










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
versión impresa ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.26 no.1 Medellín jul./dic. 2014
ORIGINAL ARTICLES DERIVED FROM RESEARCH
CHEWING SIDE PREFERENCE IN CHILDREN WITH CLEFT PALATE: CONCORDANCE OF THREE METHODS
Olga Patricia López Soto;1 Lina María López Soto;2 Alejandro Osorio Forero;3 Francia Restrepo de Mejía4
1 DMD. DMD, Specialist in Research and Higher Education. Oral Health Re-
search Group (INSAO). Universidad Autónoma de Manizales, Colombia.
Email: sonrie@autonoma.edu.co
2 Speech therapist, Myofunctional therapist. Oral Health Research
Group (INSAO). Universidad Autónoma de Manizales, Colombia
3 Biomedical Engineer. Neurolearning Research Group. Universidad
Autónoma de Manizales, Colombia
4 Medical Physiatrist, Ph.D in Social Sciences, Childhood and Youth
Studies. Neurolearning Research Group. Universidad Autónoma de
Manizales, Colombia
SUBMITTED: DECEMBER 3/2013-ACCEPTED: MAY 7/2014
López OP, López LM, Osorio A, Restrepo F. Chewing side preference in children with cleft palate: concordance of three methods. Rev Fac Odontol Univ Antioq 2014; 26(1): 89-105.
ABSTRACT
INTRODUCTION: the objective was to measure the concordance of three methods to determine chewing side preference in children with cleft palate.
METHODS: the sample included 47 children with cleft palate and similar age and socioeconomic level. Methods: the test
of Christensen & Radue (1985), the test of Paphangkorakit et al (2006) and surface electromyography (sEMG) were used. Comparisons among
groups were made by non-parametric methods.
RESULTS: the method of Paphangkorakit et al (2006) did not show concordance with the preference
measured by the Christensen & Radue method (1985) (Pearson's X2 = 0.96, p = 0,619; Kappa = ?0.08, p = 0,475). The results showed that
cleft type is not associated to chewing side preference measured by the method of Paphangkorakit et al (2006) (Pearson's ?2 = 5.07; p = 0,281;
Kappa = 0.07, p = 0,274) but by the method of Christensen & Radue (1985) (Pearson's ?2 = 7.09; p = 0.029; weak Cramer's V association = 0.39,
p = 0.029; Kappa = 0.19, p = 0.009). Patients with right cleft palate differ from patients with bilateral cleft in terms of sEMG amplitude asymmetry
while chewing (right: 7.3 ± 12.8; bilateral: ?2.67 ± 6.61; U = 104; p = 0,038).
CONCLUSIONS: no concordance was found between the two studied
clinical methods to identify masticatory preference, nor between these and sEMG.
Key words: cleft palate, mastication, surface electromyography.
INTRODUCTION
Normal mastication is characterized by unilateral cycles, with periodic food alternation on both sides of the dental arches, although fewer unilateral cycles have been observed with homogeneous soft foods. Once food takes consistency, homogeneity and cohesiveness and is ready to be swallowed, bilateral cycles may occur.1 Studying patterns of chewing side is useful to understand the neural control of mastication and to design dental treatments. Previous studies have shown that most people normally chew more on either the right or the left side, which is known as ''preferred chewing side''.2 Some studies have concluded that chewing side preference is not related to hand side preference3, 4 and is not associated with tooth contact area5 or chewing side efficiency.6 Hannam et al7 suggested that preferred chewing side was connected with the ability to move the mandible laterally towards the preferred side. Preferred chewing side has usually been determined by the percentage of right or left masticatory cycles using subjective clinical assessments. However, Wilding and Lewin2 propose to overcome this limitation by using computational methods that allow quantifying left and right closing contacts by means of a graphic interface.
Preferred chewing side has been defined by Christensen and Raude as follows: ''when mastication is consistently or predominantly done on the right or left side of dentition''.3 Usually, people alternate mastication between one side and the other, but when it is preferably done on one side it may cause uneven loading on the temporomandibular joint (TMJ). One of the conditions of occlusal stability is to alternately chew on both sides of the dental arch and to protrude during incision.8-10 Besides maintaining occlusal balance, a bilateral alternated mastication with wide excursions, physiological occlusal contacts, bilateral synchronous muscular activity, and the application of uniform forces on supporting tissues produces adequate stimuli for normal sagittal and transversal development of mandible and maxilla, directly and indirectly participating in the prevention of periodontal alterations and TMJ disorders.10 Moreover, occlusal balance is one of the objectives of oral rehabilitation, and understanding masticatory pattern changes can help assessing the effect of malocclusion in the oral functions of children and adults.11 Having a preferred chewing side is considered by McDonnell et al as inefficient chewing.12
A variety of methods can be used to determine chewing side preference; for example, McDonnell's team12 used kinesiography, a technique that allows observing the movement of maxillaries without blocking their normal functioning. Christensen and Radue3 used the visual method of observing at previously defined times, which consists of a series of checkups after chewing gum for seven consecutive periods of time—this method has been reported as one of the most accurate—.13 Paphankorakit et al14 described a method using a video camera to record the movement of the chin with respect to other two reference points vertically marked along the midline facial; slow-speed video analysis is used to identify chewing side in each cycle. Moller15 used surface electromyography (sEMG) and proposed it as a reliable method considering that myoelectric activity levels are higher in the masseter muscles of the chewing side compared to the side with no masticatory activity.16, 17
Although mastication can be done with unilateral movements, this does not represent a practical occlusal function. Unilateral chewing exerts different stimuli between the working side and the balance side, causing a non-harmonious development of the facial skeleton.18, 19 The referenced studies on cleft palate analyze movements and masticatory efficiency in these patients.20, 21 However, they are not intended to determine preferred chewing side.
This study attempted to determine chewing side preference in children with cleft palate by means of three methods: the Christensen & Radue method, the Paphangkorakit method, and surface electromyography.
METHODS
This analytical study included a sample by convenience of 47 children (7-14 years of age) with cleft palate (left: 12, right: 22, bilateral: 13) and similar socioeconomic levels, who were receiving multidisciplinary care at health centers in the cities of Manizales, Pereira and Armenia. The treatment protocol these patients received was accepted by the two foundations from the Eje Cafetero where the kids were being seen; it included psychological attention, speech therapy, maxillary and functional orthopedics, and orthodontics. The inclusion criterion was presence of cleft palate in the specified age range. The study was approved by Universidad Autónoma de Manizales Ethics Committee by Agreement N° 12 of February 2, 2011, and it complied with all the requirements of Standard 8430 regarding health research in patients. Parents or guardians of the schoolchildren were informed about the process in which they were participating, and they signed an informed consent before examinations started. Similarly, the children were requested authorization to be included in the study.
Application of Paphangkorakit & partners' test (2006)
Each patient was marked with three reference points on the skin, one at the most prominent part of the nose, one just below the center of the lower lip and another on the chin, forming a vertical line. Patients were asked to keep their heads still during all the tests. The tests were recorded with a video camera (Samsung SMX-C200BN/XAO) facing the patients and located 1 m from them; the zoom function was activated in order to cover the area marked with cue points. A plastic ruler was placed over the facial midline to determine chin movement pattern while projecting the recordings. By using this method, most cycles could be identified as either ''right'' or ''left''; cycles that were not clearly identified due to the presence of indistinguishable transverse movements were marked as ''not conclusive'' (NC). This method was validated by Paphangkorakit et al 14 with a Kappa coefficient of 0.70 to 0.83. In order to control bias in interpreting preferred chewing side, the recording was analyzed by a trained pediatric dentist not associated to the research group, in order to control possible internal bias.
Application of Christensen & Radue's test (1985)
Applying the modified technique of ''place control to determine chewing side'', described by Christensen and Radue,3 implied providing patients with 28 gr of sugar-free gum, asking them to normally chew it with their posterior teeth, without explaining the purpose of the test.15 seconds later, patients were requested to stop and squeeze the gum between their teeth, in order to observe the position of the chewing gum and to determine whether it was on the right side or the left side. This procedure was performed seven times consecutively.
Surface electromyography procedure
Registration of sEMG was performed with an electrophysiograph and Cadwell's® Sierra® Wave® software. Acquisition parameters were adjusted to 76.8 kHz of sampling frequency, a band-pass filter of 10-10,000 Hz and 200 µV gain. The sEMG protocol of record collection and archiving was chosen. Stainless steel Cadwell® disc electrodes 302139-200 of 10 mm in diameter were used.
In order to collect sEMG records, the schoolchildren were sitting on a chair with backrest, keeping their backs straight and in a state of relaxation. Before placing the electrodes, their faces were wiped with cotton and 95% ethanol. Cadwell® 202153-000 conductive gel was used to reduce the appearance of artifacts due to low conductance. The ground electrode, common to all other pairs of electrodes, was placed 2 cm above the nasion.
This study evaluated the activity of the right and left masseter by choosing a bipolar configuration which is sensitive to changes in the force exerted by muscles.22 The electrodes were positioned on the masseter in the following way: patients were requested dental closure at its maximum strength, the masseter was felt, an active electrode was located at the motor point and a reference electrode was placed 1 cm below the ear lobe. Each muscle was evaluated independently. This study analyzed muscle activity amplitude while patients were chewing gum and until the software recorded 6 averages of predominant patterns of amplitude interference. In this context, sEMG amplitude corresponds to the amplitude of the peak-to-peak voltage of the interference pattern while performing the actions.
Muscle activity asymmetry was calculated as described, like this:
Where MD and MI correspond to the sEMG amplitude of the left and right masseters respectively.
Statistical analysis
The program SPSS® (IBM, V20) was used for statistical analysis. Qualitative variables association was observed with Pearson's X2 test and Phi coefficients or Crammer's V. Comparisons of patients with right and left chewing preference were conducted with the Mann-Withney U test. The Kruskall-Wallis H test was used to analyze variance of quantitative measures among patients with three types of cleft, and comparisons were made with the Mann-Withney U test.
RESULTS
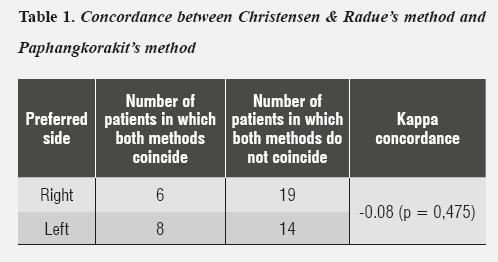
In this group of patients, chewing preference determined by the method of Paphangkorakit et al 14 did not show associations with the preference determined by Christensen & Radue's method3 (Pearson's X2 = 0.96, p = 0.619; Kappa = –0.08, p = 0,475) (table 1).
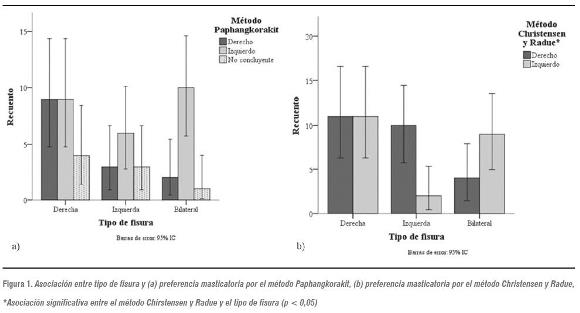
In addition, cleft type is not associated with chewing side preference according to the method of Paphangkorakit et al 14 (Pearson's X2 = 5.07; p = 0.281; Kappa = 0.07, p = 0.274) (figure 1.a), but it is according to the method of Christensen & Radue3 (Pearson's X2 = 7.09; p = 0.029 Cramer's V weak association = 0.39; p = 0.029; Kappa = 0.19, p = 0.009). With this method, most children with left cleft showed right chewing preference and children with bilateral cleft showed left chewing preference; the same amount of children with right cleft have both left and right preferences (figure 1.b).
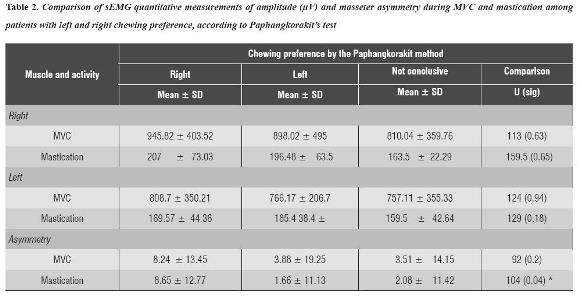
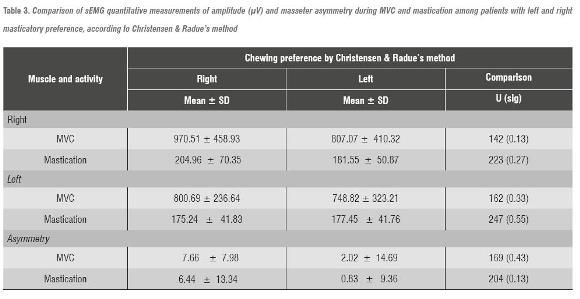
Patients with left chewing preference measured with the Paphangkorakit method differ from those with right preference in terms of masseters' sEMG asymmetry of amplitude during mastication (U = 104; p = 0.038) (table 2). This result did not show when comparing patients with left and right preferences, measured with the method of Christensen and Radue (table 3).
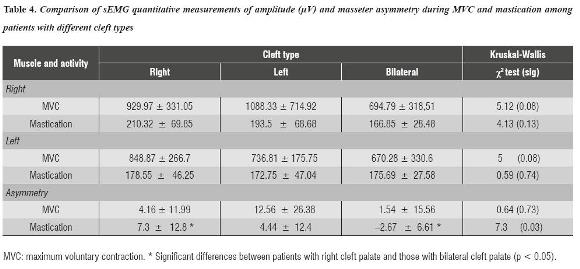
The variance of asymmetry of the masseters' sEMG activity may be explained by cleft type (Kruskal- Wallis X2 = 7.30, p = 0.026). This result is mainly due to the difference between subjects with unilateral right cleft and those with bilateral cleft (U = 49; p = 0.115) and not by the difference between subjects with unilateral left cleft and those with bilateral cleft (U = 104; p = 0.038) or by left and right cleft (U = 106; p = 0.349) (table 4).
DISCUSSION
This study associated the results of two methods to determine preferred chewing side with sEMG amplitude in cleft palate patients. Most studies that propose methods to identify preferred chewing side have included relatively small samples and normal subjects only.2, 23, 24 As far as we know, this is the first study that considers this condition in cleft palate patients and it also exceeds the sample size of previous studies with a sample of 47 subjects.
This study found no correlation between the analyzed clinical methods to identify masticatory preference. Likewise, Varela et al13 found no correlation between the test proposed by Kazazoglu et al25 and kinesiography.2 On the contrary, by comparing two methods of determining preferred masticatory side using visual observation and kinesiography, Varela et al 13 found out a marked preference to the right side and this preference was independent of the method used to determine it. It has been reported that masticatory cycles alter their pattern in accordance with food hardness and size and by rheological properties—and this seems to explain why the studies obtain diverse results.26, 27
By studying the relationship between chewing preference and sEMG, Christensen and Radue28 found a significant association in terms of right masticatory preference only. In the present study, we also found that most patients with right preference showed greater sEMG amplitude during mastication, but not in a significant way. In this study, the masseters' sEMG asymmetry of amplitude during mastication was associated with chewing preference as measured with the method of Paphangkorakit et al. Patients with right preference show asymmetry towards this side.
It has been reported that preferred chewing side determined by sEMG and observation are significantly correlated,29 but other studies, such as those by Hoogmartens & Caubergh30 and Kazazoglu, Heath & Müller,25 question the applicability of electromyography for this purpose.
Bilateral mastication is considered to be more common than reported in the literature.31 In corroborating this assumption, Farias et al 32 found that 63% of 78 participants had bilateral mastication. Bilateral mastication has been considered efficient;33 in addition, Minato et al34 showed that bilateral masticators have a more sensitive tongue—a characteristic that may play an important role in masticatory efficiency.
While some studies conclude that chewing preference is not a fixed human trait,14 some others consider that most people do have this pattern;35 they even suggest that the right side is prevalent among the studied populations13, 24 regardless of laterality.3 This study did not find a global chewing preference in the population with the Christensen and Radue method, but most patients showed left preference when applied the Paphangkorakit method.
The existence of a preferred chewing side may have implications in saliva production and distribution around the mouth. McDonnell and Hector36 showed that saliva produced by children in one side of the mouth (presumably by masticatory saliva reflex) does not tend to be distributed around the mouth—which has consequences in oral and dental health.
McDonnell, Hector and Hannigan found few differences between the proportion of children who preferred chewing by the right side or the left side, but they did find a statistically significant association between dentition status and the result of the Christensen and Radure test in the presence of predominant side preference.
By analyzing cleft type (bilateral, left unilateral and right unilateral) in relation to chewing preference, a significant association was found only when the method of Christensen and Radeu was used. Most patients with left unilateral cleft palate prefer chewing on the right side, while patients with bilateral cleft prefer chewing on the left side.
In the study by Christensen and Radue,28 the sEMG records showed that chewing side could be reliably detected by considering the record with the highest level of myoelectric activity but only on the right side, which may create confusion in applying this principle. This has not been consistent with Riise findings.37 However, it should be noted that the contralateral muscle occasionally showed the highest level of activity.
A number of peripheral factors prevent the activity of masticatory muscles from being pushed towards both sides by the motor unit, such as the presence of a preferred masticatory side, occlusal stability, food size and consistency, and mandible orientation, which is in turn related to the length of the sarcomere muscle.38, 39 However, a significant number of observations showed agreement between sEMG and the masticatory side in use by observing gum chewing or the Christensen and Radue method. These researchers did not find concordance between their method and the results obtained with sEMG, as happened in the present study.
The absence of significant differences in the masseters' sEMG activity observed among patients with different cleft types suggests a symmetric function of the masticatory muscles during mastication despite the presence of alterations. Therefore, patients with unilateral cleft palate may have developed adaptive responses to morphological alterations to achieve functional mastication, as suggested by Andrade et al.40
Examination and registration of preferred side deserve further consideration during routine dental examination and treatment.41 According to researchers like Farias et al,32 masticatory performance is not correlated with a defined movement pattern, which prevents establishing differences between uni- and bilateral masticators; however, according to these authors, bilateral chewing promotes better masticatory performance.
CONCLUSIONS
There are sEMG amplitude differences between patients with right cleft palate and those with bilateral cleft palate. No concordance was found between the two studied clinical methods to identify chewing preference, nor between these and sEMG.
RECOMMENDATIONS
There are many questions still to be answered regarding masticatory mechanisms. Our results suggest that current methods to establish preferred chewing side do not show significant levels of concordance; therefore, there needs to be further research to provide objective easily replicable methods.
CONFLICTS OF INTEREST
The authors declare having no conflicts of interest.
ACKNOWLEDGEMENTS
The authors thank the Sonríe and Abrazar foundations for their support gathering the sample, and Universidad Autónoma de Manizales for providing the necessary resources for this study (Project: 235-025). The authors declare that there no conflicts of interest.
REFERENCIAS
1. Alexander RM. News of chews: the optimization of mastication. Nature 1998; 391(6665): 329. [ Links ]
2. Wilding RJ, Lewin A. A model for optimum functional human jaw movements based on values associated with preferred chewing patterns. Arch Oral Biol 1991; 36(7): 519-523. [ Links ]
3. Christensen LV, Radue JT. Lateral preference in mastication: a feasibility study. J Oral Rehabil 1985; 12(5): 421-427. [ Links ]
4. Hoogmartens MJ, Stuyck J, Bockx E, Cheng N, Jacobs G, Nijs J et al. Stretch sensitivity of primary spindle endings in masseter and temporalis muscles: lateralization and association with unilateral preference pattern of mastication. Electromyogr Clin Neurophysiol 1980; 20(4- 5): 369-381. [ Links ]
5. Wilding RJ, Adams LP, Lewin A. Absence of association between a preferred chewing side and its area of functional occlusal contact in the human dentition. Arch Oral Biol 1992; 37(5): 423-428. [ Links ]
6. Wilding RJ. The association between chewing efficiency and occlusal contact area in man. Arch Oral Biol 1993; 38(7): 589-596. [ Links ]
7. Hannam AG, De Cou RE, Scott JD, Wood WW. The relationship between dental occlusion, muscle activity and associated jaw movement in man. Arch Oral Biol 1977; 22(1): 25-32. [ Links ]
8. Okeson J. Tratamiento de los trastornos funcionales del sistema masticatorio. En: Tratamiento de Oclusión y afecciones temporomandibulares. Madrid: Mosby; 2003. p. 39-43. [ Links ]
9. Simões WA. Visão do crescimento mandibular e maxilar; Insights on maxillary and mandibular growth for better practice. J Bras Ortodon Ortop Facial 1998; 3(15): 9-18. [ Links ]
10. Pignataro Neto G, Bérzin F, Rontani RMP. Identificação do lado de preferência mastigatória através de exame eletromiográfico comparado ao visual. Dental Press J Orthod 2004; 9: 77-85. [ Links ]
11. Gibbs CH, Wickwire NA, Jacobson AP, Lundeen HC, Mahan PE, Lupkiewicz SM. Comparison of typical chewing patterns in normal children and adults. J Am Dent Assoc 1939; 1982; 105(1): 33-42. [ Links ]
12. Mc Donnell ST, Hector MP, Hannigan A. Chewing side preferences in children. J Oral Rehabil 2004; 31(9): 855- 860. [ Links ]
13. Varela J, Castro N, Biedma B, da Silva Domínguez J, Quintanilla J, Muñoz F et al. A comparison of the methods used to determine chewing preference. J Oral Rehabil 2003; 30(10): 990-994. [ Links ]
14. Paphangkorakit J, Thothongkam N, Supanont N. Chewingside determination of three food textures. J Oral Rehabil 2006; 33(1): 2-7. [ Links ]
15. Moller E. Action of the muscles of mastication. Front Oral Biol 1974; 1: 121-158. [ Links ]
16. Mohamed SE, Christensen LV, Harrison JD. Tooth contact patterns and contractile activity of the elevator jaw muscles during mastication of two different types of food. J Oral Rehabil 1983; 10(1): 87-95. [ Links ]
17. Sheikholeslam A, Riise C. Influence of experimental interfering occlusal contacts on the activity of the anterior temporal and masseter muscles during submaximal and maximal bite in the intercuspal position. J Oral Rehabil 1983; 10(3): 207-214. [ Links ]
18. Poikela A, Kantomaa T, Tuominen M, Pirttiniemi P. Effect of unilateral masticatory function on craniofacial growth in the rabbit. Eur J Oral Sci 1995; 103(2): 106-111. [ Links ]
19. Poikela A, Kantomaa T, Pirttiniemi P. Craniofacial growth after a period of unilateral masticatory function in young rabbits. Eur J Oral Sci 1997; 105(4): 331-337. [ Links ]
20. Hideshima M. Masticatory movements in cleft lip and palate patients with unilateral buccal cross-bite. The effect of different buccal overlap on pattern of chewing. Nihon Hotetsu Shika Gakkai Zasshi 1989; 33(5): 1168-1182. [ Links ]
21. Ravera MJ, Miralles R, Santander H, Valenzuela S, Villaneuva P, Zúñiga C. Comparative study between children with and without cleft lip and cleft palate, Part 2: Electromyographic analysis. Cleft Palate Craniofac J 2000; 37(3): 286-291. [ Links ]
22. Gabriel DA. Effects of monopolar and bipolar electrode configurations on surface EMG spike analysis. Med Eng Phys 2011; 33(9): 1079-1085. [ Links ]
23. Gisel EG. Development of oral side preference during chewing and its relation to hand preference in normal 2-to 8-year-old children. Am J Occup Ther 1988;42(6): 378- 383. [ Links ]
24. Delport H, De Laat A, Nijs J, Hoogmartens M. Preference pattern of mastication during the first chewing cycle. Electromyogr Clin Neurophysiol 1983; 23(6): 491-500. [ Links ]
25. Kazazoglu E, Heath M, Müller F. A simple test for determination of the preferred chewing side. J Oral Rehabil 1994; 21(6): 723-724. [ Links ]
26. Yamashita S, Hatch JP, Rugh JD. Does chewing performance depend upon a specific masticatory pattern? J Oral Rehabil 1999; 26(7): 547-553. [ Links ]
27. Foster KD, Woda A, Peyron MA. Effect of texture of plastic and elastic model foods on the parameters of mastication. J Neurophysiol 2006; 95(6): 3469-3479. [ Links ]
28. Christensen LV, Radue JT. Lateral preference in mastication: an electromyographic study. J Oral Rehabil 1985; 12(5): 429-434. [ Links ]
29. Saifuddin M, Miyamoto K, Ueda HM, Shikata N, Tanne K. A quantitative electromyographic analysis of masticatory muscle activity in usual daily life. Oral Dis 2001; 7(2): 94- 100. [ Links ]
30. Hoogmartens M, Cauberg M. Cheuring side preference during the first cheuring cycle as a new type of lateral preference in man. Electromyogr Clin Neurophysiol 1987; 27(1): 3-6. [ Links ]
31. Mioche L, Hiiemae KM, Palmer JB. A postero-anterior videofluorographic study of the intra-oral management of food in man. Arch Oral Biol 2002; 47(4): 267-280. [ Links ]
32. Farias Gomes SG, Custodio W, Moura Jufer JS, Del Bel Cury AA, Rodrigues Garcia RCM. Correlation of mastication and masticatory movements and effect of chewing side preference. Braz Dent J 2010; 21(4): 351- 355. [ Links ]
33. Wilding RJ, Lewin A. The determination of optimal human jaw movements based on their association with chewing performance. Arch Oral Biol 1994;39(4): 333-343. [ Links ]
34. Minato A, Ono T, Miyamoto JJ, Honda E-i, Kurabayashi T, Moriyama K. Preferred chewing side-dependent two-point discrimination and cortical activation pattern of tactile tongue sensation. Behav Brain Res 2009; 203(1): 118-126. [ Links ]
35. Pond LH, Barghi N, Barnwell GM. Occlusion and chewing side preference. J Prosthet Dent 1986; 55(4): 498-500. [ Links ]
36. McDonnell ST, Hector MP. The distribution of stimulated saliva in children. Int J Paediatr Dent 2001; 11(6): 417- 423. [ Links ]
37. Riise C. Clinical and electromyographic studies on occlusion. Estocolmo: Department of Stomatognathic Physiology, Karolinska Institutet; 1983. [ Links ]
38. Bakke M, Michler L, Moller E. Feedback of bolus on elevator activity during mastication. J Dent Res 1983; 62: 653. [ Links ]
39. Stålberg E, Eriksson PO, Antoni L, Thornell LE. Electrophysiological study of size and fibre distribution of motor units in the human masseter and temporal muscles. Arch Oral Biol 1986; 31(8): 521-527. [ Links ]
40. Andrade Ad S, Gavião MB, Gameiro GH, De Rossi M. Characteristics of masticatory muscles in children with unilateral posterior crossbite. Braz Oral Res 2010; 24(2): 204-210. [ Links ]
41. Nissan J, Gross MD, Shifman A, Tzadok L, Assif D. Chewing side preference as a type of hemispheric laterality. J Oral Rehabil 2004; 31(5): 412-416. [ Links ]
