











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
The use of light-cured resin-based composite (RBC) restorations has recently become popular, including their use on teeth in the posterior region, due to their suitable mechanical behavior and their attractive aesthetic features.1) However, restoring a cavity preparation is a complex task and must be carried out using an incremental technique.2) This technique is used for two major reasons: first, because these materials have limited curing depth, preventing total polymerization of greater increments, and secondly because clinicians seek to control the material′s shrinking effects due to polymerization reactions.3)(4)(5)(6)(7) This is why researchers and clinicians alike have agreed on the need of applying this product in increments of up to 2 mm.2) Therefore, in the case of deep or extensive preparations, several layers of the material must be applied, resulting in a highly-complex timeconsuming work for the clinician, and involving certain risks such as the formation of air bubbles or contamination in between layers.8)(9
In response to these difficulties, a new generation of RBCs has been introduced, known as "Bulk-Fill RBCs".10) This term has been used by manufacturers to refer to RBCs which could be used in 4- or 5-mm thick increments using a monoblock or single-layer technique. However, there is much debate as to whether it is possible to apply this type of resin with increments of twice the thickness indicated for conventional RBCs, maintaining the same physical, mechanical, and biological properties of conventional RBCs.6)(11)(12)(13
In light of the recent efforts of manufacturers to promote the use of bulk-fill RBCs, it is important to analyze the recent changes in the technology of these products that have led to their advertising and to check if their performance in clinical situations is comparable to the results obtained by conventional RBCs used with the incremental technique.
Therefore, the objective of this review is to provide information on the state of the art of bulk-fill RBCs based on high-impact studies published globally. The methodology for this review consists on searching the Medline/Pubmed and SciELO databases, between January 2000 and May 2014, using these key words: "Bulk Fill", "Bulk Fill Resin", "Bulk Fill Composite(s)", "Bulk Fill Dental", and "Bulk technique".
Classification of bulk-fill RBCs
Surefil SDR®flow (Dentsply Caulk) appeared on the market in 2010, becoming the first RBC of this type that touted the possibility of being applied in increments of up to 4 mm.14) The consistency of this bulk-fill RBC, as well as that of others that appeared later (such as x-tra base, VOCO; Filtek™BulkFill Flowable, 3M ESPE; Venus®BulkFill, Heraeus Kulzer), is similar to that of flowable resins and has been indicated as the base in class I and class II Black cavities, requiring an additional layer of 2 mm of conventional RBC in the occlusal side.14), (18
Other resins of conventional consistency appeared later, including Tetric Evoceram®Bulkfill (Ivoclar Vivadent) and x-tra fil (VOCO), which can be used in increments of up to 4 mm without the need for an extra occlusal layer made of a different material.19), (20) Yet there is a third variation: SonicFill™(Kerr), a bulk-fill RBC that needs a special sonic handpiece for its application and whose manufacturer has even touted that it can be used in 5 mm increments.21 It is activated by means of sound vibration, producing a momentary drop in viscosity during application. This resin is also indicated in classes I and II with no occlusal layer.21
It is then possible to establish a classification of these materials according to their viscosity, indication of use, and application technique (Figure 1).
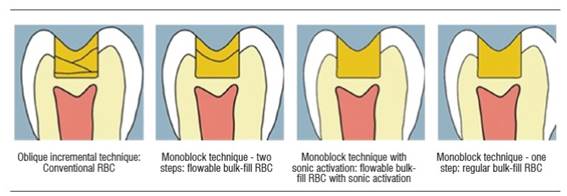
Figure 1 Illustration of the oblique incremental technique to apply conventional RBCs and the three types of bulk-fill RBCs application techniques
Ameloblasts differentiate from the inner epithelium of the enamel organ. For this process to take place, it requires the presence of dentin. This stage is called pre-secretory, which prior to the formation of mineral requires pre-dentine deposition by odontoblasts in the future dentin-enamel junction.
Flowable bulk-fill RBC to be used as cavity base.
Flowable bulk-fill RBC with sonic activation to be used as direct restorative material.
Bulk-fill RBC of regular viscosity to be used as direct restorative material. While manufacturers indicate the use of this material in the entire cavity, it is important to mention that in some cases it has been recommended to add a final surface layer of conventional RBC to provide better esthetic properties.22
COMPOSITION OF BULK-FILL RBCs
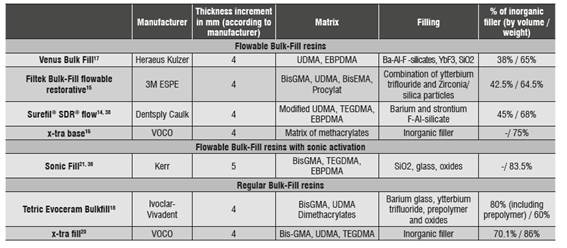
In general terms, the composition of bulk-fill RBCs does not differ much from that of conventional RBCs 18) (Table 1). The matrix of these resins is mainly based on monomers of Bis-GMA, UDMA, TEGDMA, and EBPDMA.18However, in some cases various monomers have been added and/or the classic Bowen monomer (Bis-GMA:2,2-bis[4-(2- hydroxy-3-methacryloxyprpoxy) phenyl] propane) has been modified14, 15 by monomers of lower viscosity.10), (23), (24
The manufacturer of RBC Surefil SDR flow patented a resin of dimethacrylate urethane that, as they indicate, includes the stress decreasing resin technology (SDR), which allows greater molecule flexibility thus avoiding the stress generated at the time of curing.10), (143M ESPE claims that Filtek Bulkfill flowable is based on 4 monomers: BisGMA, UDMA, Procrylat, and BisEMA, which have high molecular weight, reducing the development of shrinkage by polymerization. Furthermore, the addition of the Procrylat monomer would allow greater fluidity and thus would lower polymerization stress.25
Concerning the polymerization initiation system, major changes have not been announced by the manufacturers, with the exception of Ivoclar Vivadent.18), (19Tetric Evoceram Bulkfill (Ivoclar Vivadent) has a new polymerization initiation booster called Ivocerin, which is described as an initiator system based on Germanium of greater reactivity than that of camphorquinone, due to its greater absorption of 400 to 450 nm.26 It reportedly also has a filter of light pollution that ensures proper clinical work time.26
Concerning the amount of filling of these resins, filling percentages lower than conventional microhybrid and nanohybrid RBCs have been observed, comparable to the flowable RBCs in filling percentage by volume, but higher by weight.18It has been proposed that this lower proportion of filler, along with increased size (20µm) could increase curing depth in some bulk-fill RBCs by reducing the difference in refractive index between matrix and filling, thus improving light penetration.18), (27), (28
The materials are described according to manufacturer, suggested thickness increase, and composition. However, while the manufacturers have described some components and their respective modifications, there are still specific components that are widely unknown-something that can influence the final clinical behavior.29
SCIENTIFIC EVIDENCE ON THE PERFORMANCE OF BULK-FILL RBCs IN IN VITRO STUDIES
Curing depth
One of the relevant characteristics that need to be assessed in this type of resins is whether it is possible to obtain adequate curing depth in resin increments of 4 mm or more as indicated by the manufacturers. One of the common disadvantages of photo-cured RBCs is their limited curing depth and the possibility of insufficient monomer conversion in the bottom of the cavity preparation,5 this is relevant because it has been shown that poor photo-curing may cause RBC degradation, poor mechanical properties, and unwanted biological reactions due to the release of monomeric components that have not been polymerized.30), (36
According to the ISO 4049-2009 standard, curing depth should not be less than 0.5 mm than what has been established by the manufacturer.37 A study recently conducted by the ADA evaluated the curing depth of 10 different bulk-fill RBCs.38 The results showed curing depth values equal or greater than what is required by the ISO in bulk-fill RBCs: Quixx Posterior Restorative, x-tra fill, Filtek Bulk Fill Flowable, Surefil SDR, Venus Bulk Fill, and x-tra base. However, SonicFill, Tetric EvoCeram Bulkfill, and Alert Condensable Composite did not reach the values required by this standard.38
Other studies have also used the methodology indicated by the ISO specification, obtaining similar results. Garcia et al39reported average curing depth values of 3.46 mm for SonicFill, which is under ISO, while Surefil SDR and Venus Bulk fill resins yielded values that comply with the specification (average depth of cure: 5.01 mm). The authors explain that the smaller curing depth of SonicFill may be due to the lower light transmission by the material, due to possible resin pigments, which has been described as directly affecting curing depth,40), (41in addition to the existence of a greater amount of filler.
A study conducted by Flury et al42recorded curing depth values accepted by the standard for Tetric EvoCeram Bulkfill, Surefil SDR, Venus Bulk Fill, Quixxfill when polymerizing at 20 seconds, but when measuring Vickers hardness the ISO standard overestimated the curing depth value.
Notwithstanding, other studies have used other types of methodologies to measure curing depth, finding out that these materials do comply with the curing depths indicated by the manufacturers, including Tetric Evoceram Bulkfill, x-tra base,43), (44Venus Bulk Fill, Filtek Bulk, Fill and SonicFill.43), (45 However, it has been noted that there is great variability in the resulting mechanical properties when varying increment thickness, time of irradiation of light, and the lamp′s tip distance to the material.44), (46), (47
Various reasons have been suggested to explain the greater curing depth observed in bulk-fill RBCs in comparison to conventional systems. Three main reasons have been proposed: the incorporation of more efficient initiation systems in some resins,43greater translucency-which would allow deeper light penetration by reducing light absorption by pigments-, and decreased matrix/fill surface interface, which reduces light refraction.18
Shrinkage and polymerization stress
One of the disadvantages of the polymerization reaction occurring in RBCs is the development of shrinkage and stress in the material.48The amount of stress is mediated, among other factors, by the rigidity of the RBC, its releasing ability, and its curing rate. It has been reported that the effect of polymerization stress can cause various problems including cusp flexure, tooth fracture, and filtration or reduction of the material′s mechanical properties.49The incremental technique was developed as one of the strategies to reduce these effects, attempting to reduce the C factor of preparations (C factor: relationship between adhering surfaces / surfaces not adhering to a restoration).50 The rationale for this technique is that the application of thin layers of RBC increments would reduce the C factor, increasing the surface of free area not adhered to the walls of the preparation, thus releasing the shrinkage generated by contracting toward the material.50
Nevertheless, some authors have questioned the actual capacity of the incremental technique to reduce or avoid the effects of shrinkage and stress by polymerization.6), (11However, even before the introduction of bulk-fill RBCs it was inevitable to apply the RBC in increments of up to 2 mm, since this thickness allowed a proper depth of cure. With the emergence of bulk-fill RBCs which allow 4-5 mm increments, the usefulness of the incremental technique is now controversial.
Studies evaluating shrinkage and polymerization stress in bulk-fill RBCs are still scarce. When evaluating cusp flexure in premolars with class II restorations restored with bulk-fill RBCs, significantly lower values have been observed in comparing these (applied with the monoblock technique) with conventional RBCs (incremental technique).51It has also been observed that the development of polymerization stress is lower in bulk-fill RBCs in comparison with conventional RBCs and conventional flowable RBCs.52), (53
However, the polymerization shrinkage values found when compared to conventional flowable RBCs vary significantly according to the product. In the study by Garcia et al39there were bulk-fill RBCs with polymerization shrinkage values that are smaller, larger and similar to those of conventional flowable RBCs. Thus the relationship between the proportion of filler and polymerization shrinkage became apparent: the resins with the least amount of filling, and therefore with the greater proportion of resinous matrix, experienced higher levels of shrinkage by polymerization, and vice versa. SonicFill experienced a shrinkage by polymerization (1.76% in average) considerably lower than that of flowable bulk-fill RBCs (Venus Bulk Fill 4.4% and Surefil SDR 3.57%) with a smaller amount of filling.
With the results from the available research, it is difficult to determine if the lower cusp flexure observed by Moorthy et al52by using bulk-fill RBC is due to a smaller contraction of the resin or to changes in the mode of application of the material. In 1996, Versluis et al11 determined the existence of a smaller change in inter-cusp distance by applying RBC with the monoblock technique compared with the incremental method; this phenomenon was implemented by asserting that each increment would be causing deformation in the cavity′s walls with a movement of the walls downwards and towards the inside, which decreases the total volume of the cavity, and does not happen when applying it in a single increment. However, at that time, other reasons not related to shrinkage by polymerization and deformation, such as obtaining adequate adaptation and curing depth, made the use of the incremental technique preferable.
Therefore, it may be possible that the smaller cusp deformation observed with bulk-fill RBC51is due only or largely to the change in technique of application of the RBC. However, more research on this subject is needed, as it would help corroborate the results and whether the changes are due to the application technique or to bulk-fill RBC composition.
Marginal integrity
The ability to generate adequate marginal integrity is closely related to the development of shrinkage and stress by polymerization of these products, as these materials have been indicated to fill class I and class II cavities in a single increment. They are expected to be able to generate proper marginal integrity in adverse cavity conditions with a high C factor. Several studies have tested these products comparing them with conventional RBCs. In general, the results have not shown significant differences in marginal integrity when using bulkfill RBCs or conventional RBCs.22), (51), (54)-(56
Furness et al55compared bulk-fill RBCs and conventional RBCs used in class I cavities with both monoblock and incremental techniques. Their study did not show significant differences in terms of the restorations′ marginal integrity. Both techniques yielded higher proportions of margins free of gaps in enamel and dentin walls compared with pulp walls. On pulp walls, the percentage values of gap-free margins were low for both techniques (the average was 18% with the incremental technique and 9% with the monoblock technique), with no significant differences between them, showing that the use of bulk-fill RBCs does not eliminate the potential formation of gaps in the inner walls of the cavity.
Microleakage of bulk-fill RBCs in the cervical wall of class II restorations has also been evaluated, with no significant differences between bulk-fill RBCs and conventional RBCs used with the monoblock and the incremental techniques respectively.51This is consistent with two other studies that evaluated marginal sealing in class II cavities using bulk-fill RBC, with a 4-mm increase and an occlusal increase of 2-mm of conventional resin, showing that, in terms of percentage of continuous margins, there are no significant differences between the tested bulkfill RBCs and the conventional RBCs.22), (54
With similar results, the study conducted by Arslan et al56evaluated marginal microleakage observed in class V restorations, using a bulk-fill RBC as a cavity liner. No significant differences in marginal microleakage were found when using bulk-fill RBC liners of flowable resin or no liner at all, both in enamel and dentin.
In short, thein vitrostudies seem to agree that bulk-fill RBCs are able to provide marginal sealing comparable to that of conventional resins used with the incremental technique, which remains even after being subjected to load and temperature cycles. However,in vivostudies evaluating this property in clinical conditions have not been published to date.
Mechanical properties
Other important characteristics of bulk-fill RBCs that need to be taken into account are their mechanical properties. Since these RBCs are indicated for restoring posterior teeth, (and especially normal viscosity RBCs, which are intended to directly receive occlusal charge), it is important to assess whether they possess the appropriate mechanical properties to receive heavy occlusal loads.
The evaluation of the degree of conversion from monomer to polymer among these bulk-fill RBCs would not provide enough information on their mechanical properties, because since they have different monomers and/or modifications therein, they are expressed in different molecular conformations, and therefore a greater level of conversion in a composite resin with different components does not necessarily mean better mechanical properties.27
An evaluation conducted by the ADA in terms of bending strength in bulk-fill RBCs found greater values at 80 MPa (according to the ISO standard value) for all the tested resins: Quixx Posterior Restorative, x-tra fill, Filtek Bulk Fill Flowable, Surefil SDR, Venus Bulk Fill, x-tra base, SonicFill, Tetric Evoceram Bulkfill, and Alert Condensable Composite.18), (38The bending strength values of bulk-fill RBCs were similar to those of conventional nanohybrid and microhybrid RBCs, and higher than those of conventional flowable RBCs.18
The ADA also conducted an evaluation of surface hardness of normal-viscosity bulk-fill RBCs- which is relevant as they may be used with no conventional resin cover-finding out that bulkfill RBCs (Quixx Posterior Restorative, x-tra fill, Filtek Bulk Fill Flowable, Surefil SDR, Venus Bulk Fill, x-tra base, SonicFill y Alert Condensable Composite) comply with the specifications.38
In general, the amount of filling has been reduced in bulk-fill RBCs, something that becomes more evident in this type of flowable resins.
Seven bulk-fill RBCs were evaluated in a study carried out by Ilie et al.18They established that the values of flexural modulus, modulus of indentation, and Vickers hardness of bulk-fill RBCs were somewhere in between the hybrid RBCs and the flowable resins.18 Similar results were obtained by Czasch et al,27who evaluated two flowable bulk-fill RBCs, finding out a direct relationship between flexural strength, indentation module, and Vickers hardness with respect to the percentage of filling by volume.
Similarly, in evaluating creep resistance in bulkfill RBCs, a direct relationship was found with the proportion of filler by volume.57Flowable bulk-fill RBCs (Venus Bulk-Fill and Surefil SDR) showed lower resistance when compared with normal viscosity bulk-fill RBCs (Tetric Evoceram), as well as with flowable bulk-fill RBCs with higher percentage of filling (x-tra base). However, the creep resistance of Tetric Evoceram and x-tra base were appropriate, of approximately of 1%, in comparison with conventional nanohybrid RBCs.57
In terms of flexural strength, bulk-fill RBCs are similar to conventional hybrid RBCs,18), (38but in terms of indentation module values, hardness, flexural modulus, and creep, they are in direct proportion to the amount of filling by resin volume, which is significantly reduced in some bulk-fill RBCs.18), (27It is therefore necessary, as the manufacturer suggests, to add one occlusal layer of conventional resin in resins with lower percentage of filling, it is the flowable ones, to provide the mechanical properties required in areas with high occlusal loads.29
Handling properties
Composite resins are used to restore teeth imitating natural anatomy. A series of characteristics that favor their use have been described, including easy application in cavity, easy modelling, adhesion to tooth surface instead of to the instrument and capability of maintaining shape.58
In a study comparing viscosity, Filtek Bulkfill resin presented the lowest viscosity compared to nanohybrid and microhybrid resins; according to the authors, this is due to the bulk-fill RBC′s relative low load of filling by volume, which seems to be closest to that of conventional flowable RBCs.58 While flowable resins applied with a syringe are useful in situations in which access is difficult or where good penetration of the material is required, they are difficult to shape.
Petrovic et al,59in assessing the viscoelastic properties of RBF Surefil SDR, found out that its behavior differs from other flowable composite resins, which in clinical conditions would allow it to "self-level" in the cavity.
Studies evaluating the clinical management characteristics of these materials are scarce, so the information available here is minimal.
DISCUSSION
The emergence of bulk-fill RBCs has prompted a series ofin vitrostudies. However, to date noin vivostudies have been published, even though they could provide more relevant information on the performance of these materials in clinical situations
The introduction of bulk-fill RBCs that can be used in 4-5 mm increments raised two major questions. The first one is related to the capacity of being properly cured in such thickness increments and the second one is if the application of resins with a monoblock technique would be detrimental. The application of resins with the incremental technique emerged as a strategy to control shrinkage and the polymerization stress generated by RBCs; 2 however, the current scientific evidence on its effectiveness in this sense is not yet conclusive.4), (6), (11
The studies that have attempted to elucidate the effects on shrinkage and stress of polymerization in bulk-fill RBCs are scarce and in many cases the results are difficult to interpret.39), (52), (53Some studies have found lower shrinkage stress values and higher polymerization shrinkage values.39), (53 However, cusp flexure resulting after restoring with bulk-fill RBC using a monoblock technique is significantly lower compared with conventional RBCs using an incremental technique. These results totally agree with the observations by Versluis11 in the mid- 1990s, so maybe this is due to the change in the RBC application technique, rather than to changes in the RBCs themselves.
Using a monoblock technique with bulk-fill RBCs could potentially help overcome some of the disadvantages associated with the use of the incremental technique, such as increased probability of adding gaps or contaminants between increments, potential cohesive failure between increments, difficulty in the application of the resin in conservative cavities, extended clinical time for a correct application of the resin in layers, and the subsequent light-curing in each increment.57), (60), (61
Concerning the advantages of reducing operation times, it would be interesting to assess whether the monoblock technique really means clinical time reduction. In the case of flowable bulk-fill RBCs, they require a 2-mm occlusal layer with additional conventional resin, so it would be necessary to seal cavities with at least two increments and different resins, which could not be far from the operative time needed for 4-mm cavities, sealed with conventional resins; this is why further studies are suggested.
A more in-depth evaluation of these materials is required. While most bulk-fill RBCs do comply with the ISO specification on the ability to obtain a proper depth of cure with 4-mm increments,38), (39), (42), (44some studies suggest that not all types of bulk-fill RBCs would comply with the restrictions indicated by the ISO.38 This shows once again the importance of independent research to support the use of new materials or technologies.
Thein vitrostudies evaluating marginal integrity have yielded results comparable to those of conventional RBCs.51), (54), (55This is not the same for the studies that have evaluated their mechanical properties, which could be directly related to the resins′ filling proportion. This is why, in the case of flowable bulk-fill RBCs, the use of an occlusal layer of conventional RBC has been recommended in order to obtain the appropriate mechanical properties for restoring posterior teeth.
As with any new technique, it is vital to follow instructions closely. Bulk-fill RBC systems vary in their composition and have different photoinitiators systems; this is why it is necessary to ensure the use of the appropriate light source to achieve consistent results. Another aspect to keep in mind is that the viscosity of some of these resins is more flowable, so the proper use of band matrices is essential for proximal contact points- a topic that has not been discussed yet in scientific analysis due to lack of clinical studies-.
The results of clinical research on these products are expected to be published in the near future. According to these results, and hopefully with longterm randomized clinical trials, it will be possible to judge with greater scientific basis any benefits or difficulties of applying these new materials using the monoblock technique.
CONCLUSIONS
While using these materials could mean a significant simplification of the technique, by disregarding the need of applying the material in small increments, its clinical efficacy is still in doubt due to the absence of clinical studies that support it. Although the publishedin vitrostudies are promising, long-term clinical trials are necessary to provide evidence that support their clinical behavior.
Due to differences in composition and behavior observed inin vitrostudies, it is not possible to generalize the results obtained for a given type of bulk-fill RBC to the range of products that are labeled as such. The results obtained with a product cannot be extrapolated as generalizations. Finally, it is suggested to wait for more consistent evidence on these products, in order to help clinicians in making correct decisions.

