










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
versão impressa ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.26 no.2 Medellín jan./jun. 2015
ORIGINAL ARTICLES DERIVED FROM RESEARCH
A CEPHALOMETRIC STUDY IN CHILDREN FROM MEDELLÍN AGED 3 TO 6 YEARS WITH CLASS I DENTAL OCCLUSION11
Julia Andrea Gómez Gómez2; Elizabeth Llano Sánchez2; Claudia Patricia Londoño Urrego3; Alejandra María Rendón Ocampo3; Mónica María Gaviria Molina4
1 Article derived from a research project funded by the CODI, to qualify for
the title of Clinical Specialist in Comprehensive Dentistry for Children and
Maxillary Orthopedics, School of Dentistry, Universidad de Antioquia.
2 Specialists in Comprehensive Dentistry for Children and Maxillary
Orthopedics, Universidad de Antioquia. Part-time professor, School
of Dentistry, Universidad de Antioquia. E-mail: juliagomezg@gmail.com
3 Student of the Clinical Specialization in Comprehensive Dentistry for
Children and Maxillary Orthopedics, School of Dentistry, Universidad
de Antioquia.
4 Dentistry Student, School of Dentistry, Universidad de Antioquia.
SUBMITTED: MARCH 5/2013-ACCEPTED: MARCH 4/2014
Gómez JA, Llano E, Londoño CP, Rendón AM, Gaviria MM. A cephalometric study in children from Medellín aged 3 to 6 years with Class I dental occlusion. Rev Fac Odontol Univ Antioq 2015; 26(2):
ABSTRACT
INTRODUCTION: the few available studies that have been done with digital lateral cephalic x-rays in children younger than 6 years
makes it necessary to conduct research on this age group. The purpose of this study was to determine the average cephalometric measures in
children from the municipality of Medellín aged 3 to 6 years with class I dental occlusion, by estimating differences by age, sex, facial biotype,
weight and size.
METHODS:this was a descriptive transversal study using digital lateral cephalic radiographs in 99 children aged 3 to 6 years
who met the inclusion criteria in order to determine cephalometric averages.
RESULTS: between the ages of 3 and 4 years there is more sexual
dimorphism, with more protrusive maxilla and mandible in girls; these differences are lower at the age of 5, becoming undetectable at the age of
6. The behavior of variables by age show that longitudinal measures tend to increase with age. Dolichofacial kids showed higher values in the
anterior-posterior direction of linear measures, while leptofacial kids showed higher values in the angular measures in the vertical direction. There
were no statistically significant differences in terms of weight/height relationship with cephalometric variables.
CONCLUSIONS: the value of linear
measures rises as age increases, supporting the use of specific standards for each age. This study suggests that there is sexual dimorphism among
cephalometric variables, being more evident at the ages of 3 and 4 years. The different facial biotypes show specific cephalometric features.
Key words: cephalometry, reference values, children, cross-sectional study, growth.
INTRODUCTION
Parents or guardians are currently more aware of the possibility of early interventions in children and nowadays there is more recognition of the role of maxillary orthopedic specialists dedicated to the management of craniofacial problems, who are interested in understanding how the craniofacial complex changes during growth and try to determine how much and when significant amounts of these changes may occur, as well as the direction they take and when they are considered completed. These specialists should therefore be more prepared every day with reliable diagnostic criteria and more preventive interventions, rather than waiting for the occlusal alterations to worsen, probably making prognosis less favorable.1-5
Correcting any type of craniofacial alterations requires proper diagnosis and to this end clinicians use, in addition to their clinical judgment, diagnostic aids such lateral cephalic x-rays, since a better understanding of the development of skeletal relations can enable more accurate decisions on the time and type of orthopedic interventions, and allow to determine their prognosis, evaluate their progress, and show parents or guardians the achieved progress.5
Several authors6-18 have suggested specific cephalometric studies, assessing skeletal, dental, and soft tissue relationships in individuals with good occlusion and facial harmony, and establishing standard sizes for each characteristic, with ranges according to age, sex, facial type, race, and among other variables. This has been done because researchers have shown that the craniofacial complex is in constant change and the behavior of each structure largely depends on the child's stage of development; also, there are differences in terms of sex, and from early age growth trends and deviations from normality can be identified. This makes it necessary for each patient to be evaluated within specific cephalometric standards according to population type, age, and sex.
Most standards have been established in Caucasian populations aged 6 and above. However, some studies have been done in younger populations. For example, in 1954, Higley6 conducted a longitudinal study in the Caucasian population aged 4 to 8 years. In 1973, Bugg7 carried out a cross-sectional study on Latino children aged 4 and 5 years. Bishara,8 in 1981, made a longitudinal study in the Caucasian population of 5 to 12 years of age, obtaining cephalometric standards by sex. In 1996, Palacino and Arias9 conducted a cross-sectional study in an Envigado population with 90 children between 3 and 5 years of age, obtaining cephalometric standards by age and sex. In 1998, Bishara et al10 carried out a longitudinal study to evaluate soft tissue profile in patients between 5 and 45 years of age. In 2000, Barrera et al11 made a cross-sectional study with 1000 cephalograms of patients between 2 and 15 years of age in different regions of Colombia, in order to compare and establish differences with standards of Ann Arbor, Michigan, according to Steiner's analysis12. In 2002, Tanabe et al13 conducted a study in 122 Japanese children between 3 and 5 years of age to evaluate the relationship between cranial base and the morphological relations of the maxillofacial component. In 2004, Flores et al14 carried out a study in 47 Mexican children, and described and compared patterns of craniofacial growth by sex. In 2005, Thilander et al15 made a longitudinal study in a Swedish population between the ages of 5 and 31 years, to establish cephalometric standards and evaluate sexual dimorphism. In 2012, Moller et al17 conducted a cross-sectional study in a Caucasian population aged 3 to 6 years, establishing soft tissue standards in three-dimensional surface cephalometry.
Either these studies were made in populations different to that of Medellín18 or did not report the used measurements commonly, thus limiting the cephalometric diagnosis in our patients. In addition, the increasingly use of digital radiographs makes it necessary to have parameters that relate clinical findings of patients aged 3 to 6 years with diagnostic aids such as digital lateral cephalic x-rays, so that they can be used by health personnel as diagnosis tools and as support for early treatment.
The purpose of this study was to determine, through digital lateral cephalic x-rays, the average cranial, mandibular, maxillary, intermaxillary relations, dental, and soft tissues cephalometric measures in a population between 3 and 6 years with Class I dental occlusion living in the city of Medellín, estimating differences by age, gender, facial biotype, weight, and size.
METHODS
This was a cross-sectional descriptive study with a non-probability sample of a population of children from Medellín aged 3 to 6 years. In total, 1348 children were examined and 108 met the dental characteristics established to participate in the study. The inclusion criteria were: absence of evident interproximal caries, normal occlusion or characteristics of dental Class I occlusion (molar relationships in a flush terminal plane or a mesial step lower than 2 mm), Class I deciduous canine relationships, overjet no greater than 2 mm, overbite not exceeding 50% and without crowding, convex profile, signs of good nutrition, and absence of systemic diseases. The following patients were excluded: children with obvious facial asymmetries, interproximal caries, craniofacial syndromes, proven mouth breathing, history of craniofacial trauma and temporomandibular joint problems, as well as patients with tongue thrust, thumb-sucking, or who had undergone orthopedic, orthodontic, or surgical maxillary treatment. This research project closely followed the recommendations for biomedical research of the World Medical Association's Declaration of Helsinki in 1964, as well as the administrative and scientific-technological standards for research in health, Resolution No. 008430 of 1993 issued by the Ministry of Health. This project falls in the category of higher risk than the minimum.19
The patients' parents were informed about the study and they signed an informed written consent. A medical history form was filled for each child and each was taken a digital lateral cephalic image with standardized radiological techniques and adequate protection. Each x-ray was taken with the Frankfort plane as parallel to the floor as possible, with ear plugs in the auditory canals to prevent head movements while imaging and teeth in maximum intercuspidation. All images were obtained in the same cephalometric equipment and by the same operator to avoid differences in both radiographic magnification and technique. The obtained image was calibrated 1:1, eliminating magnification. A Bluex PantOs 16xp Ceph equipment was used; it was vertically adjusted to accommodate subjects on their feet, standardized to 67 kV, 10 mA and with an exposure time of 10 seconds and a focus-cassette distance of 165cm; the digital images were recorded on a FUJIFILM Fuji IP X-ray 20.1 x 25.2 cassette.
Of the initial sample of 108 x-rays taken, 9 were discarded due to bad image quality, leaving a total of 99 radiographs (55 girls and 44 boys). A total of 63 cephalometric variables were selected to be measured in each individual, and they were processed in the Radiocef Studio 2 software version 4.0, obtaining digital tracings.
To avoid variability between the researchers, intraand inter-operator standardization was made in the cephalometric points, evaluating 19 radiographs at two different times, with an interval of 2 weeks, making a blind evaluation of them. Intraclass correlation coefficient was used to evaluate intraoperator concordance. The standardization process was done up to three times in order to achieve concordance above 0.8, not only in terms of point stimulator, but also in the respective confidence interval.
The sample was divided by age and sex (table 1) as follows: 3 years (12 females and 9 males), 4 years (20 females and 18 males), 5 years (14 females and 12 males), and 6 years (9 females and 5 males). In addition, they were classified according to biotype by means of Bimler suborbital facial index20, 21 (56 dolichofacial, 36 mesofacial, and 7 leptofacial) (table 1) recording each patient's weight and height at the time of taking the radiograph in order to classify them according to the Z-score index.
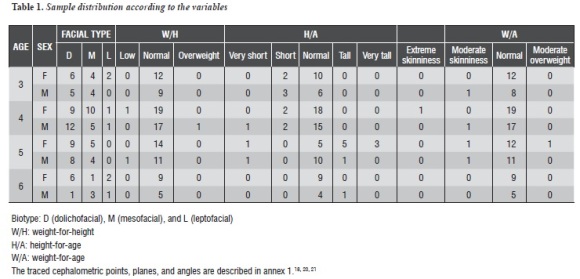
The following indicators were used: weight-forheight (W/H), height-for-age (H/A), and weightfor- age (W/A), as well as a classification system recommended by the National Center for Health Statistics (NCHS) based on Standard Deviations (SD) from the median (Z-scores).
Of the total sample (table 1) , 96 patients presented suitable weight-for-height, only 2 had low weightfor- height, and only 1 had high weight-for-height. While 77 patients presented appropriate height/age relationship, only 12 patients had very low to low height/age ratio and 10 had a high to very high relationship. In terms of weight/age ratio, 93 patients had normal weight/age ratio, 5 presented low weight-for-age, and 1 had high weight-for-age. Since most patients presented appropriate weight/ height, height/age, and weight/age relationships, the analysis only took into account the height/age ratio, which is the one that in the long term demonstrates patients' nutritional status and can affect craniofacial development and growth.22, 23
Statistical analysis
Version 17 of the SPSS software was used to conduct descriptive statistical analysis, and the quantitative variables (cephalometric variables) were summarized and described by measurements of central tendency as average, and variation as standard deviation. A confidence interval of 95% for the respective average was also included. Qualitative variables are presented in absolute or relative frequencies expressed in percentages. Tables were made to summarize the obtained information.
An initial average was obtained for each of the quantitative variables regardless of age and sex. Measure comparisons between boys and girls of different ages was performed with Student t-test, and one-way ANOVA test was used to compare linear and angular measurements by age, facial type, weight, and size. Chi-square test was used to compare facial type against sex and age and to assess the existence of weight and height differences with the linear cephalometric measurements according to age and sex. A significance level of 5% (less than 0.05 P value) was always considered for the statistical tests.
RESULTS
Table 2 shows the averages, standard deviation and confidence interval for each variable, regardless of sex and age.
Table 3 summarizes of the obtained averages according to sex by age and the significance levels yielded for linear and angular measurements. Statistically significant differences are observed between boys and girls at the age of 3 in the following measurements: midface length, N-perpendicular to A point, depth of the maxilla, posterior height of the upper maxilla, Lande's angle and upper angle of profile, effective mandibular length, length of the mandibular body, and depth of face, in which we observe a slightly higher value in girls than in boys, which suggests that, in this sample, girls have larger maxilla and mandible, and a maxillary in a protruded position. The gonial angle, mainly in its upper portion, shows a greater value in boys than in girls. The anterior and anterior-inferior height appears with an increased value in girls. There is evidence of more anterior dentoalveolar maxillary development and anterior and posterior mandibular development in girls.
At age 4, the anterior cranial length and the upper gonial angle are higher in boys than in girls. The distance from N-perpendicular to point A, Lande's angle, ANB angle and upper angle of the profile is higher in girls than in boys. At the age of 5 years, the statistically significant differences are in length of midface, face depth, position of TMJs, and anterior facial height, being higher in boys. At the age of 6 years there are no statistically significant differences between boys and girls in skeletal and dental measures; the latter results may be related to the size of the sample that was lower for these ages.
Table 4 shows the obtained average values, standard deviation, and confidence intervals by age, without discrimination by sex. Note that anterior and posterior cranial length, midface length, maxillary length, maxillary depth, the maxilla anterior and posterior height, the effective mandible length, the mandibular body 1 and 2, ramus length, face depth, the position of the TMJs, maxillary-mandibular difference, anterior and posterior facial height, anterior-inferior facial height, the distance of the second deciduous upper molar to the palatal plane, the deciduous lower central incisor to the mandibular plane, the deciduous lower second molar to the mandibular plane, the permanent upper central incisor to the palatal plane, the permanent lower central incisor to the mandibular plane, and the angles of the lower permanent central incisor to the mandibular plane and FH regularly increase as age increases, while the gonial angle, especially its upper component, decreases as age progresses. On the other hand, the upper angle of profile increases from age 4.
Table 5 shows the averages, standard deviations, and confidence intervals of the variables, estimating differences by sex. Note that the distance from point A to the perpendicular of the nasion, SNA angle, Lande's angle, upper angle of the profile, the distance of the pogonion point to Nasion perpendicular, facial angle, and articulare angle show greater values in girls, which shows once again that girls from the sample have maxilla and mandible in a more protruded position. In boys, the gonial angle, especially its upper component, and the distance of the first permanent lower molar to the mandibular plane are greater. In terms of cranial base measurements, maxillary-mandibular relationships, soft tissue, and growth pattern, there are no statistically significant differences between the sexes.
Table 6 presents the averages, standard deviations, and confidence intervals for the cephalometric variables according to facial type. Notice that anterior cranial length, midface length, length and depth of the maxilla, gonial upper angle, face depth, maxillary-mandibular difference, and Ricketts' facial axis have higher values in dolichofacial patients followed by the meso and leptofacial patients, who have the lowest values. The articulare angle, S-N/Go-ME angle, MP angle, and lower gonial angle are larger in leptofacial patients, followed by mesofacial patients. In terms of the y axis, it showed a greater value in mesofacial patients, but a comparison of leptofacials and dolichofacials showed that the latter had a lower value. It is important to highlight that very few patients in the sample belong to the lepto category, which generates a very wide confidence interval that ends up covering the patients under the meso and dolicho categories.
Analysis of the cephalometric variables by age group and sex according to the children's heightper- age did not yield statistically significant differences in terms of the craniofacial structures measured in the studied population aged 3 and 5 years, and in 6-year-old boys. At age 4, statistically significant differences appear in both girls and boys, since children with a low height-for-age have lower values in posterior cranial length, sella height, ramus length, and posterior facial height. Girls with a low height-for-age have lower values in effective mandibular length, and in mandibular bodies 1 and 2. Comparisons of 6-year-old girls were not possible since they all had normal heightfor- age; 6-year-old boys were not compared either because there was only one who was not classified as having normal nutritional status.
In general, most patients had a suitable weight for their height, and both height and weight were appropriate for their age; therefore, the craniofacial measurements were not greatly affected.
Due to the sample size, it is possible that significant differences in other structures have not been noticed, but that does not imply that they do not exist.
DISCUSSION
Currently, the majority of parameters proposed for cephalometric measurements analyzed in lateral cephalic x-rays result from longitudinal and transversal studies on populations over 6 years of age, and the studies in children of this age focus on populations different from that of Medellín or report few measurements, thus limiting the cephalometric diagnosis in these patients. Moreover, the ever more frequent use of digital lateral cephalic x-rays makes it necessary to rely on standards determined by x-rays obtained with this technology.
By comparing the values shown in table 2 with those obtained in the variables distributed by age and sex in table 3, one may observe that some measurements for 3-year-old children are not within the average values, which supports the need for differentiated parameters by age. Variables that are not within the average correspond to maxillary and mandibular longitudinal measurements, specifically maxillary length, maxillary depth, effective mandibular length and mandibular bodies 1 and 2.
Table 2 also shows that, concerning skeletal measurements, the articulare angle had the widest range of variation between the minimum and maximum values and the greatest standard deviation. This could be considered normal since this angle changes to make compensations and keep constant positional bonds between the dental arches, thus maintaining more stable relations that are also close to normal.24, 25 Similarly, concerning soft tissues, the nasolabial angle also showed a wide range of variation, agreeing with the findings by Palacino and Arias.9
When the values obtained in the different skeletal dimensions without distinguishing by sex and age were compared with the aforementioned study, whose sample consisted of children from Envigado with deciduous dentition, a similar value was found in the following variables in both studies: nasolabial angle, SNA angle, mandibular plane- SN angle, FH-mandibular angle, axis angle, gonial angle, SNB angle, ANB angle, central upper incisor to SN, and central lower incisor to mandibular plane. The study by Bishara8 reported standards for Caucasian children between 4 and 7 years without discriminating by age and sex, showing different standards in ramus length and posterior facial height—with smaller values in the present study—. The upper central incisor and the lower central incisor had a more retrusive position in the aforementioned sample. These differences are probably due to racial diversity. The differences in linear measurements may be due to magnification in the radiographic technique used in the other studies, which do not clearly specify the degree of magnification of the equipment.
In order to compare the linear measurements with the study by Palacino and Arias,9 magnification was adjusted to 11.6%, considering that lateral cephalic radiographs in the present study were taken at a distance of 16 cm from the midface to the chassis. The present study shows that the length dimensions of midface, effective mandibular length, posterior maxillary height, anterior maxillary height, anteriorinferior facial height, anterior facial height, and posterior facial height are larger. Vertical dental measurements of deciduous teeth, and Nasion perpendicular to point A and point Pog were very similar in both studies. By analyzing the posterior facial height/anterior facial height ratio, we found out that patients in the sample of Palacino and Arias9 had an average pattern of vertical growth, while in the present study patients had a neutral pattern.
By comparing the different variables by age according to sex (table 3), one can observe that greater dimorphism occurs at the age of 3, especially in terms of longitudinal measurements of maxilla and mandible, which were larger in girls. These results differ from those described by Palacino and Arias,9 who found such prevalence in boys, and from those described by Flores et al,14 who claim that there are no significant statistical differences in the cephalometric variables between the sexes.
In the present study, variables of the cranial base are not dimorphic in the ages under study. Moreover, measurements of the angles SNA, SNB, and ANB for each of the ages agree with the values obtained by Barrera et al.11 By comparing the angular measurements at the age of 6 with Riolo's standards,18 there is concordance in the following measurements: SN-FH angle, SNA angle in boys, SNB angle, SN-mandibular plane angle, gonial angle, ANB angle, and y axis angle.
The only difference was found in the SNA angle in girls, presenting a slightly increased value in the present study.
When the behavior of variables is analyzed by age (table 4), one can observe that, in general, longitudinal measurements tend to increase with age. These include effective mandibular length, which presents the highest growth, followed by length of the midface. These results are in accordance with the reports by Björk and Skiller,26 who state that growth of the mandible is greater than that of the upper maxilla in certain developmental stages.
Cranial base measurements show a longitudinal increase in cranial base, both in the anterior and posterior areas, showing statistically significant differences. This significant growth happens because the cranial base is influenced by both skeletal growth and neural growth, and this explains its higher growth rate in early stages of development as it is very dependent on the growth of the brain, which grows very fast during the three first years of life, stopping at the age of 7 or 8 years, while the cranial base continues growing due to pneumatization of the ethmoid and frontal bones.27, 28
Conversely, it was observed that the gonial angle value tends to decrease with age, in agreement with the findings by Palacino et al9 and Tanabe et al.13 This can be explained because with age the mandibular ramus acquires a more upright position, with bone apposition in the lower area of the posterior mandibular ridge rather than in the upper area, and reabsorption by adjustment occurs in the anterior edge in a downwards direction rather than upwards, producing rotation by reshaping of the ramus alignment. All these changes lead to closure of the gonial angle. 24, 25, 29, 30
Regarding dental changes, the present study showed that a greater vertical dentoalveolar development occurs at later ages, in agreement with the observations by Palacino and Arias,9 who proved greater vertical dentoalveolar development in both maxilla and mandible as age increases.
When comparing the values obtained in boys and girls regardless of age (table 5), it has been proven that girls in this sample had a more protruded position of maxilla and mandible, indicating sexual dimorphism. This behavior could be explained by the fact that women tend to grow faster than men, who later reach them and continue growing until several years later—a behavior observed during pubertal growth peak. 1, 31
When the different cephalometric variables are analyzed in relation to facial type (table 6), one can observe that the measurements with the highest statistically significant values in the dolichofacial patients were the linear measurements in an anteriorposterior direction, while the highest statistically significant values in the leptofacial patients were the angular measurements in a vertical direction. Both results confirm that leptofacial patients tend to have vertical growth, while dolichofacial patients tend to have horizontal growth. 20, 21, 32
In assessing the behavior of the different cephalometric variables according to height-for-age ratio, there are no overall statistically significant differences in the expression of growth of the different craniofacial structures evaluated, with the exception of posterior cranial length, saddle height, ramus length, and posterior facial height in 4-year-old boys, and effective mandibular length and mandibular body in 4-year-old girls—points that present lower values in children with a low height-for-age.
Since 78% of the study population had adequate height-for-age, it is possible to state that this population does not present statistically significant differences between those considered short or tall, in contrast with the study by Meneses López and Mendoza Canales,23 who evaluated 74 chronic malnourished children and 126 children with normal nutritional status, finding out marked differences between the two groups.
With the exception of a few measurements, the nutritional status does not affect the behavior of cephalometric variables; however, more specific studies are required with regard to the nutritional status of patients in order to determine the presence of significant differences in cephalometric measurements by relating height- and weight-for-age.
CONCLUSIONS
Comparisons between sexes by age show greater dimorphism between the ages of 3 and 4 in terms of maxilla and mandible dimensions. Between 5 and 6 years of age, these gender differences tend to decrease.
In general, in the studied sample, girls have larger maxilla and mandible, with a more protruded position.
The value of linear dimensions increases as age increases, validating the use of specific standards for each age.
Each facial type exhibits specific cephalometric features that indicate the underlying growth pattern.
RECOMMENDATIONS
It is suggested to conduct a longitudinal study to evaluate the behavior of the different cephalometric variables over time in children classified with normal occlusion.
In order to make linear measurement comparisons among cephalometric studies, it is necessary for future research to precisely describe the radiographic magnification provided by the equipment used.
To establish the influence of nutritional status in the behavior of craniofacial structures, it is suggested to include a larger sample of children in different nutritional scales, homogeneously distributed.
ACKNOWLEDGMENTS
To the Foundations Golondrinas and Ximena Rico Llano, and to Institución Educativa Julio Arboleda, for allowing us to select patients to participate in this study.
To the Imágenes y Especialistas radiological center, where we could take the x-rays and the cephalometric tracing.
To doctors Tomás Bernal and Orlando Martínez, for their unconditional collaboration in the development of this study.
To Dr. Luis Gonzalo Álvarez Sánchez, for his advice on the statistical part.
CONFLICTS OF INTEREST
The authors report not having any conflicts of interest.
ANNEXES
Annex 1
The cephalometric points, planes, and angles that were traced are described below:
Cephalometric points: Sella (S): Centre of the sella turcica of the sphenoid. Nasion (N): most anterior point of the frontonasal suture, located on the median sagittal plane. Articulare (Ar): intersection of the posterior edge of the ramus and the basilar process of the occipital. Porion (Po): highest point of the external auditory meatus. Orbitale (Or): lowest point on the lower edge of the orbit. Condileon (Co): most posterior-superior point of the mandibular condyle. Anterior nasal spine (ANS): most anterior point of the spinous process of the maxilla, on the lower margin of the nasal cavity. Posterior nasal spine (PNS): most anterior point of the horizontal contour of the palatal bones. Point A (A): most anterior point of the anterior concavity in the bone profile of the upper maxilla, located between the ANS and the alveolar ridge. Point B (B): most anterior point of the anterior concavity in the bone profile of the anterior border of the mandible, between the Pogonion and alveolar ridge. Pogonion (Pog): most prominent point in the most anterior part of the symphysis menti. Built Gonion (Go): intersection of tangents to mandibular body and ramus. Anatomical Gonion (Go’): Center of the posterior-inferior contour of the mandible. Menton (Mn): lowest point of the mandibular symphysis, the junction of the lower edge of the symphysis with the bottom edge of the mandibular body. Anatomical Gnation (Gn): the junction of the anterior edge with the lower edge of the chin, between the Mn and the Pog; it is the center of the anterior-inferior chin contour. Built Gnation (Gn’): intersection of the tangents of N-Pog and Go-MN. Frontosphenoidal Suture (Fs): highest point of frontosphenoidal suture. Basion (Ba): most anterior and low point of the basilar process of the occipital. Pterigo-maxillary Fossa (Pt): most posterior-superior point of the pterygomaxillary fissure contour. Mesiovestibular cusp of the first upper permanent molar (C1p). Mesiovestibular cusp of the first upper deciduous molar (C1d). Mesiovestibular cusp of the first lower permanent molar (C2p) Mesiovestibular cusp of the second lower deciduous molar (C2d). Incisal edge of the deciduous upper central incisor (UCId). Incisal edge of the permanent upper central incisor (UCIp). Apex of the deciduous upper central incisor (Ap. UCId). Apex of the permanent upper central incisor (Ap. UCIp). Incisal edge of the deciduous lower central incisor (LCId). Incisal edge of the permanent lower central incisor (LCIp). Apex of the deciduous lower central incisor (Ap. LCId). Apex of the permanent lower central incisor (Ap. LCIp). Projection of A point on the horizontal of Frankfort (A’). Tuber (T): intersection in Frankfort of the vertical passing through the center of the pterygomaxillary fissure. Upper Clivus (CLu): point in the upper third of the clivus. Lower Clivus (CLl): point in the lower third of the clivus. Temporomandibular (TM): projection of point the Capitulare on Frankfort. Capitulare (C): the condyle center.
Cephalometric planesPlanes of reference: Frankfort plane (FH) points O with Po. N-Ba plane. Tangent to the clivus (CLu-CLl).NA plane. Palatal plane (ANS with PNS). Mandibular plane (Go with Mn). N-Pog plane. Go-N plane. S-Gn plane. functional occlusal plane: line that passes through the largest number of occlusal contacts. Ba-N plane. Pt-Gn Plane. longitudinal axis of the permanent upper central incisor (axis UCIp: UCIp-Ap. UCIp). Longitudinal axis of the deciduous upper central incisor (axis UCId: UCId-Ap. UCId). Longitudinal axis of the lower permanent central incisor (axis LCI q: LCIp-Ap.LCIp.). Longitudinal axis of the lower deciduous central incisor (axis LCId: UCId-Ap.UCId).Measured in mm: anterior cranial length (S to N). Posterior cranial length (S to Ar). Saddle height: S to FH perpendicularly taken to FH. Nasion height: N to FH perpendicularly taken to FH. Length of midface (Co to point A). Point "A" to the FH perpendicular to N. maxillary length (ANS to PNS). Maxillary depth (A’ to T). Posterior height of the upper maxilla (Se to PNS). Anterior height of the upper maxilla (N to ANS). Effective mandibular length (Co-NG). Length of the mandibular body L1 (Go to Mn). Length of the mandibular body L2 (Go to Gn’). Length of the mandibular body L3 (Go’ to Pog perpendicularly projected to the mandibular plane). "Pog" point to the FH perpendicular passing through N. Ramus length (Ar to Go). Facial depth (A’ to TM). Position of the TMJs (T to TM). Anterio-inferior facial height (ANS to Mn). Anterior facial height (N to Mn). Posterior facial height (S to Go’). Vertical measurement of UCIp or LCSd to the palatal plane, perpendicular to the palatal plane. Vertical measurement of C1p or C1d to the palatal plane, perpendicular to the plane palatal. Vertical measurement of LCIp or LCId perpendicular to the mandibular plane. Vertical measurement of C2p or C2d to the mandibular plane, perpendicular to the mandibular plane.Maxillo-mandibular difference: effective length of the mandible mandibular minus length of midface.
Cephalometric angles: SN-FH. S-N-Ar. SNA angle (internal angle). Tangent to the clivus/FH, inner upper angle (Factor 5). Lande's Angle (FH with NA). Upper angle of the profile (factor 1): intersection of NA with vertical passing through A perpendicular to FH (upper angle). Palatal plane-FH. Upper basal angle (PP/tangent to the clivus, inner upper angle). SNB Angle, facial angle (FH/N-Pog, outer lower angle). Articulare Angle (S-Ar- Go). SN- mandibular plane angle (S-N-MP). (FH with MP) Mandibular plane angle. Upper gonial angle (Ar-Go-N). Lower gonial angle (N-Go-Mn). Total gonial angle (Ar-Go-Mn) total gonialo. ANB angle (N-A and NB). Angle of the convexity (n-A-Pog). Angle of the occlusal plane with FH plane (PO with FH, internal angle). Occlusal plane-mandibular plane (PO with MP, internal angle). Angle of the "Y" axis (S-Gn with FH, acute inner lower angle). Ricketts's facial axis (Ba-N with Pt-Gn, outer lower angle). Angle of the ICSp or ICSd incisor to SN, outer lower angle. Angle of the UCIp or UCId with FH, outer lower angle. Angle of the UCIp or UCId to the palatal plane, outer lower angle. Angle of the LCIp or LCId to the mandibular plane, outer upper angle. Axis of the LCIp or LCId with FH, outer lower angle. Nasolabial angle (tangent to the base of the nose and tangent to the upper lip).
Bimler suborbital facial index: It is the difference between suborbital facial height (FH-I) and face depth (A’-TM); it numerically indicates facial type and its expressiveness, classifying facial types into: Deep face (1) (dolich): height is smaller than depth and the result is negative.
Medium face (2) (meso): height is larger than depth, resulting in a value between 0 and 5.
Long face (3) (lepto): height is larger than the depth, resulting in a value greater than 5.
Anthropometric indexes: each index is recorded as a z-score (*), which describes to what extent and in which direction deviates the anthropometric measurement of an average individual of its sex, established by the WHO in the 2006 Child Growth Patterns.H/A (height-for-age) Classified as normal when the value of z ≤ 1, short height for age when the value of z ≤ - 2 and ≥ - 3, very short height-for-age when the z value is ≤ - 3, tall height for age when the value of z is ≥ 2 and ≤ 3, and very tall height for age when the value of z ≥ 3.W/A (weight for age) Classified as normal when the value of z ≤ 1, low weight for age when the value of z is ≤ - 2 ≥ - 3, very low weight for age when the z value is ≤ - 3, high weight for age when the value of z is ≥ 2 and ≤ 3, very high weight for age when the value of z ≥ 3.W/H (weight for height) Classified as normal when the value of z ≤ 1, low weight for height when the value of z ≤ - 2 ≥ - 3, very low weight for height when the z value is ≤ - 3, high weight for height when the value of z is ≥ 2 and ≤ 3, very high weight for height when the value of z ≥ 3.
*Z score is measured by standard deviations.
REFERENCES
1. Ferrario VF, Sforza C, Poggio CE, Schmitz JH. Facial Volume changes during normal human growth and development. Anat Rec 1998; 250(4): 480-487. [ Links ]
2.Tausche E, Luck O, Harzer W. Prevalence of malocclusions in the early mixed dentition and orthodontic treatment need. Eur J Orthod 2004; 26(3): 237-244. [ Links ]
3. Schopf P. Indication for and frequency of early orthodontic therapy or interceptive measures. J Orofac Orthop 2003; 64(3): 186-200. [ Links ]
4. Pedersen T, Norholt SE. Early orthopedic treatment and mandibular growth of children with temporomandibular joint abnormalities. Semin Orthod 2011; 17(3): 235-245. [ Links ]
5. Buschang PH, Martins J. Childhood and adolescent changes of skeletal relationships. Angle Orthod 1998; 68(3):199-208. [ Links ]
6. Higley LB, Hill Ch. Cephalometric standards for children 4 to 8 years of age. Am J Orthod 1954; 40(1): 51-59. [ Links ]
7. Bugg JL Jr, Canavati PS, Jenning RE. A cephalometric study for preschool children. J Dent Child 1973; 40(2): 103-104. [ Links ]
8. Bishara SE. Longitudinal cephalometric standards from 5 years of age to adulthood. Am J Orthod 1981; 79(1): 35- 44. [ Links ]
9. Palacino DC y Arias MI. Estudio cefalométrico en niños con dentición decidua entre los 3 y los 5 años de edad del municipio de Envigado [Tesis de Postgrado]. Medellín: Universidad CES; 1996. [ Links ]
10. BBishara SE, Jakobsen JR, Hession TJ, Treder JE. Soft tissue profile changes from 5 to 45 years of age. Am J Orthod Dentofacial Orthop 1998; 114(6): 698-706. [ Links ]
11. Barrera MN, Bermúdez TA, Ferrucho MS, Salgado MM, Suárez A, Castro W. Determinación de las medidas del cefalograma de Steiner en un grupo de niños Colombianos. Revista de la Federación Odontológica Colombiana 2000; 98: 74-88. [ Links ]
12. Steiner C. The use of cephalometrics as aid to planning and assessing orthodontic treatment report of a case. Am J Orthod 1960; 46(10): 721-735. [ Links ]
13. Tanabe Y, Taguchi Y, Noda T. Relationship between cranial base structure and maxillofacial components in children aged 3-5 years. Eur J Orthod 2002; 24(2): 175-181. [ Links ]
14. Flores L, Fernández MA, Heredia E. Valores cefalométricos craneofaciales en niños preescolares del Jardín de Niños CENDI UNAM. Rev Odont Mex 2004; 8(1-2): 17-23. [ Links ]
15.Thilander B, Persson M, Adolfsson U. Roentgencephalometric standards for a Swedish population. A longitudinal study between the ages of 5 and 31 years. Eur J Orthod 2005; 27(4): 370-389. [ Links ]
16. Hönn M, Göz G. Reference values for craniofacial structures in children 4 to 6 years old: review of the literature. J Orofac Orthop 2007; 68: 170-182. [ Links ]
17. Möller M, Schaupp E, Massumi-Möller N, Zeyher C, Godt A, Berneburg M. Reference values for three-dimensional surface cephalometry in children aged 3-6 years. Orthod Craniofac Res 2012; 15: 103-116. [ Links ]
18. Riolo ML. An atlas of craniofacial growth: cephalometric standards from the university school growth study, the University of Michigan. Michigan: Craniofacial growth series. Center for Human Growth and Development, University of Michigan; 1974. [ Links ]
19. Colombia. Ministerio de Salud. Resolución N.° 008430 de 1993 por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. Bogotá: El Ministerio; 1993 [ Links ]
20. Simões WA. Ortopedia funcional de los maxilares a través de la rehabilitación neuro-oclusal. 3.a ed. Sâo Paulo: Artes Médicas; 2003. [ Links ]
21. Bimler HP. Los modeladores elásticos y análisis cefalométrico compacto. Caracas: Amolca; 1993. [ Links ]
22.WHO. Experts Committe. Physical status: The use and interpretation of anthropometry. [Internet]. [Consultado 2012 May 9]. Disponible en: http://www.who.int/.../ physical_status/en/index [ Links ]
23. Meneses López A, Mendoza Canales FV. Características cefalométricas de niños con desnutrición crónica comparados con niños en estado nutricional normal de 8 a 12 años de edad. Rev Estomatol Herediana 2007; 17(2): 63-69. [ Links ]
24. Enlow DH, Poston WR. Crecimiento maxilofacial. 3.ª ed. México: Interamericana McGraw Hill; 1992. [ Links ]
25. Enlow DH, Moyers R. Growth and architecture of the face. J Am Dent Assoc 1971; 82(4): 763-774. [ Links ]
26.Björk A, Skieller V. Postnatal growth and development of the maxillary complex. En: McNamara JA, editor. Factors affecting the growth of the midface. Ann Arbor: University of Michigan; 1976. [ Links ]
27. WFord EHR. Growth of the human cranial base. Am J Orthod 1958; 44(7): 498-506. [ Links ]
28. Björk A. Cranial base development. Am J Orthod 1955; 41(3): 198-225. [ Links ]
29. Enlow DH, Harris DB. A study of the postnatal growth of the human mandible. Am J Orthod 1964; 50(1): 25-50. [ Links ]
30.Liu YP, Behrents RG, Buschang PH. Mandibular growth, remodeling, and maturation during infancy and early childhood. Angle Orthod 2010; 80: 97-105. [ Links ]
31. Proffit WR, Fields HW. Ortodoncia contemporánea. Teoría y Práctica. 4.a ed. Barcelona: Elsevier; 2007. [ Links ]
32.FF. Schudy. Vertical growth versus anteroposterior growth as related to function and treatment. Angle Orthod 1964; 34(2): 75-93. [ Links ]
