










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
versão impressa ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.25 no.1 Medellín jul./dez. 2013
ORIGINAL ARTICLES DERIVED FROM RESEARCH
REPRODUCIBILITY OF SOFT TISSUE CEPHALOMETRIC LANDMARK IDENTIFICATION BY CONVENTIONAL AND DIGITAL DIRECT RADIOGRAPHY
Margarita María Bonilla Londoño1; Judith Patricia Barrera Chaparro2; Angela Ptricia Arroyave Godoy3; Mónica Eliana Díaz Roa4
1 Dentist, Orthodontics Specialist. Fundación Universitaria San Martín. Bogotá, Colombia
2 Dentist, Epidemiology Specialist. Research Professor. Dentistry Graduate School. Fundación Universitaria San Martín. Bogotá, Colombia. E-mail address: barrerajudith@gmail.com
3 Dentist, Orthodontics Specialist. Fundación Universitaria San Martín. Bogotá, Colombia
4 Dentist, Orthodontics Specialist. Fundación Universitaria San Martín. Bogotá, Colombia
SUMBITTED: MAY 8/2012-ACCEPTED: JULY 30/2013
Bonilla MM, Barrera JP, Arroyave ÁP, Díaz ME. Reproducibility of soft tissue cephalometric landmark identification by conventional and digital direct radiography. Rev Fac Odontol Univ Antioq 2013; 25(1): 76-91.
ABSTRACT
INTRODUCTION: there is little information on the reproducibility of soft tissue cephalometric points; the purpose of this study was then to evaluate the reproducibility and accuracy of soft tissue cephalometric landmark identification in direct digital radiography and conventional radiography. METHODS: 11 pairs of conventional and direct digital radiographs were introduced in the Cephapoint program. 10 cephalometric points were located on a Cartesian plane (X and Y) in conventional and digital images. The measurements were taken twice by 3 operators with 1 week interval. Interobserver average error was calculated in order to assess reproducibility in each point, and intraobserver error was used to determine accuracy. RESULTS: interobserver error in soft tissue cephalometric points was less than 1 mm for most points in both images, except in chin and pogonion, with no statistically significant differences. Statistically significant differences were found between the variances in the X axis, with less variability in the case of digital radiography in these points: labrale superius (p = 0.043), subnasale (p = 0, 013), columella (p = 0.038), stomion superius (p = 0.029), and stomion inferius (p = 0.015). The Y axis did not show statistically significant differences between the two methods. The assessment of intraobserver reproducibility showed an excellent Intraclass Correlation Coefficient (ICC) (0.935) in both methods.. CONCLUSION: According to the findings of this study, the evaluated radiographs and methods offer similar diagnostic accuracy.
Key words cephalometry, results reproducibility, radiography, double-photon emission radiographic image.
INTRODUCTION
In orthodontics, treatment success and patient satisfaction depend to a large extent on aspects such as diagnosis, the various treatment options available, and the operator's skills. Timely appropriate diagnosis is essential to establishing treatment goals, using various means and tools such as cephalometric tracing, which has been used since 1930 to assess anthropometric data.1 This technique involves taking measurements on a radiograph of the patient's skull, where points are located, planes are traced, and angles are measured, and the results are compared with measurements previously established by several studies;2-6 these studies have achieved the standardization of methods of analysis so that cephalometric tracing is now considered as a reliable diagnosis technique.7
Conventional radiography equipment are being gradually replaced by digital technology, which offers advantages such as instant image achievement, easy storage, elimination of the development phase, and the possibility of digitally sharing images.8
To assess reproducibility (interobserver error) of cephalometric landmark identification by means of conventional and digital radiography, several studies have been conducted in order to compare these two types of radiographs.8-11 These studies show that reproducibility of landmark identification in digital images is comparable to that of conventional radiographs.
Recently, Bonilla et al12 conducted a study to determine the reproducibility of 14 hard tissue cephalometric points; for this study they created and used Cephapoint, a program that allows landmark identification on a computer screen directly with the cursor. They used a sample of 22 films, 11 digital and 11 conventional radiographs, each pair taken on the same patient and with the same equipment; they took the digital radiograph first and then the conventional one. They found out that all points show similar reproducibility in both types of radiographs, except for these points: infraorbital, posterior nasal spine, joint, porion, and basion, with direct digital image presenting the lowest interobserver error. In another study, Sandler reported that joint and gonion are the points with the most reproducibility by manual tracing.13
Few studies determine reliability in identifying soft tissue landmarks.14-17 Wisth and Böe15 claim that soft tissue measurements depend on the quality of conventional cephalometry more than hard tissue measurements. Also, Hagemann et al16 report that reproducibility of pronasal and pogonion in soft tissues is better in digital imaging than in conventional radiography. On the other hand, Dvortsin,17 by comparing manual tracing in a 1:1 printing with Viewbox® version 3.1.1.9 in soft tissues, noted that the area around the stomion was the least reproducible, and although small statistically significant differences were found, the clinical relevance of these findings is questionable.
Given the limited information found in the literature, the goal of this study was to evaluate the reproducibility of soft tissue cephalometric landmark identification using direct digital radiography and conventional radiography.
Conflict of Interest Statement
The authors declare that this research study does not have any conflict of interest. The study was approved by the Bioethics Committee of Fundación Universitaria San Martín School of Dentistry.
METHODS
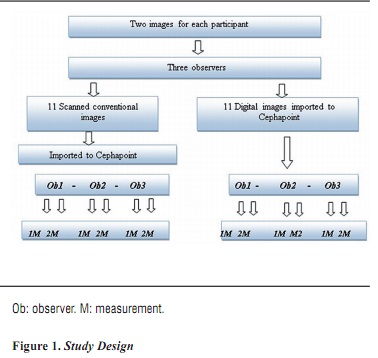
This was a concordance study on 11 direct digital lateral radiographs used in a previous study by Bonilla et al;12 the radiographs were taken by orthodontic students once informed consent was obtained. The use of these materials for research purposes was approved by the Bioethics Committee of Fundación Universitaria San Martín (FUSM) Department of Dental Graduate Studies.
The radiographs were taken in natural head position by a trained operator. Each participant was taken two radiographs, one using a conventional development process, taken with a Veraview Epocs J Morita® machine— these were scanned and transformed into analog digital images using an HP Deskjet F 4180® scanner with 600 dpi resolution—. The other was a phosphor-stimulated direct digital radiographic image, processed in an FCR CAPSULE X® machine, which immediately transfers images to the computer screen. The two radiographic images of each participant were imported to Cephapoint, a program designed to locate cephalometric points.12
Soft tissue points were selected bearing in mind that they are directly located, i.e., they are constructed points, so it was not necessary to draw anatomical structures, which are usually operator-dependent, thus allowing bias control during the study; these points were: labrale superius (Ls), labrale inferius (Li), subnasale (Sn), glabella (G'), columella (Cm), menton (Me), pogonion (Pg'), stomion superius (Stms), stomion inferius (Stmi), and lower vermilion (Vmi).
These cephalometric points were directly located on images displayed on a 14-inch Toshiba® monitor with a mouse-controlled cursor connected to Cephapoint, a program designed for a previous study.12 After recording each cephalometric point with the mouse, the monitor image indicated their position. The latter could be corrected until the operator was satisfied. The points were recorded on a form with X and Y coordinates. The computer program X axis was the upper margin of the image and the Y axis was its anterior margin.
In this study, the average position of three observers for each soft tissue cephalometric point was defined as the "reference parameter". This parameter was used to determine interobserver errors in both conventional and digital images. The average distance in millimeters between the reference parameter and the localizations identified by the observers was defined as interobserver error, and this in turn was used as a variable to determine each point's reproducibility. Consequently, reproducibility of landmark identification for each of the two images (conventional and digital) could be considered as the differences in these distances' magnitude from the average, between these two types of imaging.
Intraobserver accuracy or error is defined as the level of measurement agreement of each of the three observers, showing how close the cephalometric points are during the first and second observations at weekly intervals. It is obtained by comparing each operator's measurements, and is calculated with the Intraclass Correlation Coefficient (ICC) statistical method. Figure 1 shows the study design.
STATISTICAL ANALYSIS
The data were registered in Microsoft Excel 2007 and analyzed in the Statistical Package for Social Sciences (SPSS) version 15.0. Quantitative variables were analyzed using means and standard deviations. For comparing the conventional and digital methods, we used the Student t-test for independent groups and the Levene test for equality of variances. A significance level of Α = 0,05 was used for all the tests, and the confidence intervals were used with 95% reliability.
RESULTS
Reproducibility
In conventional images, the points with the highest interobserver error average in the X axis were menton (0.816 mm) and pogonion (0.699 mm). Regarding the Y axis, the highest averages were observed in labrale superius (0,687 mm) and menton (0.672 mm). In direct digital imaging, the points with the greatest interobserver error in the X axis were pogonion (0.792 mm) and menton (0.78 mm). In the Y -axis, the highest average occurred in menton (0.724 mm) followed by pogonion (0.604 mm) and labrale superius (0.594 mm). Interobserver error was no more than 1 mm in both types of X-rays. When comparing the average interobserver error between conventional and direct digital images, no statistically significant differences were found (p ≥ 0,05).
In most points, the level of interobserver error dispersion was lower in digital radiography as indicated by the standard deviation data, except in the X axis of glabella and the Y axis of labrale superius, subnasale, columella, stomion superius, and stomion inferius (table 1).
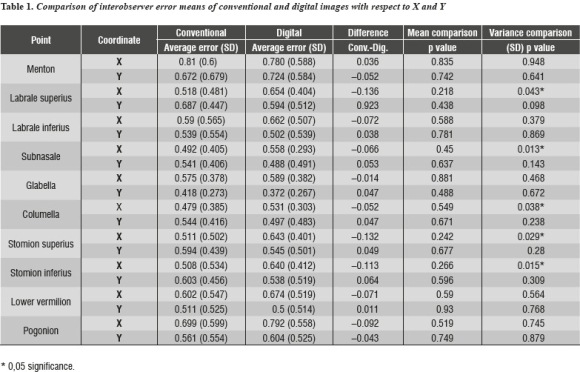
We compared standard deviation values between the conventional and digital methods, regardless of the average value of each point (Fisher's F test), which is considered to be a more reliable interobserver error indicator, as the standard deviation measures dispersion error levels. A statistically significant difference was found within the standard deviation (SD) of the X axis in labrale superius (p = 0.043), subnasale (p = 0.013), columella (p = 0.038), stomion superius (p = 0.029) and stomion inferius (p = 0.015). These differences favor digital radiography due to their lower standard deviation values. On the Y axis no statistically significant differences were observed between the two methods (table 1).
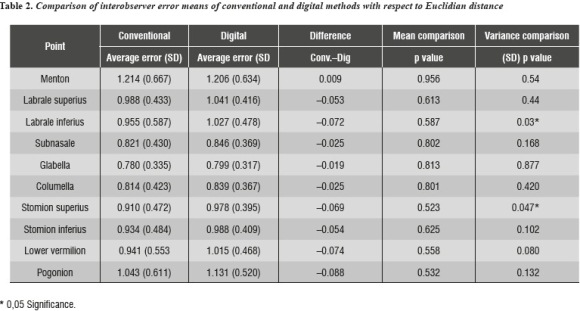
In order to estimate each point's reproducibility by integrating the values obtained in the X and Y axes, the Euclidean distance was calculated. Interobserver error averages greater than 1 mm were observed for conventional radiography in chin (1,214 mm) and pogonion (1,043 mm), and for digital radiography the averages greater than 1 mm were chin (1,206 mm), pogonion (1,131 mm), labrale superius (1,041 mm), labrale inferius (1,027 mm), and lower vermillion (1,015 mm), with no statistically significant differences between the methods.
The greatest standard deviations in the conventional method were found in chin (0, 667 mm) and pogonion (0, 611 mm) and in the digital method in chin (0.634 mm). By comparing standard deviations, statistically significant differences (p < 0.01) were found in the dispersion between the conventional and direct digital images, with higher levels of significance in labrale inferius (p = 0.003) and stomion superius (p = 0.047); higher dispersion values are observed in conventional radiography, indicating less reproducibility because its standard deviation is higher (table 2).
Precision
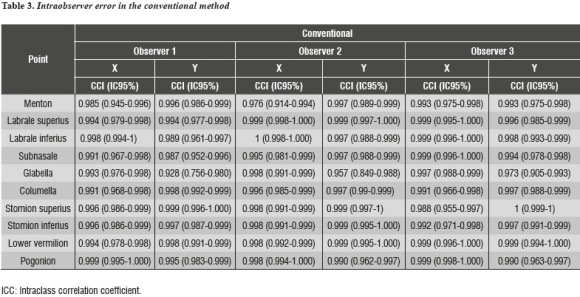
The assessment of intraobserver reproducibility yielded excellent Intraclass Correlation Coefficient (ICC) in both methods, being greater than 0.928 for the conventional method (table 3).
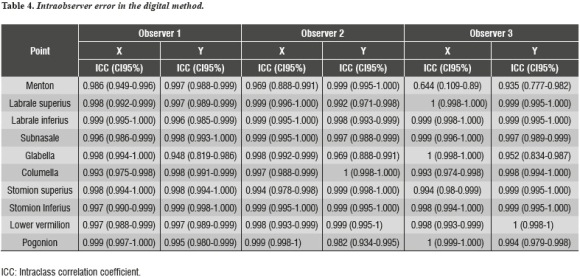
In the digital method, ICC was above 0.935 with the exception of the chin, which was 0,644 under observer 3 (table 4)
DISCUSSION
Some studies that compare conventional radiographs with digital radiographs simultaneously recorded have demonstrated that measurements of digital images are more reproducible due to better sight of soft tissues.18-19
Other authors point out that, although digital images can be improved, this only increases reproducibility— instead of accuracy.19-20 However, the loss of detail that occurs when an image is compressed to JPEG format does not significantly affect diagnostic quality.10
In the present study we found that interobserver error averages for conventional and digital methods in X and Y axis did not show significant differences in the Euclidian distance between the methods, but there were higher error values for menton and pogonion, with averages greater than 1 mm on the Euclidean distance; these points were difficult to locate in conventional radiography due to the dominance of a radiolucent area which makes soft tissue less visible in these areas. In contrast, Hagemann et al compared digital radiography with conventional radiography and found out that pronasale and pogonion of soft tissue were the most reproducible points in digital imaging.16
Another finding of the present study indicates that in digital radiography labrale superius, labrale inferius, and lower vermilion presented interobserver error values greater than 1 mm, but with no significant differences compared to conventional imaging, suggesting that the lower vermilion was more difficult to locate because two-dimensional radiographic imaging does not clearly show where the lower lip ends. Other authors compared digital and manual tracing and found out statistically significant differences between the digital and manual methods in labrale inferius;20 also, Cooke and Wei found out that lips prominences were sites of poor identification when using manual tracing..21
As for dispersion, recorded according to standard deviation data—which was considered in this study as a more reliable measure of reproducibility— statistically significant differences were found in the labrale superius, subnasale, columella, stomion superius, and stomion inferius on the X axis, and greater reproducibility was found in digital radiography. In terms of Euclidean distance, labrale inferius and stomion superius were more reproducible in digital imaging, which was more precise and accurate. The lower interobserver dispersion error in digital imaging may be explained because these radiographs show greater sharpness and contrast in gray scale.
In the present study, stomion superius showed higher dispersion in conventional imaging because its location is found in the most curved area of the lips making it more difficult to locate in its lower part. Other authors found out that the stomion was less reproducible, because some individuals have lips in contact with each other, while others are slightly separated at rest, which makes it harder to locate this point, especially in patients with separated lips.17, 20
Glabella was the most reproducible point both in digital and conventional radiography with respect to the Euclidean distance; similar findings were reported by Lim et al, who compared reliability between computed lateral cephalometry and location of manual points in conventional radiography.22
In the present study, ICC was used to assess intraobserver reproducibility in each of the three observers; we obtained a value above 0.90 which was a great result, similar to that reported in other studies.11, 23-25 These results indicate a high level of measuring accuracy thanks to proper training of the observers; therefore, the found differences are attributed to the evaluated methods only.
The development of cephalometric tracing software has provided orthodontists with new possibilities because they allow manipulating image quality for greater clarity especially in soft tissues, but few studies have compared the location of cephalometric points and measurements soft tissue in digital and conventional images—which limits the comparisons of the present study. 18, 26-27
Kawahara et al reported no statistically significant difference between conventional and digital radiography, and they conclude that regardless of the method used or the clinician performing tracings manually or with software, it must be trained and calibrated for implementation;28
For this reason, this study included intraobserver evaluation, with satisfactory results.According to the results of this study, the differences between these methods are not clinically relevant as the application of either does not affect the diagnostic. Regardless of the method used, the individual must be trained and calibrated for implementing. Therefore, the choice of method of analysis depends on the orthodontist's judgment as to the assessment of advantages, disadvantages, costs, time, accessibility, and comfort.
CONCLUSIONS
Reproducibility, measured as interobserver error, was less than 1 mm for most points in conventional and digital imaging except for menton and pogonion, with no statistically significant differences.
Labrale inferius and stomion superius were more accurate in digital imaging with respect to conventional radiography, with statistically significant differences.
According to the findings of this study, the two methods show the same diagnostic validity.
REFERENCES
1. De Araujo P, Nascimento J, Mesquita F, Nery E. A comparative study of manual vs. computerized cephalometric analysis. Dental Press J Orthod 2010; 15(2): 44-51. [ Links ]
2. Steiner C. Cephalometrics for you and me. Am J Orthod 1953; 39(10): 729-755. [ Links ]
3. Legan HL, Burstone CJ. Soft tissue cephalometric analysis for orthognathic surgery. J Oral Surg 1980; 38(10): 744-751. [ Links ]
4. Burstone CJ, James RB, Legan H, Murphy GA, Norton LA. Cephalometrics for orthognathic surgery. J Oral Surg 1978; 36(4): 269-277. [ Links ]
5. McNamara JA Jr. A method of cephalometric evaluation. Am J Orthod 1984; 86(6): 449-469. [ Links ]
6. Sassouni V. A classification of skeletal facial types. Am J Orthod 1969; 55(2): 109-123.Vion P. Anatomía cefalométrica. São Paulo, Brasil: Ed. Santos. 1994: 45-60. [ Links ]
7. Chung RR, Lagravere MO, Flores-Mir C, Heo G, Carey JP, Major PW. A comparative analysis of angular cephalometric values between CBCT generated lateral cephalograms versus digitized conventional lateral cephalograms. Int Orthod 2009; 7(4): 308-321. [ Links ]
8. Bruntz LQ, Palomo JM, Baden S, Hans MG. A comparison of scanned lateral cephalograms with corresponding original radiographs. Am J Orthod Dentofacial Orthop 2006; 130(3): 340-348. [ Links ]
9. Uysal T, Baysal A, Yagci A. Evaluation of speed, repeatability, and reproducibility of digital radiography with manual versus computer-assisted cephalometric analyses. Eur J Orthod. 2009; 31(5):523-528. [ Links ]
10. Sayinsu K, Isik F, Trakyali G, Arun T. An evaluation of the errors in cephalometric measurements on scanned cephalometric images and conventional tracings. Eur J Orthod 2007; 29(1): 105-108. [ Links ]
11. Yu SH, Nahm DS, Baek SH. Reliability of landmark identification on monitor-displayed lateral cephalometric images. Am J Orthod Dentofacial Orthop 2008; 133(6): 790. [ Links ]
12. Bonilla M, Barrera J, Gutiérrez D, Paredes M, Puentes J. Comparación del error en la ubicación de puntos cefalométricos entre una imagen digital directa y una convencional. Revista Científica Sociedad Colombiana de Ortodoncia 2011; 18(17): 63-71. [ Links ]
13. Sandler PJ. Reproducibility of cephalometric measurements. Br J Orthod 1988; 15(2): 105-110. [ Links ]
14. Swennen GR, Grimaldi H, Berten JL, Kramer FJ, Dempf R, Schwestka-Polly R et al. Reliability and validity of a modified lateral cephalometric analysis for evaluation of craniofacial morphology and growth in patients with clefts. J Craniofac Surg 2004; 15(3): 399-412. [ Links ]
15. Wisth PJ, Böe OE. The reliability of cephalometric soft tissue measurements. Arch Oral Biol 1975; 20(9): 595- 599. [ Links ]
16. Hagemann K, Vollmer D, Niegel T, Ehmer U, Reuter I. Prospective study on the reproducibility of cephalometric landmarks on conventional and digital lateral headfilms. J Orofac Orthop 2000; 61(2): 91-99. [ Links ]
17. Dvortsin DP, Sandham A, Pruim GJ, Dijkstra PU. A comparison of the reproducibility of manual tracing and on-screen digitization for cephalometric profile variables. Eur J Orthod 2008; 30(6): 586-591. [ Links ]
18. Eppley BL, Sadove AM. Computerized digital enhancement in craniofacial cephalometric radiography. J Oral Maxillofac Surg 1991; 49(10): 1038-1043. [ Links ]
19. Macrí V, Wenzel A. Reliability of landmark recording on film and digital lateral cephalograms. Eur J Orthod 1993; 15(2): 137-48. [ Links ]
20. Naoumova J, Lindman R. A comparison of manual traced images and corresponding scanned radiographs digitally traced. Eur J Orthod 2009; 31: 247-253. [ Links ]
21. Cooke M, Wei H. Cephalometric errors: a comparison between repeat measurements and retaken radiographs. Aust Dent J 1991; 36: 38-43. [ Links ]
22. Lim KF, Foong KW. Phosphor-stimulated Computed Cephalometry: Reliability of Landmark Identification. Br J Orthod 1997; 24: 301-308. [ Links ]
23. Polat-Ozsoy O, Gokcelik A, Toygar Memikoglu TU. Differences in cephalomatric measurements: a comparison of digital versus hand-tracing methods. Eur J Orthod 2009; 31: 254-259. [ Links ]
24. Ongkosuwito E, Katsaros C, Hof M, Bodegon J, Kuijpers- Jagtman A. The reproducibility of cephalometric measurements; a comparison of analogue and digital methods. Eur J Orthod 2004; 24: 655-665. [ Links ]
25. Tsorovas G, Karsten AL. A comparison of hand-tracing and cephalometric analysis computer programs with and without advanced features-accuracy and tune demands. Eur J Orthod 2010; 10:1-8. [ Links ]
26. Chen YJ, Chen SK, Yao JC, Chang HF. The effects of differences in landmark identification on the cephalometric measurements in traditional versus digitized cephalometry. Angle Orthod 2004; 74(2): 155-161. [ Links ]
