










Services on Demand
Journal
Article
 text in
text in  Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
Print version ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.25 no.2 Medellín Jan./June 2014
ORIGINAL ARTICLES DERIVED FROM RESEARCH
TOMOGRAPHIC DETERMINATION OF RESIDUAL RIDGES SHAPE AND SIZE PREVALENCE IN EDENTATE PATIENTS
Amparo Constanza Varón de Gaitán1; Juan Carlos Bustamante Mesa2; Ana Catalina Hoyos Galvis3; Andrés Felipe Zapata Suárez4; Sonia Patricia Plaza Ruíz5
1 Dentist, Orthodontics Specialist. Academic Vice-President, UniCIEO, Bogotá D.C, Colombia. Email: sacademica@cieo.edu.co
2 Dentist, Candidate to Specialization in Implantology. UniCIEO, Bogotá D.C., Colombia. E-mail: juacarbus@hotmail.com
3 Dentist, Candidate to Specialization in Implantology. UniCIEO, Bogotá D.C., Colombia. E-mail: pacificb@hotmail.com
4 Dentist, Candidate to Specialization in Implantology. UniCIEO, Bogotá D.C., Colombia. E-mail: felione26@hotmail.com
5 Dentist, Orthodontics Specialist. Epidemiology Master's Degree candidate. Universidad El Bosque, Bogotá D.C, Colombia. E-mail: orthoplaza@hotmail.com
SUBMITTED: MAY 28/2013-ACCEPTED: SEPTEMBER 10/2013
Varón AC, Bustamante JC, Hoyos AC, Zapata AF, Plaza SP. Tomographic determination of residual ridges shape and size prevalence in edentate patients. Rev Fac Odontol Univ Antioq 2014; 25 (2):.
ABSTRACT
INTRODUCTION: the objective of this tomographic study was to determine residual ridges shape and size prevalence in edentate patients and its association with age, sex, and upper and lower residual ridge. METHODS: we evaluated 722 scans taken at the UniCIEO diagnostic center between 2010 and 2012, obtaining 102 residual ridges images, 70 of the maxilla and 32 of the mandible, from 73 patients (46 women and 27 men) aged between 24.67 and 90.17 years. The evaluation of residual ridge size and shape was achieved through nine templates generated by the Galaxis 3D computer program, of the Cone beam GALILEOS system (Sirona Dental Systems Inc., Bensheim, Germany). RESULTS: the prevalent shape and size of upper residual ridge were: large ovoid 48.6%, large triangular 42.9%, medium triangular 4.3%, large square 2.9%, medium ovoid 1.4%; and in the mandible they were: large ovoid 93.8%, and large square 6.25%. CONCLUSIONS: the most prevalent residual ridge size and shape was large ovoid both in the upper and lower maxilla. We found no association between shape/size and any of the variables under study.
Key words: prevalence, edentate arch, dental arch, alveolar processes, CT cone-beam.
INTRODUCCTION
Losing natural teeth produces several changes in the stomatognathic system and the craniofacial structures, which must be taken into account when determining the changes occurring in the edentate patient's maxilla and to achieve proper diagnosis, prognosis, and prosthetic treatment plan. According to the 1998 Oral Health National Study ENSAB III,1 the prevalence of edentulism in Colombia is 25% in both maxillae and 7% in the mandible only. In Mexico, in 2006,2 it affected 30% of individuals over 65 years; in the United States, in 2000,3 it affected 30% of the same population, and 33.33% in Spain in 2013.4
Geometrically, an arch is defined as a segment of a curve. Several authors, like Brader, have defined the arch as a section of a conical curve, a catenary curve, a parabola, an ellipse, a segment of the circumference, or a simple sphere.5-15 Some studies have even classified arch shapes. In 1934, Chuck evaluated the various human arch shapes and described them as square, narrow, and ovoid.16-18
Once the alveolar process disappears after teeth extraction, the patient keeps part of the tooth—the so-called residual ridge—. Residual ridges can be ovoid, square, or triangular.19, 20 In 2009, Misch highlighted the importance of the shape of both the edentate arch and the arch to be restored in diagnosing and planning implants.21 In 2010, Sagat et al conducted a finite elements study to assess the influence of arch shape, implant position, and stress distribution around it, concluding that these factors are more important than the length of the free end22
The shape and size of residual ridges can be influenced by numerous factors, including the soft tissues covering the residual ridge, sex, age, and race, to name just a few.23-27
The diagnostic methods to study and define the shape and size of residual ridge include plaster models, clinical calibration, mapping, and, recently, specialized Cone Beam tomographic analysis (CBCT) for use in dentistry. This led to the development of interactive computerized tomography (ICT) as a bridge between radiologists and clinicians, who usually need a diagnostic template to take advantage of this technique. Diagnostic templates allow dentists to incorporate a three-dimensional treatment plan (from the final prosthetic result) into the image examination phase and to evaluate the patient's anatomy in a three-dimensional treatment plan that can be viewed prior to surgery by members of the team involved in the implant.21
There are numerous studies on the prevalence of dentate arches in different populations and malocclusion types,18, 28-32 but the studies on residual ridge shape are scarce.33, 34 Table 1 shows a comparative analysis of some of these studies.
There are no available studies on the shape and size prevalence of residual ridges in Colombia. The objective of this tomographic study was to determine the prevalent shape and size of residual ridges in edentate patients who consulted the UniCIEO Diagnostic Center between 2010 and 2012.
METHODS
This was an observational cross-sectional study.35 The project was evaluated and approved by the UniCIEO Ethics Committee on February 14, 2012. The sample included 722 CT scans of patients who consulted the UniCIEO Diagnostic Imaging Center between 2010 and 2012. We selected 76 patients who met the inclusion criterion: having at least one totally edentate arch. Three patients were excluded because they presented distorted images—this being the only exclusion criterion—. From the remaining 73 patients, we obtained 70 images of upper residual ridges and 32 images of lower residual ridges, for a total of 102 tomographic images, which were labeled with a consecutive number for identification purposes and to preserve patients' confidentiality. Out of the 73 patients, only 29 were edentate in both maxillae.
Three operators with previous theoretical and practical training were selected to conduct the analysis and to determine the shape and size of each residual ridge.
Tomographic imaging
Images were obtained with a Galileos CT cone beam scanner (Sirona Dental Systems Inc., Bensheim, Germany). This system has a 15 x 15 x 15 cm3 x-ray volume, voxels of 0,3/0,15 mm resolution, time of exposure of 14/2-6 s, duration of reconstruction of 4 to 5 min, 85 kV, 5-7 ma, and an effective dose: 29 Μ Sv (21 more, 85 kV). It also uses a software for dental clinical consultation (Galaxis 3D), which provides three-dimensional volume reconstructions of the maxillofacial region, useful for both diagnosis and planning, with an accuracy of ± 0,15 mm. The manufacturer's instructions for imaging were carefully followed, making sure that the patient's occlusal plane remained parallel to the floor.
Orientation of tomographic images
After considering the three available methods to determine the shape and size of each patient's residual ridges: lateral, antero-posterior, and panoramic cephalometric imaging, we chose lateral cephalometric radiography because it allows better image orientation. Images were oriented in such a way that the vertical grid would go through the middle odontoid process and the nasopalatine foramen in the upper residual ridge; and in the lower residual ridge it would go horizontally through the menton orifice and vertically through the middle of the vertebra.
Defining the cutting site
In the panoramic image, the anatomical structures of reference were located in an axial view of the upper residual ridge, as shown in figure 1.
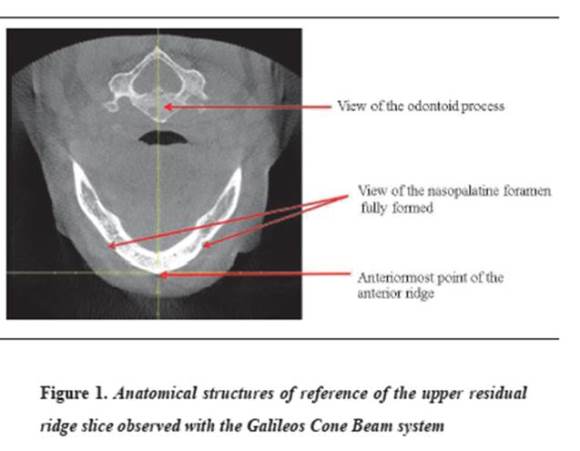
The vertical guide was positioned in such a way that it went through the middle of the odontoid process and the horizontal guide through the posterior wall of the nasopalatine foramen; this site was intersected at the transverse section where the horizontal guide was positioned. We decided that the cutting site would be located at the level of the anterior cortical of the lowest posterior wall of the nasopalatine foramen. The distance from the anterior nasal spine to the guide plane was measured by each operator with the ruler included in the software and then these measures were compared until obtaining a concordance no greater than or equal to 1.4 mm in height among the three operators, in order to have the same image for the analysis. This range was determined by calculating the method's error.
For the lower residual ridge, the chosen anatomical structures of reference were placed at the axial view of the lateral cephalometric radiography (figure 2).
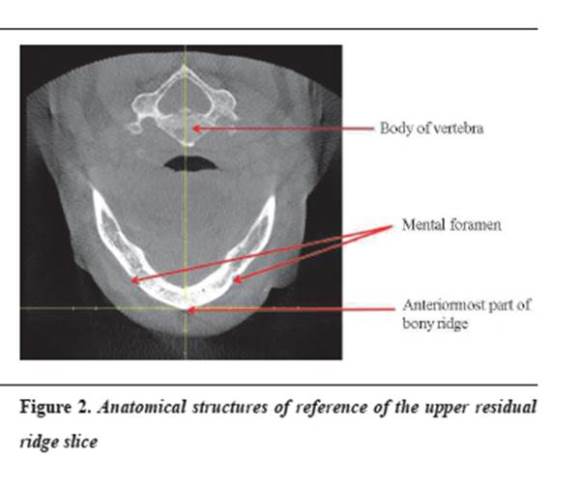
The vertical guide was positioned in such a way that in went through the center of the vertebra, and the horizontal through the anterior-most point of the lower bone ridge.
Defining shape and size
The obtained panoramic image showed the nine shape and size combinations offered by Galaxis 3D: small ovoid (UP), small square (ЏP), small triangular (VP), medium ovoid (UM), medium square (ЏM), medium triangular (VM), large ovoid (UG), large square (ЏG), and large triangular (VG). The cutting site was then located by checking the specific anatomical structures of reference for both upper arch (figure 3)and lower arch (figure 4).
<Each operator individually chose the template that in their opinion best fitted each residual ridge and recorded the findings in a form developed for this purpose. Later, a fourth operator brought the data in a single template, finding out lack of concordance in at least one of the three operators in 20 of the 70 upper residual ridges and in 6 of the 32 lower residual ridges. He also noticed that the error came from the curve location at the anterior area, so parameters of curve location were clarified and the evaluation was conducted once again. A 100% concordance was achieved.
Statistical analysis
Method Error
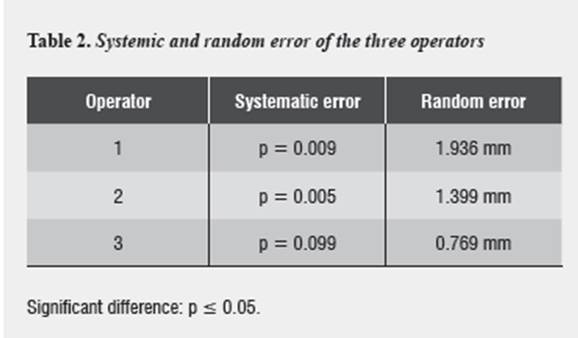
In order to standardize the cut's height at the upper ridge, each operator took the measurement two times in 25 scans; the obtained data were analyzed with the Student's t test as suggested by Houston to determine systematic errors,36 with a significance level of 0.05. To determine random error, Dahlberg coefficient37 was used (tabla 2). As the differences were statistically significant, we decided to have a cut's height no greater than 1.4 mm, repeating as many times as necessary to achieve it.
For shape and size evaluation, we only accepted a 100% concordance among the three operators.
Statistical method
The data were entered in a Microsoft Excel 2010 database, and processed in the R statistical program, version 12.2 Stat plus, version 2, 2008.
The qualitative variables were described by frequency and percentage distribution, and the quantitative variables with measures of central tendency (like average) and measures of dispersion (like standard deviation). For the bivariate analysis we used Pearson's correlation test and Fisher's exact test for frequencies below 5. A significance level of 0.05 was used in all the tests.
RESULTS
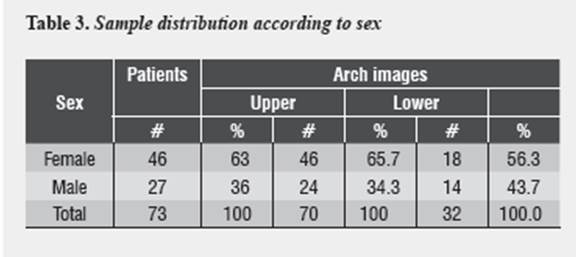
We examined 70 images of upper residual ridges and 32 images of lower residual ridges, for a total of 102 tomographic images from 73 patients. The average age was 61.31 years, with SD of ± 11,34. The minimum age was 24.67 years and the maximum was 90.17 years. Concerning the upper arch, 46 (65.71%) were female patients and 24 (34.29%) were male patients. In terms of the lower arch, 18 (56.3%) were female and 14 (43.8%) were male patients (table 3).
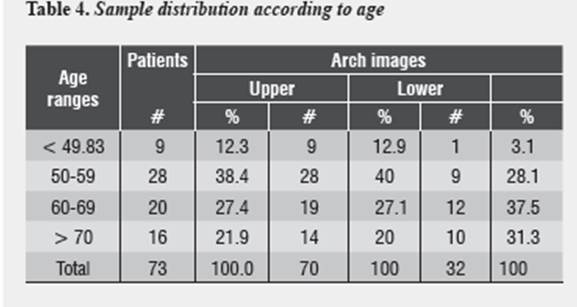
Patients were grouped in four age ranges: < 49,83 years, 9 patients (12.3%), from 50 to 59 years, 28 patients (38,4%), from 60 to 69 years, 20 patients (27.40%) and > 70 years, 16 patients (21.9%). The highest proportion (40%) of upper maxilla images was found in the range of 50 to 59 years, followed by 60 to 69 years (27.1%); concerning the lower maxilla, 37.5% of the sample were patients 60 to 69 years old, followed by 31.3% in the group of patients older than 70 years (table 4).
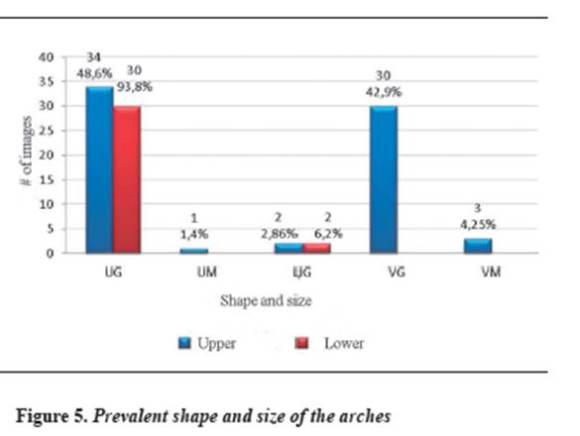
The prevalent shape and size of the upper maxilla was UG (48.6%), followed by VG (42.9%). No image presented these shape and size: ЏP, UP, VP, VP and ЏM. For the lower maxilla, the prevalent size and shape were UG (93.8%) and ЏG (6.25). No images presented this size and shape: ЏP, UP, VP, ЏM, VM, and VG, as shown in figure 5.
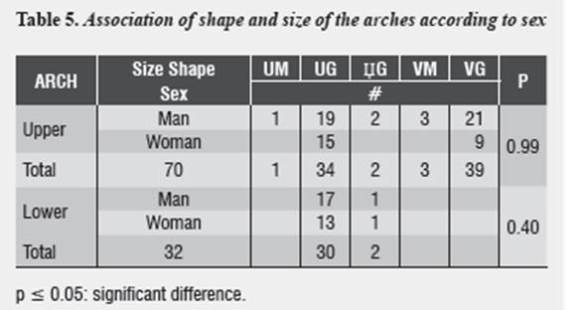
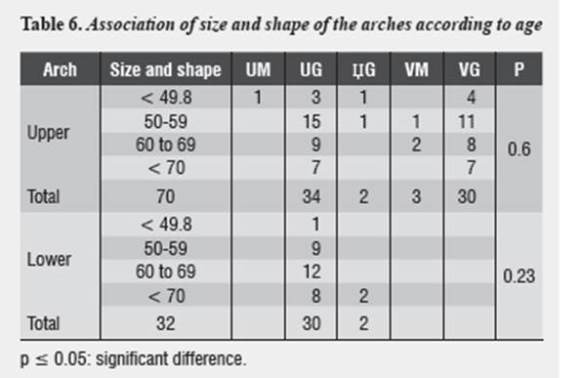
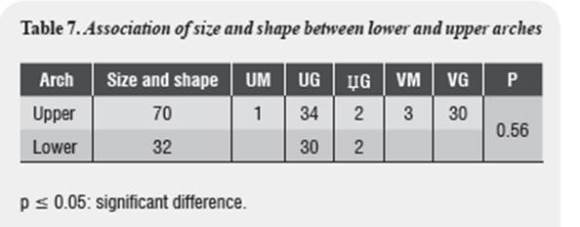
No statistically significant association was found between shape and size of upper and lower residual ridges and the variables sex and age, and no association was observed between shape and size of the upper and lower arch (p > 0.05) (tables 5, 6 y 7).
DISCUSSION
With tooth loss, the alveolar process disappears, the alveoli containing teeth roots are filled with new bone, and this alveolar process becomes residual ridge,38 which evolves during the edentulous life of patient, with constant changes due to resorption that can affect the shape and size of the arches.32 This observational cross-sectional study35 was conducted to evaluate the prevalent size and shape of the arches of edentate patients who consulted UniCIEO Diagnostic Image Center between 2010 and 2012.
We evaluated 722 patients with tomographic images of the maxillary arches, of which 73 (10.1%) met the inclusion criteria with at least one edentulous arch. The average age of patients was 60.8 ± 11,3 years and 102 tomographic images were observed, 70 residual ridges in the upper maxilla and 32 residual ridges in the lower maxilla. It is important to note that the subjects of this study were specifically undergoing evaluation for implant treatment, therefore, the proportion of edentate subjects may vary with respect to the general population.
In the present study we found out that the most prevalent upper arch shape and size was UG (48.6%), followed by VG (42.9%). For the mandible, the highest size and shape prevalence was UG (93.8%), followed by ЏG (6.25%). These are similar to the findings by Pietrokovski33 in a study on dry skulls in Israeli population, where the most prevalent arch shape was the ovoid (upper 65%, lower 77%), followed by the triangular (upper 25%, lower 12%) and the square (upper 10%, lower 11%). On the other hand, the results of the present study disagree with those of Bustillos,34 who reported a prevalence of 100% ovoid arch shape both upper and lower. His results could have been affected because arch shape was evaluated in plaster models, where connective tissue may affect the observations, as suggested by Krajicek.23 In 1993, Misch19 also mentioned that the ovoid is the most common residual ridge arch shape, followed by the square shape; however, he does not mention percentages neither prevalence reports to support this information.
EAs for the comparison of our findings with studies on dented arches, Kanashiro32 observed higher prevalence of upper arch triangular shape (73.8%) among class II division 1 Brazilian individuals. One may think then that this result was affected by alterations in parafunctional habits, often concomitant with class II, which tend to result in triangular arches. In his study in class I and class II Caucasian population, Nojima,30 reported a prevalence of lower arch triangular shape of 46.7% and 69.8% respectively. Among class I Japanese population, the most prevalent lower arch shape was the square—a finding that may be associated to race characteristics—. Among Caucasian and Japanese population, class III presents a higher prevalence of the square shape. According to the study by Varón et al31 in a sample of ideal Andean mestizo patients, there is a 6% prevalence of lower arch square shape, while the study by April28 reports a higher prevalence of lower arch square shape in class III patients (19%). According to Rai,18 residual ridge shape may not always reflect the shape of the toothed arch, but it remains fairly steady in the absence of surgical interventions. The shape differences between dentate arch and edentulous arch may also arise from the fact that the method of measuring dentate arches is more defined and the position of the teeth determines arch shape.
One of the difficulties of this study was the standardization of the coronal section of the maxilla in tomographic images, since we found a great difference in nasopalatine foramen which height, since that was the anatomical structure of reference for the image of the upper residual ridge (ranging from 1 mm to 13,52 mm). Because of this we created a method of observer calibration so that the residual ridge to be classified were the same among the three of them, with a margin of maximum error of 1,4 mm; however, according to this study, making cuts at different heights in the same patient did not produce changes in arch shape and size classification.
One of the greatest strengths of this study was that the classification of the shape and size of residual ridges was performed on tomographic images, obtaining residual ridge images through 9 default templates supplied by the Galaxis 3D software that facilitated objective, reproducible and accurate image location.39 Additionally, residual ridges were observed on bone tissue, contrary to other studies, most of which use plaster models to observe residual ridge soft tissue, which may have different shape and structure,23 and this is an important variable to take into account. One may think that using tomography to classify residual ridge shape is a very expensive and sophisticated analysis, but nowadays this type of images are common in implantology for accurate diagnosis and prognosis of edentate patients to be rehabilitated.
According to Atwood,38 the resorption of residual ridge is chronic and localized, and remodeling depends on many factors, including the bone cell viability, biomechanical (local and systemic) factors, and individual resorption patterns. Since the present study did not include the patients' medical records, it did not take into account many factors that can contribute to residual ridges remodeling, such as tooth extractions, surgical procedures such as osteotomies for this purpose, trauma during teeth dislocation that may have caused fractures in alveolar walls, periodontal status and root canal treatment due to lesions that affect the bone prior to teeth loss, time of edentulism, or type and time of prosthetic rehabilitation. Therefore, these variables were not controlled, which might have influenced the findings of the present study, thus becoming one of its limitations.
The present study did not show statistically significant associations between age and sex and residual ridge shape and size, contrary to the findings by Pietrokovski et al,26 who concluded that, over time and with prosthesis use, edentulous structures may suffer changes by slow progressive resorption, or to the findings by Suresh40 and Gur,41 who suggested that hormonal changes that women undergo during menopause may cause greater residual ridge changes and different arch shapes in comparison to men. It must also be taken into account that the sample size of this study does not reach levels of significance for associations.
Out of the 73 patients of this study, 29 (39.7%) were totally edentulous, and in 15 of them (51.7%) the upper and lower maxilla shape coincided, without statistically significant association between these variables. These results agree with the study by Misch,19 who pointed out that it is frequent that the edentulous maxillo-mandibular arches shape is not the same. This may be due to different bone resorption patterns that occur among them.
Misch21 defines the distance from the center of the anterior-most implant to a line joining the distal side of the two distal-most implants as the A-P distance, which indicates the amount of free end that can be reasonably planned, and emphasizes that the shape of dentate arches is a critical element when anterior implants are connecter to a free end of the restoration in posterior areas. A square arch shape provides a poorer prognosis than a triangular one by having a shorter A-P distance.
In clinical practice, the size and shape of the arches determines the location of implants, being fundamental when rehabilitating, as well as the intermaxillary relationship and the type of occlusion which could be simulated in finite elements studies on these nine arch shapes and sizes provided by the Galaxis 3D software.
The failures of restorations with implants in edentate patients could be analyzed with this new diagnostic tool, as it would be possible to elucidate potential variables that affect the prognosis of restorations in the long and medium term.
CONFLICTS OF INTEREST
the authors declare that they have no conflict of interest. The study was evaluated and approved by UniCIEO Ethics Committee on February 14, 2012.
CONCLUSIONS
The prevalent upper residual ridge shape was large ovoid (UG), with 48.6%, followed by large triangular (VG), with 42.9%, medium triangular (VM), with 4.29%, large square (ЏG), with 2,86% and medium ovoid (UM), with 1.43%. In the lower maxilla we only observed large ovoid (UG), with a prevalence of 93.75% and large square (ЏG), with 6.25%.
We did not find associations between size and shape of the residual arch and sex or age, both in the upper and lower maxilla.
We did not find statistically significant associations between the shape and size of upper and lower residual ridges.
REFERENCES
1. Colombia. Ministerio de Salud, Centro Nacional de Consultoría. III Estudio Nacional de Salud Bucal-ENSAB III. Bogotá: Ministerio de Salud; 1999. [ Links ]
2. Medina-Solís CE, Pérez-Núñez R, Maupomé G, Casanova-Rosado JF. Edentulism among Mexican adults aged 35 years and older and associated factors. Am J Public Health 2006; 96(9):1578-1581. [ Links ]
3. Estados Unidos. Departamento de Salud y Servicios Humanos. La salud oral en los Estados Unidos: informe del cirujano general. Resumen ejecutivo. Rockville: Departamento de Salud y Servicios Humanos de los Estados Unidos, Instituto Nacional de Investigación Dental y Craneofacial, Institutos Nacionales de la Salud; 2000. [ Links ]
4. Raga MVE, Silla JMA. Factores asociados con el edentulismo en población anciana de Valencia (España). Gac Sanit 2013; 27(2): 123-127. [ Links ]
5. Brader AC. Dental arch form related with intraoral forces: PR=C. Am J Orthod 1972; 61: 541-561. [ Links ]
6. Bonwill WGA. Geometrical and mechanical laws of articulation. Trans Odont Soc Penn 1884-1885;119-133. [ Links ]
7. Bromwell N. Anatomy and histology of the mouth and teeth, 2.a ed. Philadelphia: P Blakiston's; 1902. [ Links ]
8. Stanton FL. Arch predetermination and a method of relating the predetermined arch to the malocclusion, to show the minimum tooth movement. International Journal of Orthodontia, Oral Surgery and Radiography 1922; 8(12): 757-778. [ Links ]
9. Izard G. New method for the determination of the normal arch by the function of the face. International Journal of Orthodontia, Oral Surgery and Radiography 1927; 13(7): 582-595. [ Links ]
10. MacConaill MA, Scher EA. The ideal form of the human dental arcade, with some prosthetic application. Dent Rec (London) 1949; 69(11): 285-302. [ Links ]
11. Scott JH. The shape of the dental arches. J Dent Res 1957; 36(6): 996-1003. [ Links ]
12. Currier JH. A computerized geometric analysis of human dental arch form. Am J Orthod 1969; 56(2): 164-179. [ Links ]
13. White LW. Accurate arch-discrepancy measurements. Am J Orthod 1977; 72(3): 303-308. [ Links ]
14. Steyn CL, Harris AM, du Preez RJ. Anterior arch circumference adjustment--how much?. Angle Orthod 1996; 66(6): 457-462. [ Links ]
15. Braun S, Hnat WP, Fender DE, Legan HL. The form of the human dental arch. Angle Orthod 1998; 68(1): 29-36. [ Links ]
16. Chuck GC. Ideal arch form. Angle Orthod 1934; 4(4): 312-327. [ Links ]
17. White LW. Individualized ideal arches. J Clin Orthod 1978; 12(11): 779-787. [ Links ]
18. Rai R. Correlation of nasal width to inter-canine distance in various arch forms. J Indian Prosthodont Soc 2010; 10(2): 123-127. [ Links ]
19. Misch CE. Contemporary Implant Dentistry. Michigan: Mosby; 1993. [ Links ]
20. Jivraj S, Chee W, Corrado P. Treatment planning of the edentulous maxilla. Br Dent J 2006; 201(5): 261-279. [ Links ]
21. Misch CE. Implantología contemporánea, 3.a ed. Michigan: Mosby; 2009. [ Links ]
22. Sagat G, Yalcin S, Gultekin BA, Mijiritsky E. Influence of arch shape and implant position on stress distribution around implants supporting fixed full-arch prosthesis in edentulous maxilla. Implant Dent 2010; 19(6): 498-508. [ Links ]
23. Krajicek DD, Dooner J, Porter K. Observations on the histologic features of the human edentulous ridge. Part I: Mucosal epithelium. J Prosthet Dent 1984; 52(4): 526-531. [ Links ]
24. Baat C, Kalk W, van't Hof M. Factors connected with alveolar bone resorption among institutionalized elderly people. Community Dent Oral Epidemiol 1993; 21(5): 317-320. [ Links ]
25. Andrés-Veiga M, Barona-Dorado C, Martínez-González MJ, López-Quiles-Martínez J, Martínez-González JM. Influence of the patients' sex, type of dental prosthesis and antagonist on residual bone resorption at the level of the premaxilla. Med Oral Patol Oral Cir Bucal. 2012; 17(1): e178-e182. [ Links ]
26. Pietrokovski J, Starinsky R, Arensburg B, Kaffe I. Morphologic characteristics of bony edentulous jaws. J Prosthodont 2007; 16(2): 141-147. [ Links ]
27. Koffi JN, Koffi SG, Assi DK. Maxillary tuberosities size and shape in African Blacks total edentulous. Odontostomatol Trop 2004; 27(108):11-14. [ Links ]
28. Abril P, Rodríguez J, Zárate F. Relación de la morfología craneofacial con la forma y dimensión de los arcos dentales en la población mestiza colombiana. [Trabajo de Grado Especialista en Ortodoncia]. Bogotá: Universidad Militar Nueva Granada, Fundación CIEO; 1993. [ Links ]
29. Guzmán MS, Páez J. Dimensiones y formas de los arcos dentales en la población mestiza colombiana con oclusión normal. [Trabajo de Grado Especialista en Ortodoncia]. Bogotá: Universidad Militar Nueva Granada, Fundación CIEO; 1994. [ Links ]
30. Nojima K, McLaughlin RP, Isshiki Y, Sinclair PM. A comparative study of Caucasian and Japanese mandibular clinical arch forms. Angle Orthod 2001; 71(3): 195-200. [ Links ]
31. Varón A, Mejía E, García P, Gómez M. Valoración de la forma del arco dentario respecto a su forma individualizada y la curva MBT correspondiente en el grupo poblacional colombiano con el cual se determinaran los rangos de referencia para la cefalometría Optava. [Trabajo de Grado Especialista en Ortodoncia]. Bogotá D.C.: Universidad Militar Nueva Granada-Fundación CIEO. Posgrado de Ortodoncia; 2002. [ Links ]
32. Kanashiro LK, Vigorito JW, Domínguez GC, Tortamano A. Estudo da prevalência das formas de arcos preconizadas pela filosofia MBT, em indivíduos com má-oclusão de classe II, divisão 1ª e diferentes tipos faciais. Ortodontia 2005; 38(3): 229-235. [ Links ]
33. Pietrokovski J, Harfin J, Levy F. The influence of age and denture wear on the size of edentulous structures. Gerodontology 2003; 20(2): 100-105. [ Links ]
34. Bustillos L, Terán AA, Arellano L. Estudio de la forma y taman~o de maxilares edéntulos de pacientes de la ciudad de Mérida, Venezuela. Revista Odontológica de Los Andes 2008; 3(1): 20-25. [ Links ]
35. Levin KA. Study design I. Evid Based Dent 2005; 6(3):78-79. [ Links ]
36. Houston WJ. The analysis of errors in orthodontic measurements. Am J Orthod 1983; 83(5): 382-390. [ Links ]
37. Harris EF, Smith RN. Accounting for measurement error: a critical but often overlooked process. Arch Oral Biol 2009; 54 Supl 1:S107-S117. [ Links ]
38. Atwood DA. Some clinical factors related to rate of resorption of residual ridges. 1962. J Prosthet Dent 2001; 86(2):119-125. [ Links ]
39. Sheikhi M, Ghorbanizadeh S, Abdinian M, Goroohi H, Badrian H. Accuracy of linear measurements of Galileos cone beam computed tomography in normal and different head positions. Int J Dent 2012; 2012: ID 214954. [ Links ]
40. Suresh S, Sumathy G, Banu MR, Kamakshi K, Prakash S. Morphological analysis of the maxillary arch and hard palate in edentulous maxilla of South Indian dry skulls. Surg Radiol Anat 2012; 34(7):609-617. [ Links ]
41. Gur A, Nas K, Kayhan O, Atay MB, Akyuz G, Sindal D, et al. The relation between tooth loss and bone mass in postmenopausal osteoporotic women in Turkey: a multicenter study. J Bone Miner Metab 2003; 21(1):43-47. [ Links ]
