [ Links ]
2. Álvarez NC, Servín HS, Pares VF. Frecuencia de los componentes de la maloclusión clase II esquelética en dentición mixta. Revista ADM 2006; 63(6): 210-214. [ Links ]
3. Evensena JP, Øgaardb B. Are malocclusions more prevalent and severe now? A comparative study of medieval skulls from Norway. Am J Orthod Dentofacial Orthop 2007; 131(6): 710-716. [ Links ]
4. García HB. Facultad de Estudios Superiores Zaragoza. Prevalencia de maloclusiones en niños en edad escolar asociada al tiempo de dedicación de la madre al cuidado de sus hijos. [Tesis especialidad]. Zaragoza: FES-Zaragoza, UNAM; 2007. [ Links ]
5. Alonso AA, Albertini JS, Bechelli AH. Oclusión y diagnóstico en rehabilitación oral. 2.ª ed. México: Panamericana; 2007. [ Links ]
6. Santos JD. Oclusión: principios y conceptos. 2.ª ed. Caracas: Actualidades Médico Odontológicas Latinoamérica; 2000. [ Links ]
7. Guardo AJ. Ortodoncia. 4.ª ed. Buenos Aires: Mundi; 2004. [ Links ]
8. Dacosta OO. The prevalence of malocclusion among a population of northern Nigeria school children. West Afr J Med 1999; 18(2): 91-96. [ Links ]
9. Onyeaso CO. An epidemiological survey of occlusal anomalies among secondary school children in Ibadan, Nigeria. Odontostomatol Trop 2003; 26(102): 25-29. [ Links ]
10. Onyeaso CO. Prevalence of malocclusion among adolescents in Ibadan, Nigeria. Am J Orthod Dentofacial Orthop 2004; 126(5): 604-607. [ Links ]
11. Grando G, Vedovello FM, Vedovello SA, Ramírez YG. Prevalence of malocclusions in a young Brazilian population. Int J Orthod Milwaukee 2008; 19(2): 13-16. [ Links ]
12. Orellana O, Mendoza JZ, Perales ZS, Marengo H. Estudio descriptivo todas las investigaciones sobre prevalencia de maloclusiones realizadas en la Universidad de Lima, Ica y Arequipa. Odont Sanmarquina 2000; 5(1): 39-43. [ Links ]
13. Segura MN, Gutiérrez SM, Ochoa RM. Frecuencia de maloclusión en niños de 3 a 5 años de edad, policlínica Pedro Díaz Coello. Corr Med Cient Holg 2006; 10(1): 55-57. [ Links ]
14. Garibay CM. Prevalencia de maloclusiones y presencia de síntomas de disfunción temporomandibular en una muestra de pacientes. [Tesis de pregrado]. México: Facultad de Odontología, UNAM; 2006. [ Links ]
15. Galindo RM. Prevalencia de maloclusiones esqueletales y dentales en pacientes que acudieron a las Clínicas Multidisciplinarias Netzahualcóyotl, Zaragoza, Tamaulipas y Estado de México, durante el periodo de enero a septiembre del 2001. [Tesis de pregrado]. Zaragoza: FES-Zaragoza, UNAM; 2008. [ Links ]
16. Aliaga CA, Mattos VM, Aliaga CR, Castillo MC. Maloclusiones en niños y adolescentes de caseríos y comunidades nativas de la Amazonia de Ucayali, Perú. Rev Perú Med 2011; 28(1): 27-31. [ Links ]
17. Danaie SM, Asadi Z, Salehi P. Distribution of malocclusion types in 7-9 years old Iranian children. East Mediterr Health J 2006; 12(1-2): 236-240. [ Links ]
18. Gelgör IE, Karaman AI, Ercan E. Prevalence of malocclusion among adolescents in central Anatolia. Eur J Dent 2007; 1(3): 125-131. [ Links ]
19. Montiel JM. Frecuencia de maloclusiones y su asociación con hábitos perniciosos en una población de niños mexicanos de 6 a 12 años de edad. Revista ADM 2004; 61(6): 209-214. [ Links ]
20. Robledo R. Prevalencia de maloclusiones en pacientes de 6 a 14 años de las Clínicas Periféricas las Águilas y Aragón. [Tesis de pregrado]. México: Facultad de Odontología, UNAM; 2008. [ Links ]
21. Onyeaso CO, Sanu OO. Psychosocial implications of malocclusion among 12 to 18 years old secondary school children in Ibadan, Nigeria. Odontostomatol Trop 2005; 8(109): 39-48. [ Links ]
22. Talley MM, Katagiri KM, Pérez TH. Casuística de maloclusiones clase I, clase II y clase III según Angle en el Departamento de Ortodoncia de la UNAM. Rev Odont Mex 2007; 11(4): 175-180. [ Links ]
23. Silva RG, Kang DS. Prevalence of malocclusion among Latino adolescents. Am J Orthod Dentofacial Orthop 2001; 119(3): 313-315. [ Links ]
24. Arredondo AM. Análisis y reflexión sobre modelos teóricos del proceso salud-enfermedad. Cad Saúde Publica 1992; 8(3): 254-261. [ Links ]
25. Ramos RA, Martínez RA, Morales FA, Valdez LR. La prematurez y sus repercusiones en el crecimiento y desarrollo del niño, en la zona metropolitana de Guadalajara, Jalisco, México. Cad Saúde Publica 1998; 14(2): 102-111. [ Links ]
26. Nieto MV, Nieto MA, Lacalle RJ, Abdel KM. Salud oral de los escolares de Ceuta. Influencias de la edad, el sexo, la etnia y el nivel socioeconómico. Rev Esp Salud Pública 2001; 75(6): 541-550. [ Links ]
27. Louis J.P. Calisti M, Michael C, Martha HF. Correlation between malocclusion, oral habits, and socioeconomic level of preschool children. J Dent Res 1960; 39(3): 450-457. [ Links ]
28. Heimer MV, Tornisiello KC, Rosenblatt A. Non-nutritive sucking habits, dental malocclusions, and facial morphology in Brazilian children: a longitudinal study. Eur J Orthod 2004; 30(6): 580-585. [ Links ]
29. Hebling SR, Cortelazzi KL, Tagliaferro EP, Hebbling E, Ambrosano GM, Meneghim MC et. al. Relationship between malocclusion and behavioral, demographic and socioeconomic variables: a cross-sectional study of 5 years. J Clin Pediatric Dent 2008; 33(1): 75-79. [ Links ]
30. Magallán D. Segmentación de mercados y CRM para sitios noticiosos en línea. El Universal. 2008 ene 04; Sec segunda: 2 (col 3). [ Links ]
31. Santi MJ. Maloclusión clase I: definición, clasificación, características clínicas y tratamiento. Revista Lat Ort Odont 2003; 18(3): 217-221. [ Links ]
32. Murrieta PF, Cruz DP, López AJ, Marques DM, Zurita MV. Prevalencia de maloclusiones dentales en un grupo de adolescentes mexicanos y su relación con la edad y el sexo. Acta Odont Ven 2007; 65(1): 85-92. [ Links ]
33. Cervantes AP. Relación entre postura y maloclusión en pacientes infantiles de la Clínica Periférica Padierna, turno vespertino, 2008. [Tesis de pregrado]. México: Facultad de Odontología, UNAM; 2009. [ Links ]
34. Pérez C. Prevalencia de maloclusiones y hábitos perniciosos en una población de escolares de 5to. y 6to. grado en la escuela primaria Estado de Michoacán. [Tesis de pregrado]. México: FES-Zaragoza: UNAM; 2008. [ Links ]
35. Cruz W. Prevalencia de maloclusiones dentales en pacientes que solicitaron atención odontológica en la Clínica Periférica Azcapotzalco UNAM ciclo 2007-2008 [Tesis de pregrado]. México: Facultad de Odontología, UNAM; 2009. [ Links ]
36. Hamamci N, Basaran G, Uysal E. Dental Aesthetic Index scores and perception of personal dental appearance among Turkish university students. Eur J Orthod 2009; 31(2): 168-173. [ Links ]
37. Senado DJ. Los factores de riesgo en el proceso salud-enfermedad. Rev Cubana Med Gen Integr 1999; 15(4): 453-460. [ Links ]
38. Moreno AA. Reflexiones sobre el trayecto salud-padecimiento-enfermedad-atención: una mirada socioantropológica. Salud Pública Méx 2007; 49(1): 63-70. [ Links ]
