










Services on Demand
Journal
Article
 text in
text in  Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
Print version ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.26 no.2 Medellín Jan./June 2015
ORIGINAL ARTICLES DERIVED FROM RESEARCH
GUIDELINES FOR CLINICAL DIAGNOSIS OF PULP AND PERIAPICAL PATHOLOGIES. ADAPTED AND UPDATED FROM THE "CONSENSUS CONFERENCE RECOMMENDED DIAGNOSTIC TERMINOLOGY" PUBLISHED BY THE AMERICAN ASSOCIATION OF ENDODONTISTS (2009)
Talía Y. Marroquín Peñaloza1; Claudia C. García Guerrero2
1 DDM, Endodontics Specialist, Universidad Nacional de Colombia
2 DDM, Endodontics Specialist, Pontificia Universidad Javeriana.
Assistant Professor, Universidad Nacional de Colombia. E-mail: ccgarciag@unal.edu.co
SUBMITTED: APRIL 9/2013-ACCEPTED: NOVEMBER 10/2013
Marroquín TY, García CC. Guidelines for clinical diagnosis of pulp and periapical pathologies. Adapted and updated from the "Consensus Conference Recommended Diagnostic Terminology" published by the American Association of Endodontists (2009). Rev Fac Odontol Univ Antioq 2015; 26(2): 398-424.
ABSTRACT.
INTRODUCTION: accurate diagnosis in endodontics leads to the selection of adequate endodontic treatment. The terms used to name
each pathology must be associated to particular clinical conditions. The standardization of diagnostic terminology in endodontics has been
widely discussed in the academic and clinical fields. The objective of this study was to adapt and update the Guidelines for clinical diagnosis of
pulp and periapical pathologies under the parameters of the ADAPTE methodology for circulation and socialization within the academic and
professional communities.
METHODS: guidelines search was conducted in compiling agencies such as the National Guideline Clearinghouse (NGC),
USA National Center of Guidelines, and the Agency for Healthcare Research and Quality (AHRQ). Guidelines were selected with the AGREE II
tool, considering AAE's document "Consensus Conference Recommended Diagnostic Terminology" (2009) as "recommendable", and initiating
the adaptation process with ADAPTE. The source databases include Cochrane, PubMed, Tripdatabase, with verifiable key words in DeCS and
MeSH. Literature assessment followed the parameters of the Scottish Intercollegiate Guidelines Network (SIGN) and the method of the National
Institute for Clinical Excellence (NICE).
RESULTS: adaptation and update of the Guidelines for clinical diagnosis of pulp and periapical disease.
CONCLUSIONS: terminology standardization will allow identifying pulp tissue and periapical conditions. The development of guidelines for clinical
practice must be supported on scientific evidence and on agreed methodologies.
Key words: dental pulp diseases, diagnosis, sensitivity and specificity, x-rays, periapical diseases, guidelines for clinical practice as search terms.
INTRODUCTION
Endodontics is a clinical discipline that involves the development of specialized academic activities in microbiology, oral biology, pathology, epidemiology, radiology, and biomaterials, which assist in the diagnosis, prevention, and treatment of pulp and periapical pathologies.1 Endodontic diagnosis is defined as the process of identifying pulp and periapical conditions, comparing the signs and symptoms of each disease.2 However, the terminology of endodontic diagnostic has been a topic of discussion, controversy, and debate for decades.3
The Guidelines for Good Clinical Practice (GCP) and the Guidelines for Clinical Diagnosis (GCD) are recognized as "systematically developed recommendations to help professionals and patients make decisions on appropriate health care, by choosing the adequate diagnostic or therapeutic options in dealing with a health problem or a specific clinical condition".4
Since 1990, with the rise of evidence-based medicine, the development of GCP has been implemented to support professional performance in the field of health.5, 6
In Colombia, the Ministry of Health, now Ministry of Social Protection, under Resolution 412 of the year 20007 in accordance with the Agreement 117 of the National Social Security Council, states that "all the activities, procedures, and interventions of induced mandate and enforced observance shall design or adopt technical standards and guidelines of care in order to develop specific protection and early detection actions, along with attention to diseases of interest in public health care."7
The same section continues with Chapter I, Article 4, which determines:
Healthcare Guidelines is the document that establishes the activities, procedures, and interventions to be followed in a sequential and logical order for the diagnosis and treatment of diseases of public health interest, established in Agreement 117 of the National Council of Social Security in Health as liability of Health Promoting Entities, Adapted Entities, and Administrators of the Subsidized Regime.8
By 2008, program managers of the Workshop of the American Association of Endodontists (AAE)9 held the first consensus conference for standardization of diagnostic terminology in endodontics, gathering authorities and experts with the ability to evaluate the best evidence available in this regard.9 Aware of this backgrounds, the Endodontics Graduate Program of Universidad Nacional de Colombia School of Dentistry (FOUN for its Spanish initials) proposed to adapt and update the Guidelines for Clinical Diagnosis of Pulp and Periapical Diseases under the parameters of the ADAPTE methodology.10 This guidelines are intended for the dental profession in general and particularly for clinicians and providers of endodontic services.
METHODS
Initial phase
Topic selection and prioritization of the subject
Confusion in diagnostic definitions increases when clinicians, educators, and researchers use a variety of terms in their teaching and clinical practice to define endodontics diagnosis.9, 11 The FOUN Endodontics Graduate Program identified the need to unify the criteria for pulp and periapical disease diagnosis in endodontics (figure 1).
Formulation of clinical questions for the development of GCD
The objective of this phase was to design clinical questions to develop the topic approached by GCD4, 10, 12 (figure 1).
The PICO (patients-intervention-comparisonoutcome) and PIPOH (patient or problemintervention- professionals-outcome-health as context) methods made it possible to formulate wellstructured clinical questions to guide the literature search and the elaboration of recommendations for each endodontic diagnostic.
Adaptation phase
Recognition and application of search engines for diagnostic guidelines
The possibility of consulting other high-quality GCP as secondary sources of scientific evidence can prevent the unnecessary duplication of efforts, especially in the stages of search and evaluation of scientific evidence.10, 13
GCD search included compiling agencies such as:
The National Guideline Clearinghouse (NGC),14 and the Agency for Healthcare Research and Quality (AHRQ).15 The Trip Database was also included.16
Evaluation of the consulted guidelines
The AGREE II assessment instrument (Appraisal of Guidelines for Research and Evaluation II)17 is known as the most effective tool in the evaluation and validation of the contents of diagnostic and clinical practice guidelines.18
Inclusion criteria
- Guidelines prepared as part of team activity, based on evidence, with specific, clear recommendations preferably developed by renowned agencies.
GCP with good quality standards achieving ratings over 60% in each area of the instrument (AGREE II),17 particularly in the section "Rigor of Development".
Guidelines developed or updated in the past three years.
Guidelines developed for implementation in a similar local context, in terms of patients and professionals to whom the guidelines are intended.
Exclusion criteria
- Documents unavailable in Spanish or English.
- Documents whose full version cannot be retrieved.
Documents which constitute narrative reviews of the literature produced by one or more authors; prevalence, observational or experimental studies.
Guideline selection
Two evaluators (TM), (GC) applied the AGREE II instrument17 to the selected documents,2, 11 classifying the AAE's document "Consensus Conference Recommended Diagnostic Terminology" (2009)2 as "recommendable" and continuing with the adaptation phase12, 18, 19 (figure 1).
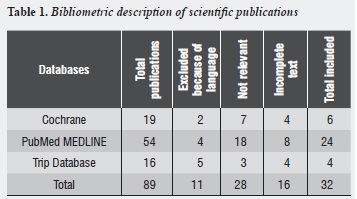
Bibliometric description
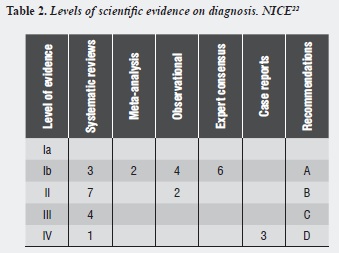
The process of literature assessment followed the parameters of the Scottish Intercollegiate Guidelines Network (SIGN),18-21 The strength for recommendation of each study was assessed using the method of National Collaborating Centres and Guideline Developers (NICE),22 which are appropriate for the assessment of diagnostic studies.
As a result, the search yielded a total of 89 items associated to endodontic diagnostic terminology and the applied tests, 32 of which (table 1) were subjected to assessment according to the NICE degree of evidence.22 All the information was finally arranged in templates designed for the evaluation (table 2). Besides the scientific publications, we included relevant archives according to the methodology as well as the official pages for each instrument applied to the entire development of the Guidelines for clinical diagnosis of pulp and periapical diseases (table 3).
DISCUSSION
The need to standardize endodontic diagnostic terminology led to the development of this adaptation/update document of the Guidelines for Clinical Diagnosis of Pulp and Periapical Diseases as a version of the "Consensus Conference Recommended Diagnostic Terminology" published by the AEE (2009). The present document used the ADAPTE methodology10 as the appropriate instrument for the adaptation process.
The development of a standardized endodontic diagnostic terminology will facilitate communication among scholars, practitioners, and patients,24 favoring accurate decision-making in relation to individual treatment of each pathology.35, 53
Quantification of pulp response to stimuli or diagnostic tests will allow the detection of tissue status. The authors use the term "accuracy" to refer to the amount or frequency in which an applied test correctly classifies a patient.26 The "accuracy" of each test needs to be demonstrated in clinical studies in correlation with Gold Standard tests. Terms such sensitivity, specificity, and predictive values must be closely associated with the clinical interpretation of individual diagnosis.54 Extensive revisions and meta-analysis show that current sensitivity tests are subjectively interpreted by both patients and operators, limiting the accuracy of predictive values to assess tests.26
The detection of periapical pathologies of endodontic origin through diagnostic imaging requires some degree of sensitivity in relation to the lesion's extent and its location within the oral cavity.54 Two-dimensional images are recognized as tests with high specificity for normal periapical tissue in 100%; however, in the detection of radiolucent lesions the sensitivity of the test may be close to 80%.55
3-D cone-beam tomography diagnostic imaging has been introduced in endodontics as a non-invasive tool to diagnose periapical pathologies, known as being 100% sensitive56 and considered as the Gold Standard Imaging Test due to its high definition and accuracy.57
The development of clinical studies that quantitatively evaluate the application of diagnostic tests becomes increasingly necessary.
CONCLUSIONS
The development of Guidelines for Clinical Diagnosis in Endodontics is an invitation to professionals and scholars to recognize the available methodology for the process of construction or adaptation of GCP based on the contribution of expert consensus, and consolidated through the analysis of clinical evidence mainly, in order to define recommendations as accurate as possible.
ACKNOWLEDGMENTS
The authors thank the group of professors of the FOUN Graduate Program in Endodontics for their recommendations from academia and their perspective as experts in the field.
Similarly, we thank Asociación de Endodoncia de Bogotá for allowing the presentation and socialization of this work.
CONFLICTS OF INTEREST
None of the authors has declared conflicts of interest.
REFERENCES
1. European Society of Endodontology. Accreditation of postgraduate specialty training programmes in endodontology. Minimum criteria for training specialists in endodontology within Europe. Int Endod J 2010; 43: 725-737. [ Links ]
2. Newton CW, Hoen MM, Goodis HE, Johnson BR, McClanahan SB. Identify and determine the metrics, hierarchy, and predictive value of all the parameters and/or methods used during endodontic diagnosis. J Endod 2009; 35(12): 1635-1644. [ Links ]
3. Sigurdsson A. Pulpal diagnosis. Endodontic Topics 2003; 5(1): 12-25. [ Links ]
4. Grupo de trabajo sobre GPC. Elaboración de guías de práctica clínica en el Sistema Nacional de Salud. Manual metodológico. Madrid: Plan Nacional para el SNS del MSC. Instituto Aragonés de Ciencias de la Salud-I+CS; 2007. [ Links ]
5. Marzo Castillejo M, Viana-Zulaica C. Calidad de la evidencia y grados de recomendación. Revista Guías Práctica Clínica [internet] 2007; 1(6) Supl: 1-14 [consultado 2012 Nov 15]. Disponible en: http://www. fisterra.com/guias2/fmc/sintesis.pdf [ Links ]
6. Oliveros HR. Niveles de evidencia y grados de recomendación en la elaboración de guías de práctica clínica. En: Manual de investigación biomédica clínica. Bogotá: Nomos, Orden Hospitalaria San Juan de Dios, Hospital Universitario Clínica San Rafael; 2009. p. 111- 118. [ Links ]
7. Colombia. Ministerio de Salud. Capítulo I Artículo 4o. Guía de atención. En: resolución número 00412 DE 2000 Febrero 25. Santa Fe de Bogotá: El Ministerio; 2000. [ Links ]
8. Colombia. Ministerio de la Protección Social, Programa de Apoyo a la Reforma de Salud/PARS. Norma técnica para la protección específica de la caries y la enfermedad gingival. En: Guías de promoción de la salud y prevención de enfermedades en la salud pública, Programa de Apoyo a la Reforma de Salud. Guía 7: 385-413. [Internet] Bogotá: Scripto; 2007. [Consultado 2013 Ene 18]. Disponible en: http:// www.nacer.udea.edu.co/pdf/libros/guiamps/ guias07.pdf [ Links ]
9. Glickman GN, Bakland LK, Fouad AF, Hargreaves KM, Schwartz SA. Diagnostic terminology: report of an online survey. J Endod 2009; 32(12): 1625-1633. [ Links ]
10. ADAPTE. Guideline adaptation: a resource toolkit. [Internet]; 2010 [Consultado 2013 Jul 12]. Disponible en: http://www.g-i-n.net/document-store/working-groupsdocuments/ adaptation/adapte-resource-toolkit-guidelineadaptation- 2-0.pdf [ Links ]
11. Colombia. Bogotá. Secretaria Distrital de Salud. Guía de práctica clínica en salud oral. patología pulpar y periapical. [Internet]. Bogotá: La Secretaría; 2009 [Consultado 2010 Mar 17] Disponible en: http://acfo.edu.co/educacion/pdf/ Guias/guia_enf_pulpar_y_periapical.pdf [ Links ]
12. Paik S, Sechrist C, Torabinejad M. Levels of evidence for the outcome of endodontic Retreatment. J Endod 2004; 30(11): 745-750. [ Links ]
13. De Gutiérrez I, González C. ¿Cómo localizar GPC? [Internet]. [Consultado 2012 Feb 10]. Disponible en: http://www.fisterra.com/bd/upload/localizar.pdf [ Links ]
14. National Guideline Clearinghouse. Health partners dental group guideline for diagnosing and treating endodontic emergencies [Internet]. [Consultado 2011 Oct 7]. Disponible en: http://www.guideline.gov/faq.aspx [ Links ]
15. Health Information and Quality Authority. Draft national quality assurance criteria for clinical guidelines. [Internet]. [Consultado 2010 Nov 3]. Disponible en: http://www.hiqa. ie/press-release/2011-10-26-national-quality-assurancecriteria- clinical-guidelines [ Links ]
16. Trip Database [Internet]. [Consultado 2012 Feb 8]. Disponible en: http://www.tripdatabase.com/search?categoryid=& criteria=++DIAGNOSIS+ENDODONTICS+
17. Consorcio AGREE. Instrumento para la evaluación de guías de práctica clínica. [Internet]. [Consultado 2011 Feb 8]. Disponible en: http://www.guiasalud.es/contenidos/ documentos/Guias_Practica_Clinica/Spanish-AGREE-II. pdf [ Links ]
18. Universidad Nacional de Colombia, Instituto de Investigaciones Clínicas, Facultad de Medicina, Grupo de Evaluación de Tecnologías y Políticas en Salud (UN GETS). Manual metodológico para la elaboración y adaptación de guías de práctica clínica, basados en la evidencia. Capítulo 2. Adaptación de guías de práctica clínica. [Internet]. [Consultado 2011 Feb 12]. Disponible en http://www.gets.unal.edu.co/cap2.pdf [ Links ]
19. Grupo de Expertos, Comité de Vacunación del Adulto Asociación Colombiana de Infectología. Guía de práctica clínica para la vacunación del adolescente y del adulto en Colombia 2012. Infectio 2012; 16(S2): 5-55. [ Links ]
20. Guyatt GH, Oxman AD, Vist GE, Kunz R, Ytter YF, Coello PA et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. [Internet]. [Consultado 2010 Oct 5]. Disponible en: http:// www.gradeworkinggroup.org/publications/GRADE-1_ BMJ2008.pdf [ Links ]
21. Scottish Intercollegiate Guidelines Network. A Guideline developer's handbook. [internet] Edimburgo: SIGN; 2001 [Consultado 2010 Oct 2] Disponible en: http://www.show. scot.nhs.uk/sign/guidelines/fulltext/50/index.html [ Links ]
22. National Institute for Clinical Excellence (NICE). Guidelines development methods. Information for National Collaborating Centres and Guideline Developers. [Internet]. [Consultado 2010 Oct 5]. Disponible en: http://www.nice.org.uk/niceMedia/pdf/GDM_ Allchapters_0305.pdf [ Links ]
23. Marroquín T, García C. Diagnósticos en endodoncia adaptación y actualización. Facultad de Odontología Universidad Nacional de Colombia. [ I n t e r n e t ] . [Consultado 2010 Oct 5]. Disponible en: http://www. odontologia.unal.edu.co/posgrados/pos_endodoncia.php [ Links ]
24. Levin LG, Law AS, Holland GR, Abbott PV, Roda RS. Identify and define all diagnostic terms for pulpal health and disease states. J Endod 2009; 35(12):1645-1657. [ Links ]
25. Marroquín T, García C. Guías de diagnóstico clínico en endodoncia adaptación para la facultad de odontología de la Universidad Nacional de Colombia. [Tesis para optar al título de especialista en Endodoncia] Bogotá: Universidad Nacional de Colombia, Facultad de Odontología; 2012. [ Links ]
26. Levin LG. Pulp and periradicular testing. J Endod 2013; 39(3S): S13-S19. [ Links ]
27. Huumonen S, Ørstavik D. Radiological aspects of apical periodontitis. Endodontic Topics 2002; 1: 3-25. [ Links ]
28. Colombia. Bogotá. Secretaría Distrital de Salud. Dirección de Planeación y Sistemas Análisis, Programación y Evaluación, Grupo de Información Lineamiento para diligenciamiento de Rips en odontología. [Internet] [Consultado 2013 Feb 18]. Disponible en: http://www.saludcapital.gov.co/Publicaciones/ Informaci%C3%B3n%20de%20prestaci%C3%B3n%20 d e % 2 0 s e r v i c i o s % 2 0 ( R I P S ) / M e m o r i a s % 2 0 Capacitaciones/RIPS%20Independientes%2016%20 mayo%202012/Lineamiento_codificaci%C3%B3nRIPS_ Salud_Oral.pdf [ Links ]
29. World Health Organization. Application of the international classification of diseases to dentistry and stomatology. 3.a ed. Geneva: WHO; 1995. [ Links ]
30. Gopikrishna V,Tinagupta K, Kandaswamy D. Comparison of electrical, thermal, and pulse oximetry methods for assessing pulp vitality in recently traumatized teeth. J Endod 2007; 33(5): 531-535. [ Links ]
31. Petersson K, Söderström C, Kiani-Anaraki M, Lévy G. Evaluation of the ability of thermal and electrical tests to register pulp vitality. Endod Dent Traumatol 1999; 15(3): 127-131. [ Links ]
32. Jafarzadeh H, Abbott PV. Review of pulp sensibility tests. Part I: general information and thermal tests. Int Endod J 2010; 43: 738-762. [ Links ]
33. Gutmann JL, Lovdahl PE. Problem solving in prevention, identification endodontics, and Management, 5.a ed. Maryland Heights: Elsevier Mosby; 2011. [ Links ]
34. Pitt Ford TR, Patel S. Technical equipment for assessment of dental pulp status. Endodontic Topics 2004; 7: 2-13. [ Links ]
35. Mejàre IA, Axelsson S, Davidson T, Frisk F, Hakeberg M, Kvist T et al. Diagnosis of the condition of the dental pulp: a systematic review. Int Endod J 2012; 45: 597-613. [ Links ]
36. Iqbal M, Kim S, Yoon F. An investigation into differential diagnosis of pulp and periapical pain: a penn endo database study. J Endod 2007; 33(5): 548-551. [ Links ]
37. Cisneros-Cabello R, Segura-Egea JJ. Relationship of patient complaints and signs to histopathologic diagnosis of pulpal condition. Aust Endod J 2005; 31(1): 24-27. [ Links ]
38. Abbott PV, Yu C. A clinical classification of the status of the pulp and the root canal system. Aust Den J 2007; 52(1 Suppl): S17-S31. [ Links ]
39. Gopikrishna V, Pradeep G, Venkateshbabu N. Assessment of pulp vitality: a review. Int J Paediatr Dent 2009; 19: 3-15. [ Links ]
40. Lin J, Chandler NP. Electric pulp testing: a review. Int Endod J 2008; 41: 365-374. [ Links ]
41. Patel S, Ricucci D, Durak C, Tay F. Internal root resorption: a review. J Endod 2010; 36(7): 1107-1121. [ Links ]
42. Pecora EC, Saquy MD, Souza M. Clinical aspects of pulpal-periodontal lesions. Aust Endod J 2002; 26: 82-85. [ Links ]
43. Estrela C, Guedes OA, Silva JA, Leles CR, Estrela CR, Pécora JD. Diagnostic and clinical factors associated with pulpal and periapical pain. Braz Dent J 2011; 22(4): 306- 311. [ Links ]
44. Seltzer S. Classification of pulpal pathosis. Oral Surg Oral Med Oral Pathol 1972; 34(2): 269-287. [ Links ]
45. McCabel PS, Dummer PM. Pulp canal obliteration: an endodontic pulp canal obliteration: an endodontic diagnosis and treatment challenge. Int Endod J 2012; 45: 177-197. [ Links ]
46. Jacobsen I, Kerekes K. Long-term prognosis of traumatized permanent anterior teeth showing calcifying processes in the pulp cavity. Scand J Dent Res 1977; 85(7):588-598. [ Links ]
47. Jafarzadeh H, Udoye CI, Kinoshita J. The application of tooth temperature measurement in endodontic diagnosis: a review. J Endod 2008; 34(12): 1435-1440. [ Links ]
48. Gutmann JL, Baumgartner JC, Gluskin AH, Hartwell GR, Walton RE. Identify and define all diagnostic terms for periapical/periradicular health and disease states. J Endod 2009; 35(12): 1658-1674 l. [ Links ]
49. Abbott PV. Classification, diagnosis and clinical manifestations of apical periodontitis. Endodontic Topics 2004; 8: 36-54. [ Links ]
50. Ricucci D, Bergenholtz G. Histologic features of apical periodontitis in human biopsies. Endodontic Topics 2004; 8: 68-87. [ Links ]
51. Sutherland S, Matthews DC, Basrani B. Emergency management of acute apical periodontitis in the permanent dentition: a systematic review of the literature. J Can Dent Assoc 2003; 69(3): 660-660l. [ Links ]
52. Petersson A, Axelsson S, Davidson T, Frisk F, Hakeberg M, Kvist T et al. Radiological diagnosis of periapical bone tissue lesions in endodontics: a systematic review. Int Endod J 2012; 45: 783-801. [ Links ]
53. Agarwal P, Agarwal A. Pulp - dead or alive? Indian J Dent Adv 2011; 3(4): 684-686. [ Links ]
54. Rushton VE, Qualtrough AJ, Al-Masserah Y, Rushton MN. The influence of coronal tooth tissue in the diagnosis of apical pathosis. Int Endod J 2009; 42: 603-608. [ Links ]
55. De Paula-Silva FW, Wu MK, Leonardo MR, da Silva LA, Wesselink PR. Accuracy of periapical radiography and cone-beam computed tomography scans in diagnosing apical periodontitis using histopathological findings as a gold standard. J Endod 2009; 35(7): 1009-1012. [ Links ]
56. Tyndall DA, Kohltfarber H. Application of cone beam volumetric tomography in endodontics. Aust Dent J 2012; 57 Suppl 1: 72-81. [ Links ]
57. Tsai P, Torabinejad M, Rice D, Azevedo B. Accuracy of cone-beam computed tomography and periapical radiography in detecting small periapical lesions. J Endod 2012; 38(7): 965-970. [ Links ]
