











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Facial traumas are the most common injuries in the human body.1)(2)(3)(4)(5) Trauma is defined as an injury caused by an external force6) exceeding the organism′s mechanisms of adaptation. In treating fractures, it is essential to use accessories for their reduction, fixation, immobilization, and consolidation, in order to achieve a complete, stable fixation; it is also necessary to protect the organs in the face, to keep craniofacial contours, and to recover the dental occlusion and articulatory function that existed prior to the injury.7)(8) ifferent methods of fracture fixation have been used throughout history, many of which only represent a historical importance currently.9) The fixation and immobilization technique used determines the mechanical situation in a fractured zone, and therefore the various healing patterns.10
In skull-maxillofacial surgery, internal rigid fixation (IRF) with miniplates and screws made of different highly pure titanium (Ti) alloys11) and resorbable materials that allow sufficient support is currently the method of choice for the surgical management of fractures and therefore is known as the "gold standard".12) IRF is defined as the fixation conducted directly on bone, which is stable enough to allow for an active and immediate use of the skeletal structure, and that seeks to achieve maximum stability of the fracture′s core by means of plates anchored to the bone with screws allowing primary repair of the fracture without formation of bone callus.13) Internal rigid fixation was first developed by surgeons and orthopedists, this is why the principles of IRF in the treatment of facial fractures are based on the principles established in orthopedics.14
A variety of metals are used for manufacturing osteosynthesis items, especially stainless steel, cobalt-chromium-molybdenum alloys, and pure titanium or its alloys. The metal of choice for manufacturing plates and screws is titanium (Ti) as it is highly compatible due to the oxidation of its surface, which occurs spontaneously when exposed to an environment with oxygen.15) Titanium is a light metal and it is the only one that presents dimorphism: in pure state, its crystalline stable microstructure is hexagonal and becomes cubic and unstable starting at 1620 °F. This allows combinations with different elements obtaining three types of alloys: a, b and a/b, with various crystallographic structures and diverse physical and chemical properties. Commercially pure titanium (TiCP) belongs to the group of a alloys.16
TiCP is composed of titanium and oxygen, along with other impurities; commercially, it is found with nitrogen, hydrogen, and carbon from the atmosphere resulting in four types of combinations representing four degrees of the ASTM F67 standard with varying degrees of strength and ductility. (16
Grade 1: With tensile strength of 240 megapascal (MPa), yield point of 170 Mpa, and 24% elongation.
Grade 2: Strength of 345 MPa, yield point of 275 MPa and 20% elongation
Grade 3: Strength of 450 MPa, yield point of 380 MPa and 18% elongation.
Grade 4: Strength of 550 MPa, yield point of 483 MPa and 15% elongation.
The characterization of materials implies determining their mechanical properties (elastic modulus, yield point, and tensile strength), as well as their chemical composition and microstructure. Material characterization methods include electron scanning tests or SEM and mechanical tests of traction, flexion, hardness, torque, etc. Before performing these tests, one should determine the maximum force that can be achieved according to material type and to the dimensions of parts to be characterized, in order to select a scale in which the maximum force does not correspond to the first or the last subdivisions of the device used to measure strength. The literature has reported that the magnitude of interocclusal force exerted by healthy patients during normal masticatory process ranges from 185.3 to 250.7 Newton (N), which declines until reaching 31% of this force one week after performing surgery on a mandibular angle fracture, and then increases 38, 37, 68, 27 and 58% respectively in the next five weeks. It has also been mentioned, as suggested in Champy′s studies, that the tensile forces produced in the mandible angle by masticatory forces and muscles reach 600 N.17) This reduction in masticatory force post-treatment of mandibular fractures has been attributed to protective neuromuscular mechanisms that occur in the body, as well as to traumatic or surgical damage of masticatory muscles. A delayed surgery usually leads to complications, with irreversible consequences or increased difficulty in fracture reconstruction.18
The osteosynthesis materials used at Hospital Universitario de San Vicente Fundación in the city of Medellín (Colombia) are supplied by importing companies. For facial fractures, they have systems of 1.5 mm and 2.0 mm, depending on the diameter of the screws being used for fixing the miniplates in manufacturing straight plates, orbital plates, and L-H-T-Y- and X plates; with 0.7 mm and 1.0 mm in thickness; 4, 6, 8, 12 and 20 holes, and screws ranging from 4 to 19 mm in length.
In Colombia there is only one manufacturer that recently started designing, manufacturing and distributing plates for fixing facial fractures that have a morphological configuration similar to the imported ones and use the same type of metal. The company has more than twenty years of experience in the production of osteosynthesis materials in the area of orthopedics, which have been used in studies in national and international academia.19)(20
It is necessary to analyze whether IRF plates made in the country have an in vitro mechanical behavior similar to those made abroad, to ensure adequate fixation and stabilization of fracture segments from a clinical perspective. This represents a starting point in the process of creation of innovative devices favoring the treatment of maxillofacial trauma.
Following are the results of this research, aimed at comparing the chemical composition and the mechanical behavior of two systems of miniplates and screws for internal rigid fixation (one national and one imported) used in the management of facial fractures, by subjecting the miniplates to flexural and tensile tests and the screws to torque tests.
MATERIALS AND METHODS
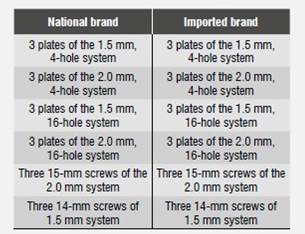
A non-probabilistic sample of 36 items was selected, including 24 miniplates and 12 screws (Table 1). Each item was assigned an identification number in order to avoid confusions during data collection and analysis. The information was brought to a database in Microsoft Excel, version 2007.
Table 1 Materials used in this study. National brand: CMx Precision® by Industrias Médicas Sampedro, Medellín (Colombia); Imported brand: MODUS® by Medartis®, Basel (Switzerland)
Microstructural characterization of materials and analysis of the chemical composition of plates were performed by means of scanning electron microscopy (SEM) and Energy Dispersive Spectroscopy (EDS) in order to find differences in the composition of each.
The response to traction and flexion in both systems of plaques was analyzed with mechanical strength tests in an Instrom universal testing machine, and torque response of both sets of screws with a Proto torque wrench, model 6169 A, with a capacity of 0-90 kg/cm (8.82 Nm).
The tensile testes were done with three 4-hole miniplates of the 1.5 mm and 2.0 mm systems of each of the two brands under evaluation, at a speed of 1 mm/min and 10,000 N load cell.
The flexure tests were carried out based on the ASTM F 382-99 standard (Reaproved 2003) "Standard specification and test method for metallic bone plates". Three 16-hole miniplates of the 1.5 mm and 2.0 mm systems of each of the two brands under evaluation were used at a 10,000 N load cell.
Torsion tests were conducted under standard ISO 6475: 1989 E "Implants for surgery - Metal bone screws with asymmetrical thread and spherical under-surface- Mechanical requirements and test methods", evaluating three 15-mm screws of the 2.0 mm system of each of the two brands, and three 14-mm screws of the 1.5 mm systems.
Statistical analysis
The obtained data were analyzed using the SPSS 18.8®statistical program (SPSS Inc., Chicago, IL, USA).
The univariate analysis calculated various descriptive measures such as median, range, and minimum/ maximum values. For the bivariate analysis, normality tests were conducted in order to determine the use of Spearman′s rank correlation coefficient. It was established that a high correlation would occur when the coefficients of correlation (rho) were greater or equal to 0.7, and low correlation when these values were lower.
The results were analyzed through Mann-Whitney U tests to compare medians among groups, and chi-square test (X2) to compare proportions. A statistical significance level of 5% was used.
RESULTS
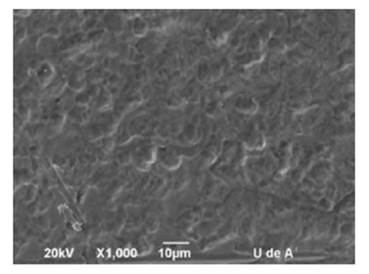
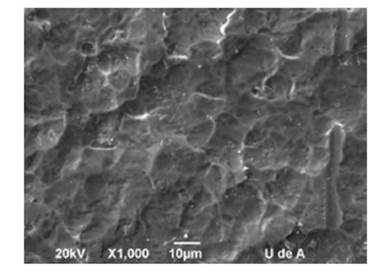
Characterization of the miniplates′ surface microstructure by means of SEM showed that the material used for manufacturing the plates of both brands (national and imported) only has an Α phase, which corresponds to titanium commercially pure (TiCP) (Figure 1 and Figure 2).
Analysis of the plates′ surface chemical composition using EDS yielded the following results:
The surface of national plates only has two chemical elements: oxygen (O) in 16.22% and titanium (Ti) in 83.78%, which corresponds to the chemical composition of titanium commercially pure (TiCP); the same components were identified in the imported plates in 25.77% oxygen and 74.23% titanium, which are also compatible with the composition of TiCP. This finding validates the results obtained with SEM.
Tensile tests evaluated the maximum load that the plates can resist before showing failure or fracture, as well as the deformation they reach at that point. Table 2 and Table 3 show the results of mechanical tensil testing for the 1.5 mm and 2.0 mm systems respectively.
Table 2 Tensile testing results of plates of the 1.5 mm system
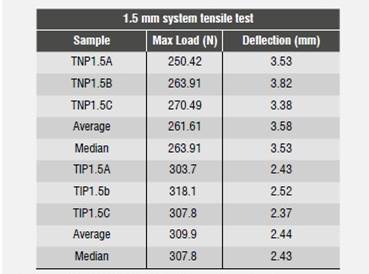
TNP: Traction National Plate. TIP: Traction Impor ted Plate
Table 3 Tensile testing results of plates of the 2.0 mm system
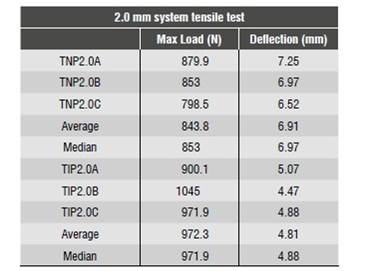
TNP: Traction National Plate. TIP: Traction Impor ted Plate
In both systems, the imported plates resist on average a greater load than the national plates; however, when analyzing the results through Mann- Whitney U tests to compare medians of maximum load and deformation between the two commercial systems (1.5 mm and 2.0 mm), there was a p value of 0.05. This shows that there were no significant differences, although it still unclear whether a bigger sample size would result in differences.
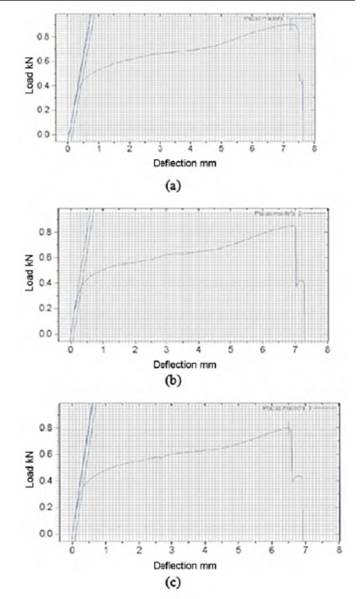
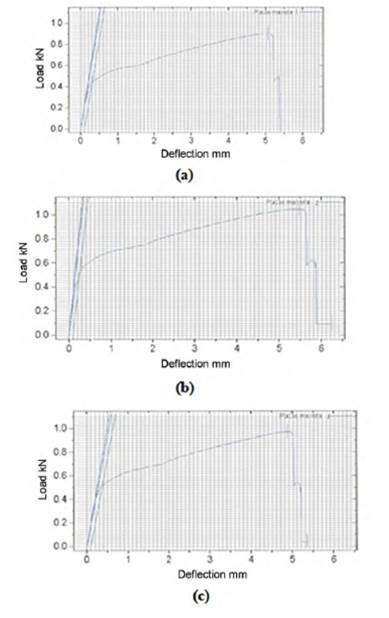
Figure 3 and Figure 4 show the load-deflection diagrams obtained from tensile tests of the 2.0 mm. plates. These results were used to calculate the modulus of elasticity in tension as shown in Table 4. This results confirm the hypothesis that significant differences could happen in a larger sample, since the national plates showed a modulus of elasticity on average 17% higher than that of the imported plates.
The flexural tests evaluated four variables for each plate in both systems. Maximum flexural load is the load applied to the plate at the time when it fails; maximum flexural deformation is the maximum deformation reached by the plate before failing; flexural rigidity is the ability of the plate to resist loads without showing large deformations; flexural strength shows the maximum force applied on a plate just before it cracks or breaks; and equivalent flexural rigidity is an indicator of the plate′s rigidity, relating plate geometry with the material used for manufacturing it.
Table 4 Calculation of modulus of elasticity for the 2.0 mm system
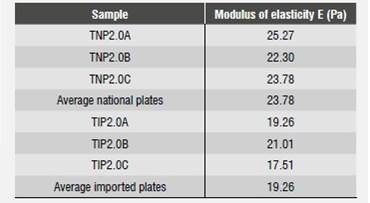
TNP: Traction National Plate
TIP: Traction Impor ted Plate
The results of flexural tests of national and imported plates of the 1.5 mm system are shown in Table 5.
Table 5 Behavior of the 1.5 mm system to flexion
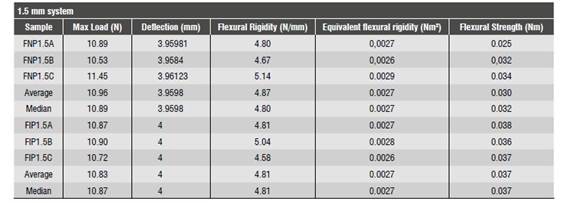
FNP: Flexion National Plate. FIP: Flexion Impor ted Plate
When comparing the variables using the Mann- Whitney U test, the p value was equal to or greater than 0.05, indicating no significant differences between the two brands for the 1.5 mm systems.
The results of flexural tests for the national and imported 2.0 mm systems are shown in Table 6.
Table 6 Behavior of the 2.0 mm system to flexion
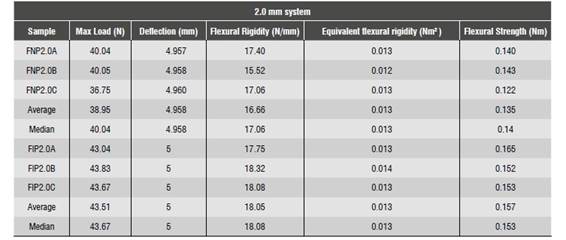
FNP: Flexion National Plate. FIP: Flexion Impor ted Plate
When analyzing the results of the Mann-Whitney U tests comparing variables, the p value for deflection was 0.037. This would suggest statistically significant differences, but in comparing medians of maximum load, flexural rigidity, and equivalent flexural rigidity, p value was 0.05, indicating no differences, although it still unclear whether a bigger sample size of plates of the 2.0 system of both brands would result in differences.
Finally, the torsion tests analyzed the maximum load resisted in torsion before screw failing and the deformation degrees before failure.
The torsion tests applied on national and imported screws of the 1.5 mm systems are shown in Table 7.
Table 7 Behavior of the 1.5 mm system to torsion
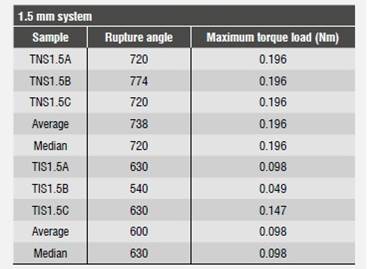
TNS: Torque National Screw. TIS: Torque Impor ted Screw
In comparing the medians of variables by means of the Mann-Whitney U test, the p value in torque angle and maximum torque load was lower than 0.05, which would suggest significant differences between the two brands of screws, with better results for the national screws.
Table 8 summarizes the results of the same tests for screws of the 2.0 mm system.
Table 8 Behavior of the 2.0 mm system to torsion
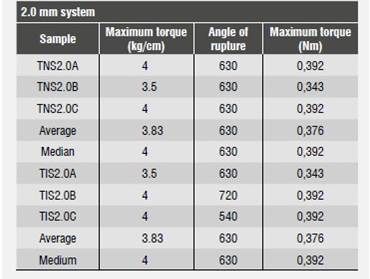
TNS: Torque National Screw. TIS: Torque Impor ted Screw
In comparing the medians of variables by means of the Mann-Whitney U test, the p value in torque angle and maximum load was lower than 0.05, which would suggest significant differences between the two brands of screws in the 2.0 mm system.
DISCUSSION
The AO/ASIF group (Association for the Study of Osteosynthesis / Association for the Study of Internal Fixation) suggests that titanium is the most biologically compatible material, and therefore is less likely to produce immunological reactions.22) The results of tests conducted in this research show that the two studied sets of plates are manufactured in commercially pure titanium, as evidenced by EDS and scanning electron microscopy, which showed a phase Α crystallographic microstructure in both brands, being consistent with current trends among manufacturers.
The vast majority of published comparative studies on the mechanical properties of miniplate systems have been carried out simulating specific clinical situations. This study conducted mechanical analysis of the devices as a prior step to clinical trials. The evaluation was conducted using the methods previously reported in other studies.21)(25)(28
The analysis of the results obtained by comparing the tensile and flexural tests of miniplate systems of 1.5 and 2.0 mm showed that the only significant differences occurred in deformation of the 2.0 mm system of both brands, and the differences of all other analyzed variables were not statistically significant. This may have happened because both brands use TiCP as raw material and have very similar designs.
On the other hand, analysis of tests on screws showed statistically significant differences when comparing screws of the 1.5 mm system, with the national system resisting a greater maximum torque load as well as higher rupture angle values.
These differences disappeared when the same variables were analyzed in the screws of the 2.0 mm system of each brand.
In comparing the maximum loads resisted by the two rigid internal fixation systems subjected to loads, we found out that both exceeded the loads on the masticatory system of healthy patients or patients with fractures, as reported in previous publications.17)(18) Therefore, the systems studied in this research met the necessary requirements to be used in the treatment of fractures of facial bones.
Previously published results indicate that the evaluated osteosynthesis material manufactured in our country has a biomechanical behavior similar to one of the imported brands most commonly used in the country, and that it could be taken into account when choosing a FIR system for facial fractures. It should be noted, however, that such decision should take into account costs, implant biocompatibility, and compatibility with tomographic images.
In the article by Edwards et al,21) components of the fixation system, i.e., the plate and its respective screws, were evaluated as a functional unit and not as separate elements, considering that their results would be closer to reality, and evaluating them as they would be used in clinical practice. However, the plates and screws were attached to a structure with different mechanical properties, which could influence the results.
In 2005, Choi et al25) used beef ribs to simulate fractures in edentulous mandibles and to analyze the mechanical behavior of the system using different strategies, but according to the findings by Hegtvedt et al,26) the mechanical behavior of materials shows differences when they are evaluated separately than when fractures are simulated using animal bones.
This is why it is important to correlate the findings of in-vitro mechanical tests of osteosynthesis material with clinical results in patients treated for fractures of facial structures using this type of material, performing a clinical comparative study of the same fixing systems in the future.
CONCLUSIONS
Both the imported and the national plates are manufactured in commercially pure titanium (TiCP), although the national plates have higher titanium content than the imported plates. This difference in chemical composition could have caused that during the flexural tests, the plates of the imported 2.0 mm system had more deformation than the national ones. All the other mechanical properties were very similar between both systems.
Concerning the screws, there were differences for the 1.5 mm system, showing that the national screws resist greater torque before failing, and they fail at a higher angle. The mechanical properties of screws in the 2.0 mm systems were similar.
These findings suggest that, in general, the mechanical behavior of both plates in imported and national brands are similar and both systems could be used as fixation material for facial fractures; however, for more conclusive results, a bigger sample of miniplates and screws of both brands would be necessary.

