










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
versión impresa ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.26 no.1 Medellín jul./dic. 2014
ORIGINAL ARTICLES DERIVED FROM RESEARCH
PREVALENCE OF DENTAL ENAMEL DEFECTS IN CHILDREN AND ADOLESCENTS FROM PASTO, COLOMBIA1
Ana Cristina Mafla2; Doris Lucía Córdoba Urbano3; Maritza Natalia Rojas Caicedo4; Manuel Alejandro Vallejos de la Rosa4; María Fernanda Erazo Sánchez4; Juliana Rodríguez Caicedo4
1 This study was suppor ted by Universidad Cooperativa de Colombia,
Pasto.
E-mails: ana.mafla@campusucc.edu.co, anamaff@yahoo.com
2 DMD, MS in Public Health. Head of the Grupo de Investigaciones en
Odontología (GIOD). School of Dentistry, Universidad Cooperativa de
Colombia, Pasto
3 DMD, Specialist in Healthcare Management and Quality Audit.
Researcher Professor. School of Dentistry, Universidad Cooperativa
de Colombia, Pasto
4 Dentistry Students. School of Dentistry, Universidad Cooperativa de
Colombia, Pasto
SUBMITTED: MAY 28/2013-ACCEPTED: MAY 12/2014
Mafla AC, Córdoba DL, Rojas MN, Vallejos MA, Erazo MF, Rodríguez J. Prevalence of dental enamel defects in children and adolescents from Pasto, Colombia. Rev Fac Odontol Univ Antioq 2014; 26(1): 106-125.
ABSTRACT
INTRODUCTION: the objective of this study was to estimate the prevalence of dental enamel defects (ED) in children and adolescents
from Pasto, Colombia.
METHODS: five hundred and ninety-nine children and adolescents aged 6 to 15 years from three municipalities of Pasto,
Colombia were clinically examined for fluoride opacity and enamel hypoplasia. Scientific literature and color photographs of the oral cavity were
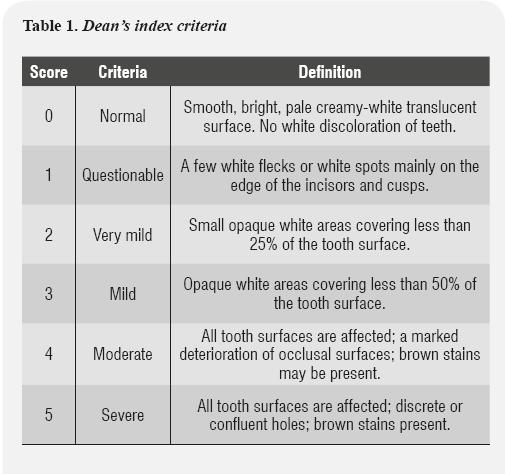
previously studied by two examiners in order to diagnose ED in these municipalities. Severity of fluoride opacity was assessed with Dean's index
and enamel hypoplasia with Silberman's index.
RESULTS: ED prevalence in children and adolescents was 49.9% (95% CI: 45.8% - 53.9%). Most of
them, 85.3%, had fluoride opacities (FOP) and 14.7% enamel hypoplasia. The predominant type of FOP severity was the moderate level (73.7%).
FOP were more prevalent in females (86.3%) than in males (84.2%) (p > 0.05), while enamel hypoplasia was more frequent in males (15.8%) than
in females (13.7%) (p > 0.05). Enamel hypoplasia appeared as creamy-white and brown lesions and were most frequently found in permanent upper
central incisors.
CONCLUSIONS: ED prevalence was high in these municipalities. Fluoride opacities were the most frequent and were classified as
moderate according to Dean's index. New studies are required to establish levels of fluoride exposure in these communities. Certainly, these findings
represent a public health problem..
Key words: dental fluorosis, dental enamel hypoplasia, epidemiology, oral health, children, adolescents.
INTRODUCTION
Pasto is the capital city of the state of Nariño, located in southwestern Colombia. This city has a population of approximately 424,283 inhabitants. It is situated in the Atrís Valley or Hatunllacta (Quechua language) on the Andes mountain range and has an altitude of 8,290 Ft (2,527 m) above sea level. This region is close to the Galeras volcano (9.32 miles). Our study was conducted in the municipalities of Catambuco, Buesaquillo and El Encano in the surroundings of Pasto. They are located 1.2, 10.5, and 21.7 miles away from the volcano (14,028 ft) respectively. These localities are low-income communities. Agriculture is still the most essential segment of the region's micro-economy and potatoes, onions, corn and vegetables are by far the most important crops. Hand cultivation using tools such as machetes and hoes is predominant and family members participate in this agricultural activity. Farming practices such as livestock breeding are also common and their main purpose is to produce dairy products, fertilizers and farm work tools.
Developmental enamel defects (DED) show deviations from the normal translucent appearance of tooth enamel, as a result of a dysfunctional enamel organ.1 They can be either quantitative, appearing as deficient enamel thickness —or enamel hypoplasia (EH)— or qualitative (hypomineralization), clinically observed as enamel opacity (EO).2 DED can have a negative impact on oral health and esthetics, including caries susceptibility, increased dental wear, tooth sensitivity3 and unfavorable dental aesthetic perception.4
The etiology of DED is not fully clear. Genetic factors such as amelogenesis imperfecta are involved, as well as environmental factors such as fluoride and medicine intake, nutritional deficiencies, prenatal infections, chicken pox and other early childhood diseases. The importance of socioeconomic factors is evident, as DED are much less prevalent in developed countries with good nutrition. Comparing the clinical presentations of defects can provide insights about the ameloblasts response to environmental aggressions in primary and permanent dentitions, and thereby facilitate the identification of etiological agents.5 Since the etiology of DED include genetic and environmental factors, localities characterized by economic deprivation and environmental variations should be taken into account to measure enamel defects such as fluoride opacities and enamel hypoplasia.
Dental enamel opacities associated with fluoride intake have been long reported.6-9 Thylstrup and Fejerskov10 stated that fluorosis is associated with increased hypomineralization and greater enamel porosity. In mild forms, it appears as chalky white lines on the enamel, which are usually symmetrical in contra-lateral teeth following the pathways of the perikymata. In severe forms, the entire tooth surface is characterized by holes and yellow, brown or black spots.10 Potential sources of fluoride identified as strong enough to cause fluorosis during childhood include community water supplies fluoridated above optimum dilution of concentrated, powdered infant formula prepared with fluoridated water, inappropriate use of fluoride or fluoridated vitamin supplements, unintentional intake of fluoridated toothpaste during brushing, and possible dietary practices of high consumption of fish or tea.11
In addition, volcanoes represent the main natural constant source of fluorine,12 one of the main sources of fluoride in our community might be related to ''Galeras'' volcano. Currently, this volcano shows a continuous activity in this region— the last emission was in March 2014—. An open channel constantly degassing into the atmosphere as the main source of fluorine can be a source of contamination of water resources close to volcanoes.
In two volcanic systems, high deposits of magmatic fluorine have been associated to human fluorosis.13
Diverse indexes or classification systems have been used in surveys to measure the presence and severity of enamel fluorosis. However, Dean's14 classification system has been the most frequently used for years for fluorosis assessment. Regarding prevalence of dental fluorosis in 6 to 15 year-old Mexican children, opacities by fluoride were found in 52.6%, of which 11.8% were moderate and 2.6% were severe15 according to Dean's index. In cities surch as Medellín, Colombia, dental fluorosis was observed in 81%16 in this age group. In addition, regarding severity, in different regions of the state of Caldas, dental fluorosis appeared in 63.3% and 56.3% as very slight and mild respectively.17
On the other hand, enamel hypoplasia is an exclusive ectodermal disturbance related to alterations in the matrix of organic enamel, which can cause white spots, narrow horizontal bands, lines of small holes, cracks, and teeth discoloration, ranging from yellow to dark brown.18 It is also a qualitative defect of dental enamel, clinically characterized during the early post-eruptive period as a creamy-white and/ or yellowish-brown discolored demarcated area of variable size.19-20 Moreover, enamel hypoplasia in permanent dentition has been diagnosed as an effect of traumatic injuries in primary dentition.21 One classification system has been developed by Silberman et al.22 In Cartagena, Colombia, the prevalence of enamel hypoplasia has been found in 6% of 5-12 year-old children.23
Although fluorosis opacity and enamel hypoplasia have been reported in Colombia, few epidemiological studies have assessed their magnitude in the geographical area of the city of Pasto. The objective of our study was therefore to estimate the prevalence of these dental enamel defects in children and adolescents from this Colombian region.
METHODS
Study population
A cross-sectional clinical evaluation of 599 volunteer children and adolescents was carried out from August 2011 to August 2012. The study was conducted in three schools from municipalities located in Pasto, Colombia, where low-income students were enrolled. These three municipalities had 42,650 inhabitants approximately. The sample included 174 subjects from Institución Educativa Municipal (IEM) Santa Teresita in Catambuco, 190 individuals from IEM El Encano in El Encano, and 235 from IEM Eduardo Romo Rosero in Buesaquillo.
The inclusion criteria was subjects aged 6 to 15 years because the eruption process begins in permanent dentition after a period of mineralization in early months and years. These dental enamel defects may onset and be easily diagnosed during this period. This study's design also included male and female children and adolescents, whose parents signed a consent form the day of evaluations. The following municipalities were included: towns with larger amounts of inhabitants, those where the population has access to drinking water supplied by the local aqueduct, those with no water treatment system and quality control of water, and the ones with large croplands and located close to Galeras volcano. Due to lack of reports on water fluoride levels, a blind evaluation of fluoride opacities was conducted. The study was approved by the Ethics Committee of Health Sciences (Act no. CECS01- 2011).
Clinical evaluation
A questionnaire that included demographic variables such as age, sex and municipality, as well as the indexes to measure fluoride opacities and enamel hypoplasia was designed for data collection. Scientific literature and color photographs of the oral cavity were previously studied by two examiners in order to diagnose dental enamel defects in these municipalities. These defects were differentiated from carious lesions by their clinical appearance and locations (active lesions in areas of plaque accumulation along the gingiva and from the gingiva to interproximal areas or occlusal fissures, not present at eruption, may affect any tooth but are commonly found in premolars and molars).24 The evaluation was performed very early in the morning. The subjects were evaluated after their dental care routine at home. Teeth were manually cleaned with cotton rolls and fluoride rinse if they were not clean enough. Teeth were isolated with cotton rolls placed on the buccal sulcus before examination. The participants were examined under natural light while sitting. The oral examination of each student was performed in the main hall of schools. Fluoride opacities were recorded according to Dean's index.25 Each individual received a score corresponding to the clinical appearance of the second tooth most severely affected in the mouth. The criteria are shown in (table 1). Enamel hypoplasia was diagnosed in dry teeth following the index by Silberman et al,22 as follows: Type I: enamel discoloration due to hypoplasia, Type II: abnormal coalescence due to hypoplasia, Type III: some parts of the enamel are missing due to hypoplasia, and Type IV: a combination of the three types of hypoplasia above. Enamel hypoplasia was diagnosed if children and adolescents had any of these types.
Inter-observer variability
For inter-examiner agreement, 60 children and adolescents (10% of 599) were evaluated once by two researchers. The agreement average between both examiners through Cohen's Kappa coefficient was 0.80.
Statistical analysis
Prevalence rate with 95% confidence intervals (95% CI) was calculated. The comparison of dental fluorosis opacities and enamel hypoplasia frequency with demographic and dental characteristics was analyzed using Chi-square test. A p value of < 0.05 was used to indicate statistical significance. Data were analyzed with the Statistical Package for Social Sciences (SPSS version 17, Chicago, IL, USA).
RESULTS
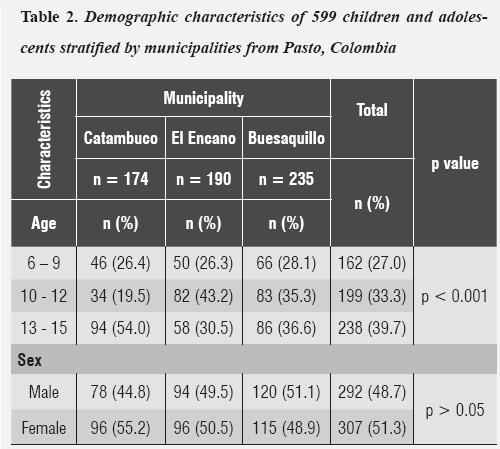
The sample included 599 students (292 males and 307 females) in the age group of 6-15 years. The mean age of children and adolescents was 11.3 years ± 2.73 individuals who were evaluated in Catambuco, El Encano, and Buesaquillo (table 2).
The prevalence of dental enamel defects in children and adolescents was 49.9% (95% CI: 45.8%-53.9%). The distribution of these defects in the municipalities of Catambuco, El Encano, and Buesaquillo was 87 (50.0 %), 95 (50.0 %) and 117 (49.7 %) respectively. Children and adolescents aged 10 to 12 (49.7%) and 13 to 15 (50.0%) showed higher frequency of dental enamel defects (p > 0.05). Fluoride opacities (FOP) were found in 255 subjects (42.6%) and enamel hypoplasia in 44 (7.3%) (table 3). Concerning FOP severity distribution, 188 out of 255 subjects (73.7%) presented a moderate level (figure 1). Prevalence of FOP in Catambuco, El Encano and Buesaquillo was 42%, 43.7% and 42.1% respectively. The highest FOP severity was found among the 13-15 age group (p < 0.001) (table 4).
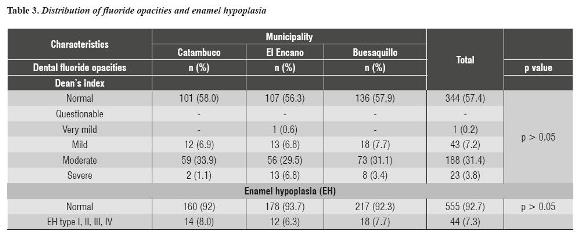
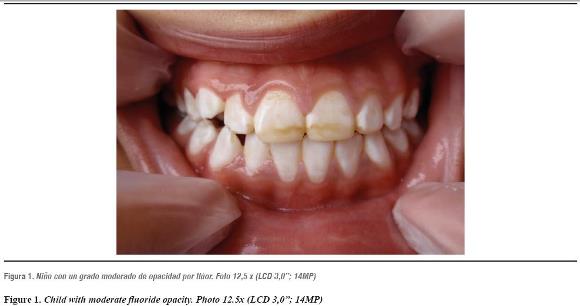
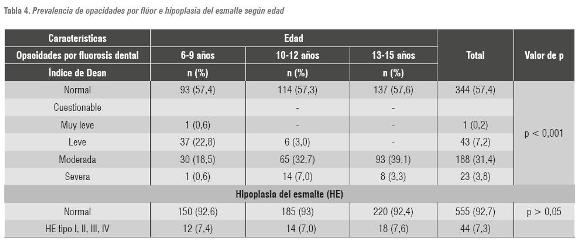
Table 5 explains the distribution of fluoride opacities and the presence of enamel hypoplasia in the total sample by sex. Out of 299 individuals with dental enamel defects, FOP were more prevalent in females, 133 (86.3%), than in males, 122 (84.2%) (p > 0.05); conversely, enamel hypoplasia was more frequent in males,23 (15.8%), than in females, 21 (13.7%).

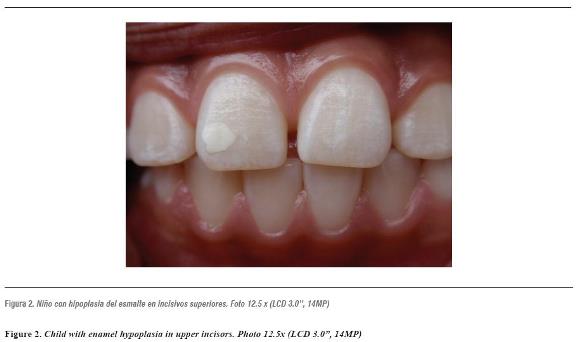
Out of the 44 children and adolescents with enamel hypoplasia, 15 (34.1%) were located in permanent upper incisors (figure 2) and canines, 8 (18.2%) in lower incisors and canines, 10 (22.7%) in upper premolars and molars and 11 (25.0%) in lower premolars and molars. Enamel hypoplasias appeared as creamy-white and brown lesions and were more frequent in permanent upper central incisors and canines.
DISCUSSION
The results of this study carried out in three municipalities of Pasto, Colombia show that prevalence rates of dental enamel defects such as fluoride opacities and enamel hypoplasia were higher and more severe than in other communities. The overall prevalence of fluoride opacities in children and adolescents was 42.6%, suggesting that fluorosis may be a public health problem in this city. We compared our results with national studies that used similar assessment methods. One of these studies was designed by Ramírez-Puerta et al,16 who found dental fluorosis in 81% of individuals from Medellín, and another one by Sánchez et al,17 who found out that regions of Caldas had 63.3% very mild and 56.3% mild dental fluorosis opacities, even this being a volcanic zone. However, in these municipalities the most frequent result was a moderate level (31.4%) according to Dean's index. Internationally, Toassi and Abegg26 reported a prevalence of 63.7% in the municipality of Santa Tereza in Rio Grande do Sul, Brazil; however, they found a moderate level of 7.7%. Rigo et al,27 reported 32.8% fluoride opacities and a moderate level of 1.9% in the city of Passo Fundo, in the same Brazilian state. Fluoride opacities were more prevalent among females (86.3%) than males (84.2%) and a higher severity was observed in older individuals (13-15 year old).
The scientific literature shows that dental fluorosis prevalence in volcanic areas ranges from 96% to 61% in the main area of Ambrym, New Zealand.28 The researchers suggest that one possible reason for this result is that fluoride accumulates in rainwater—a phenomenon that has not previously been recognized in the etiology of fluorosis—. They also mention that this is an important consideration for populations in areas of degassing volcanoes, particularly where rainwater is part of the primary potable water supply for humans or animals. Dental opacities linked to high fluoride consumption through drinking water is quite widespread in diverse nations of the world, including US, European, African, and Asian territories.29 This has become a public health problem and a disease burden for developed and underdeveloped nations. Furthermore, fluorine aerosols in eruption columns may attach to fine ash particles and travel long distances from a volcano; these thin layers of fine ash can contain toxic amounts of fluorine and accumulate on grass. The level of severity revealed in this study may also be related to the population being exposed to different fluoride sources. It be due to the consumption not only of drinking water but also vegetables and crops.30
In this sense, an interesting finding of our study is the higher prevalence of FOP among the population of El Encano (43.7%) with a severe level (6.8%) according to Dean's index. These percentages were slightly higher in the other municipalities.
El Encano is characterized by beautiful landscapes such as Laguna de la Cocha, which has been known as an ecological heritage of our community. As a potential tourist locality, it has favored a significant economic growth in the area by offering sailing and fishing activities, as well as a variety of restaurants. Even though it is located about 22 miles from the Galeras volcano, it borders on the west with the municipality of Catambuco, which is closer to this volcano. It is also likely that the inhabitants use domestic wells. It has been previously demonstrated that even within a small community, domestic wells have a wide variety of fluoride content in water. This is in part related to divergent hydro- geological conditions; the proportion of rocks with readily leachable fluoride can vary substantially within a given geographical belt.31 Unfortunately, updated records on water fluoride content are not available nor on water supply systems and not even on domestic wells. Also, more exploratory data are required to determine the sources of fluoride associated with dental fluorosis in this area to explain the slight increase in prevalence and severity.
We observed statistical differences in terms of severity. Adolescents (13-15 year-old individuals) presented more dental fluoride opacities and these were classified as moderate. The implications of fluoride opacities during this stage may also affect dental aesthetic perceptions. In our clinical evaluation we found out that adolescents thought their peers had a ''perfect smile'' if they had moderate fluorosis (extra-white appearance), and some students with severe fluorosis felt embarrassed during dental examination, especially when their peers were present. From a dental perspective, several studies have shown that milder levels of fluorosis may not be an aesthetic problem; actually, some studies have shown a preference for those levels compared with teeth with no opacities.32 For this reason, aesthetic concerns about fluoride opacities may be questionable in adolescence.33 On the other hand, other studies report conflicts between affected and non-affected students at school, problems in achieving a romantic relationship, and uncertainties concerning the professional future. Severe dental fluorosis lesions appear to be stigmatizing and have produced suffering and self-exclusion among an entire generation of adolescents and young people.34
Enamel hypoplasia was found in 7.3% of children and adolescents. A small prevalence difference was found by Mackay and Thomson,35 who reported that 5.5% of subjects had one or more hypoplastic defects in Southland, New Zealand, and Arnadóttir et al,36 who found enamel hypoplasia in 15% of dry teeth in Reykjavík, Iceland. In our study the highest prevalence was found in the municipality of Catambuco (8.0%). Enamel hypoplasia can be influenced by hereditary factors related to autosomal dominant or recessive genes or X-linked genes, where both dentitions are affected. It can also be influenced by acquired conditions including nutritional deficiencies, exanthematous diseases, congenital syphilis, hypocalcemia, inflammation or trauma during dental development, chemical substances, and idiopathic factors.37 In this regard, Ford et al,38 found out that the main risk factors for enamel hypoplasia were low socioeconomic status, respiratory infections, exposure to cigarette smoking, asthma, otitis media, urinary tract infection (UTI) and chickenpox. Considering the characteristics of our localities, risk factors such as low socioeconomic status and respiratory infections may be relevant variables. In some residences, exposures to indoor combustion occur because of the use of coal as fuel for cooking and heating. Baker et al 39 state that using coal increases the incidence of lower respiratory illness (RR = 1.45; 95% CI: 1.07–1.97).
The above data are an exploratory approach to oral health conditions related to dental fluorosis and enamel hypoplasia in three municipalities located in Pasto, Colombia. Given that our findings show higher levels of prevalence and severity of dental fluorosis than enamel hypoplasia, preventive measures to control this condition should be taken by the communities and local governments. We consider it is necessary to design an exhaustive fluoride surveillance mapping, as well as additional geochemical research of current hydric resources, vegetables, soils, and crops in order to have an accurate evaluation of dental fluorosis prevalence and fluoride sources. Fluoride opacity is a biomarker of fluoride exposure, which not only means a dental concern but also represents a toxic environment for the inhabitants. Dental fluorosis develops in an individual during the period of teeth mineralization, which takes place since early infancy. In this regard, Seraj et al,40 explained the effect of excessive fluoride on neurological development. This relation has been relevant because of the substantial role that neural health plays on the individual's quality of life. These authors concluded that average IQ scores decreased from 97.77 ± 18.91 for the normal fluoride group to 89.03 ± 12.99 for the medium fluoride group and to 88.58 ± 16.01 for the high fluoride group (p = 0.001).
The present study is one of the first reports on dental enamel defects related to fluoride opacities and enamel hypoplasia in our community. This time the research group used Dean's and Silberman's classifications since they provide an approximate diagnosis of dental fluorosis and enamel hypoplasia and are easy to apply, particularly in places lacking the appropriate conditions for dental examinations. Although Dean's index has been used for years for assessing fluorosis and its continued use is important for historical comparisons, this index has several limitations, especially concerning its inability to measure fluorosis in different tooth surfaces.
Also, the way it has been traditionally used does not allow specifying the cosmetic importance of the most severe fluorosis detected in dentition.41 In this sense, future research is necessary to analyze the criteria of the modified DED index and the TF (Thylstrup-Fejerskov) index, which can be used with reasonable reproducibility to measure enamel defects.42
CONCLUSIONS
The prevalence of dental enamel defects was high in these municipalities, especially fluoride opacities, which were moderate according to Dean's index. Further research is required to establish levels of fluoride or other chemical compounds in these communities. Our study suggests that dental fluorosis is a public health problem among school children in Catambuco, Buesaquillo, and El Encano and that it is necessary to study fluoride sources in these municipalities. Periodic clinical evaluations should be performed to monitor rates of dental fluorosis and fluoride sources in communities at risk.
CONFLICTS OF INTEREST
We declare having no conflicts of interest that may be inherent to this submission.
ACKNOWLEDGEMENTS
We thank the principals of Instituciones Educativas Municipales (IEM) located in El Encano, Buesaquillo, and Catambuco, as well as teachers, students and parents for their assistance and cooperation in carrying out this study.
REFERENCES
1. Suckling GW. Developmental defects of enamel. Historical and present-day perspectives of their pathogenesis. Adv Dent Res 1989; 3: 87-94. [ Links ]
2. FDI World Dental Federation. Commission on Oral Health, Research & Epidemiology. A review of the developmental defects of enamel index (DDE Index). Int Dent J 1992; 42(6): 411-426. [ Links ]
3. Slayton RL, Warren JJ, Kanellis MJ, Levy SM, Islam M. Prevalence of enamel hypoplasia and isolated opacities in the primary dentition. Pediatr Dent 2001; 23(1): 32-36. [ Links ]
4. Jodalli PS, Ankola AV, Hebbal M, Vikneshan M. Aesthetic perceptions regarding fluorosis by children from an area of endemic fluorosis in India. Community Dent Health 2013; 30(4): 249-253. [ Links ]
5. Robles MJ, Ruiz M, Bravo-Perez M, González E, Peñalver MA. Prevalence of enamel defects in primary and permanent teeth in a group of schoolchildren from Granada (Spain). Med Oral Patol Oral Cir Bucal 2013; 18(2): e187-e193. [ Links ]
6. Büchel K, Gerwig P, Weber C, Minnig P, Wiehl P, Schild S et al. Prevalence of enamel fluorosis in 12-year-olds in two Swiss cantons. Schweiz Monatsschr Zahnmed 2011; 121(7-8): 647-656. [ Links ]
7. Kanagaratnam S, Schluter P, Durward C, Mahood R, Mackay T. Enamel defects and dental caries in 9-year-old children living in fluoridated and non-fluoridated areas of Auckland, New Zealand. Community Dent Oral Epidemiol 2009; 37(3): 250-259. [ Links ]
8. Cochran JA, Ketley CE, Arnadóttir IB, Fernandes B, Koletsi- Kounari H, Oila AM et al. A comparison of the prevalence of fluorosis in 8-year-old children from seven European study sites using a standardized methodology. Community Dent Oral Epidemiol 2004; 32 (Suppl 1): 28-33. [ Links ]
9. Dini EL, Holt RD, Bedi R. Prevalence of caries and developmental defects of enamel in 9-10 year old children living in areas in Brazil with differing water fluoride histories. Br Dent J 2000; 188(3): 146-149. [ Links ]
10. Thylstrup A, Fejerskov O. Clinical appearance of dental fluorosis in permanent teeth in relation to histological changes. Community Dent Oral Epidemiol 1978; 6(6): 315-328. [ Links ]
11. Osuji OO, Leake JL, Chipman ML, Nikiforuk G, Locker D, Levine N. Risk factors for dental fluorosis in a fluoridated community. J Dent Res 1988; 67(12): 1488-1492. [ Links ]
12. Symonds RB, Rose WI, Reed MH. Contribution of Cl and F-bearing gases to the atmosphere by volcanoes. Nature 1988; 334: 415-418. [ Links ]
13. D'Alessandro W. Human fluorosis related to volcanic activity: a review. In: Kungolos AG, Brebbra CA, Samaras CP, Popov V. Environmental Toxicology. Ashursr: Witpress; 2006. [ Links ]
14. Dean HT. Classification of mottled enamel diagnosis. J Am Dent Assoc 1934; 21: 1421-1426. [ Links ]
15. De Lourdes Azpeitia-Valadez M, Sánchez-Hernández MA, Rodríguez-Frausto M. Risk factors for dental fluorosis in children between 6 and 15 years old. Rev Med Inst Mex Seguro Soc 2009; 47(3): 265-270. [ Links ]
16. Ramírez-Puerta BS, Franco-Cortés AM, Ochoa-Acosta EM. Dental fluorosis in 6-13-year-old children attending public schools in Medellín, Colombia. Rev Salud Pública 2009; 11(4): 631-640. [ Links ]
17. Sánchez H, Parra JH, Cardona D. Fluorosis dental en escolares del departamento de Caldas, Colombia. Biomédica 2005; 25(1): 46-54. [ Links ]
18. Crabb JJ. The restoration of hypoplastic anterior teeth using an acid-etched technique. J Dent 1975; 3(3):121-124. [ Links ]
19. William V, Messer LB, Burrow MF. Molar incisor hypomineralization: review and recommendations for clinical management. Pediatr Dent 2006; 28(3): 224-232. [ Links ]
20. Jälevik B, Norén JG. Enamel hypomineralization of permanent first molars: a morphological study and survey of possible aetiological factors. Int J Paediatr Dent 2000; 10(4): 278-289. [ Links ]
21. Do Espírito Santo Jácomo DR, Campos V. Prevalence of sequelae in the permanent anterior teeth after trauma in their predecessors: a longitudinal study of 8 years. Dent Traumatol 2009; 25(3): 300-304. [ Links ]
22. Silberman SL, Trubman A, Duncan WK, Meydrech EF. A simplified hypoplasia index. J Public Health Dent 1990; 50(4): 282-284. [ Links ]
23. Ramos-Martinez K, González-Martínez F, Luna-Ricardo L. Oral and nutritional health status in children attending a school in Cartagena, 2009. Rev Salud Pública 2010; 12(6): 950-960. [ Links ]
24. Russell AL. The differential diagnosis of fluoride and nonfluoride enamel opacities. J Public Health Dent 1961; 21: 143-146. [ Links ]
25. Dean HT. The investigation of physiological effects by epidemiological method. En: Moulton FR, editor. Fluorine and dental health. Washington, DC: American Association for the Advancement of Science; 1942. p. 23-71. [ Links ]
26. Toassi RF, Abegg C. Dental fluorosis in schoolchildren in a county in the mountainous region of Rio Grande do Sul State, Brazil. Cad Saúde Publica 2005; 21(2): 652-655. [ Links ]
27. Rigo L, Caldas Junior Ade F, Souza EA, Abegg C, Lodi L. Study on the dental fluorosis in a Southern city of Brazil. Cien Sâúde Coletiva 2010; 15(Suppl 1): 1439-1448. [ Links ]
28. Allibone R, Cronin SJ, Charley DT, Neall VE, Stewart RB, Oppenheimer C. Dental fluorosis linked to degassing of Ambrym volcano, Vanuatu: a novel exposure pathway. Environ Geochem Health 2012; 34(2): 155-170. [ Links ]
29. Aminabadi N, Taghizdeh Gangi A, Balayi E, Sadighi M. Prevalence of fluorosis in 5-12 year-old children in the North-Western Villages of Makoo in 2004. J Dent Res Dent Clin Dent Prospects 2007; 1(1): 33-41. [ Links ]
30. Saini P, Khan S, Baunthiyal M, Sharma V. Mapping of fluoride endemic area and assessment of F(-1) accumulation in soil and vegetation. Environ Monit Assess 2013; 185(2): 2001-2008. [ Links ]
31 Gopalakrishnan P, Vasan RS, Sarma PS, Nair KS, Thankappan KR. Prevalence of dental fluorosis and associated risk factors in Alappuzha district, Kerala. Natl Med J India 1999; 12(3): 99-103. [ Links ]
32. Davies GM, Pretty IA, Neville JS, Goodwin M. Investigation of the value of a photographic tool to measure self-perception of enamel opacities. BMC Oral Health 2012; 12(1): 41. [ Links ]
33. McGrady MG, Ellwood RP, Goodwin M, Boothman N, Pretty IA. Adolescents' perceptions of the aesthetic impact of dental fluorosis vs. other dental conditions in areas with and without water fluoridation. BMC Oral Health 2012; 12(1): 4. [ Links ]
34. De Castilho LS, e Ferreira EF, Perini E. Perceptions of adolescents and young people regarding endemic dental fluorosis in a rural area of Brazil: psychosocial suffering. Health Soc Care Community 2009; 17(6): 557-563. [ Links ]
35. Mackay TD, Thomson WM. Enamel defects and dental caries among Southland children. N Z Dent J 2005; 101(2):35-43. [ Links ]
36. Arnadóttir IB, Sigurjóns H, Holbrook WP. Enamel opacities in 8-year-old Icelandic children in relation to their medical history as infants. Community Dent Health 2005; 22(4): 279-281. [ Links ]
37. Ruprecht A, Batniji S, El-Neweihi E. The incidence of enamel hypoplasia in the dental office. J Can Dent Assoc 1984; 50(12): 900-902. [ Links ]
38. Ford D, Seow WK, Kazoullis S, Holcombe T, Newman B. A controlled study of risk factors for enamel hypoplasia in the permanent dentition. Pediatr Dent 2009; 31(5): 382- 388. [ Links ]
39. Baker RJ, Hertz-Picciotto I, Dostál M, Keller JA, Nozicka J, Kotesovec F et al. Coal home heating and environmental tobacco smoke in relation to lower respiratory illness in Czech children, from birth to 3 years of age. Environ Health Perspect 2006; 114(7): 1126-1132. [ Links ]
40. Seraj B, Shahrabi M, Shadfar M, Ahmadi R, Fallahzadeh M, Eslamlu HF et al. Effect of high water fluoride concentration on the intellectual development of children in Makoo/Iran. J Dent 2012; 9(3): 221-229. [ Links ]
41. Horowitz HS. Indexes for measuring dental fluorosis. J Public Health Dent 1986; 46(4): 179-183. [ Links ]
42. Khan H. Evaluation of two different indices using photographic method of assessment of enamel defects (opacities). J Postgrad Med Inst 2005; 19(2): 149-156. [ Links ]
