











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
The contributions of adhesive systems to current restorative dentistry are unquestionably important as these systems are closely connected to the concept of "restoring and preserving" by minimizing the excessive wear of healthy dental structures during restorative procedures.1) The main goal of adhesive systems is to fully interact with tooth structures in order to ensure high bonding strength, which is evidenced by satisfactory sealing at the restorative material-dental tissue interface, resulting in good marginal adaptation and therefore in less microleakage 2) of bacteria, fluids, molecules, or ions in between the walls of cavity preparation and restorative material.3
Microleakage at the tooth-restoration interface is considered to be the main cause of restoration loss; its presence is associated with clinical manifestations such as postoperative sensitivity, recurrent caries, marginal pigmentation, and even pulp pathologies.4) Several factors contribute to the presence of these clinical manifestations, such as the physical properties of adhesive restorative materials, the linear coefficient of the material′s thermal expansion, occlusal stress, and polymerization shrinkage.5) Thanks to the permanent advances in adhesive systems, there have been considerable improvements in the field of adhesion to tooth structure, reporting less microleakage with current adhesive systems compared with their predecessors.6) The advances in terms of adhesive systems have been focusing on simplifying protocols and reducing time and steps of application, thus reducing the possibility of error by dentists in applying these substances, while encouraging the development of simpler adhesive systems.
The adhesive systems currently available in the market can be classified, according to their conditioning agent, as adhesive systems with either prior acid etching or total acid etching, using orthophosphoric acid as conditioning agent at a concentration of about 37%. When applied to enamel and dentin, this element is responsible for the removal of smear layer, triggering the formation of micropores in enamel and exposing collagen of both dentin and the outermost portion of dentin tubules. After having been used for decades, these systems have demonstrated outstanding clinical results.7
On the other hand, there are the self-etching adhesive systems, whose organic acids or orthophosphoric acid esters are incorporated to the adhesive primer, creating a single system that does not require washing the surfaces where they are applied. This creates small patterns of enamel demineralization, few significant morphological changes in dentin, and a smaller likelihood of triggering errors during adhesive protocols, since they do not require washing or drying surfaces, causing adhesive strength values that are similar to those achieved with systems requiring prior acid conditioning.8
Despite the apparent evolution of adhesive systems, the varying behavior of self-etching and total-etching conditioning systems on dentin and enamel also produces mixed results. Apparently, according to the literature, simplified techniques would be highly advantageous and reliable,1) however, the diversity of affected tissues during restorative procedures, the various locations of cavity preparations, and the influence of mainly occlusal forces raises this question: does the behavior of these systems changes over time? This study is therefore intended to evaluate the behavior of two adhesive systems, a self-etching system and an acid etching system, when applied in cavity preparations at the cervical third restored with similar techniques and subjected to two different artificial aging times, 6 and 12 months.
MATERIALS AND METHODS
This was a descriptive, comparative, experimental study with a sample of 60 human third molars extracted for medical prescription, with no cavities, fissures, or restorations, thus meeting the inclusion criteria: samples free of organic waste and preserved in a synthetic saliva substitute until use. Class V cavities were performed on the free side of each sample at the crown cervical third using a pre-designed aluminum matrix measuring 3 mm long and 3 mm wide. The cavities were previously delineated with pear-shaped diamond burs at high speed and with proper refrigeration, making sure they were 2 mm in depth, in order to simulate cavities usually found at this level during clinical practice. Used diamond burs were discarded every five preparations. A total of 120 cavities were then obtained, two per tooth, making sure that the cavo-surface margin angles of these cavities ended towards occlusal in enamel and towards gingival in dentin.
Once all the cavities were completed, the enamel and dentin of each cavity were disinfected with 5.25% sodium hypochlorite using cotton swabs for 60 s The samples were sorted out into four groups (n: 15). The two groups to be treated with conventional adhesive systems were applied 34.9% orthophosphoric acid (Vococid-VOCO) during 15 s in enamel and 5 s in dentin, and then rinsed with water using a syringe for 15 s; the cavities were wiped with the same device for 5 s to prevent complete dehydration. Then the adhesive system (Admira Bond-VOCO) was applied in two layers, leaving it to act for 30 s, spreading it with a soft stream of air from the syringe and photoactivating with halogen light (Litex 680A) for 20 s, according to the manufacturer′s instructions
The two remaining groups were applied the selfetching adhesive system (Futurabond NR-VOCO) by activating the single-dose bottle which was later punctured with a disposable applicator and mixed by swirling until getting a homogeneous mix. The adhesive system was applied in a thin homogeneous layer on enamel and dentin, rubbing the tooth structure softly for 20 s; the adhesive layer was wiped with a triple syringe for 5 s and photoactivated for 10 s with halogen light (Litex 680A), following the manufacturer′s instructions.
Application of the Admira-VOCO composite resin was similar for all groups, applying it in gradual increments of 1.5 mm and photocuring with halogen lamp (Litex 680A) for 40 s at a distance of 5 mm. The restorations were immediately polished with soflex discs in a decreasing sequence, and their roots were sealed at the apex using fluid resin.
The 60 samples, sorted out into two groups, were divided into four subgroups, A and B, subjected to sudden temperature changes, and taken to containers with water at 55° C, then 37° C, and finally 5° C, and then back to water at 55° C; they remained in each temperature for 5 s. This temperature change was considered to be a cycle; thus, samples in the A subgroup were subjected to 10800 thermocycling cycles, equivalent to 12 months of aging, and those in the B subgroups were subjected to 5400 thermocycling cycles, equivalent to 6 months of artificial aging.
Following the thermocycling process, all the samples were applied two layers of nail polishing on the entire surface, with a margin of 2 mm around the restoration, leaving them in contact with 0.2% methylene blue for 24 hours; then they were rinsed with water to remove excess colorant, and each sample was cut longitudinally obtaining two fragments per sample. Penetration of methylene blue at the tooth-restoration interface was measured in each fragment using a smooth probe and a millimeter ruler under a stereoscopic microscope with 10X magnification (Pathology Laboratory, School of Dentistry, Universidad Central del Ecuador), at the gingival and occlusal edges of the two restorations previously performed on the smooth sides. The measurements in millimeters were recorded in pre-designed Excel spreadsheets, which were later tabulated and statistically analyzed.
RESULTS
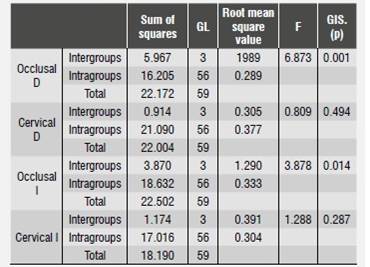
Data resulting from measuring colorant penetration in the occlusal and gingival thirds of each section in both the right side and the left side were tabulated (Table 1, Table 2, Table 3 and Table 4), obtaining averages for each wall of each fragment and for each sample in each group. The data were initially analyzed with Anova test (Table 5) yielding statistically significant differences in terms of microleakage between the occlusal and gingival sides among the groups (p < 0.05). The Tukey test was used to confirm this result, showing no difference between the adhesive systems used in the two evaluated surfaces (occlusal and gingival). Substantial differences were observed when analyzing the evaluated aging periods (p = 0.01), even considering just one of the adhesive systems (Table 6). In the four evaluated groups there was a proportional relationship between thermocycling time and the presence of microleakage, in such a way that the higher the aging time the higher the microleakage degree, regardless of the adhesive system used, being more noticeable at the gingival level of the restorations that were performed.
Table 1 Microleakage in millimeters using an acid-etching adhesive system (6 months)
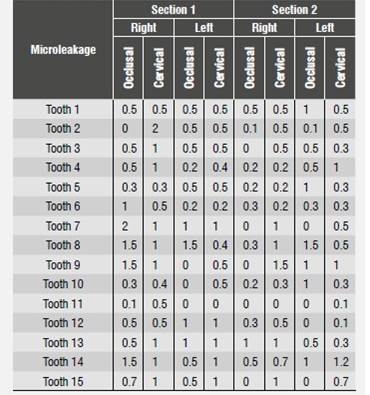
Source: Prepared by Gabriela Falconí Borja
Table 2 Microleakage in millimeters using an acid-etching adhesive system (12 months)
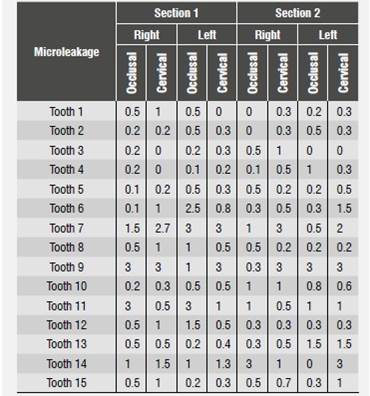
Source: Prepared by Gabriela Falconí Borja
Table 3 Microleakage in millimeters using a self-etching adhesive system (6 months)
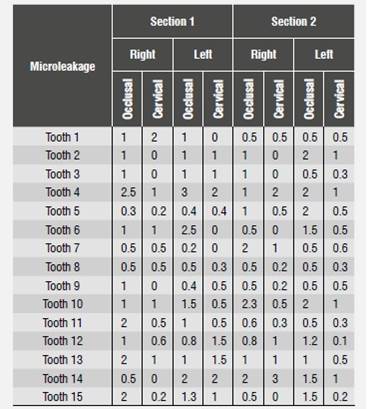
Source: Prepared by Gabriela Falconí Borja
Table 4 Microleakage in millimeters using a self-etching adhesive system (12 months)
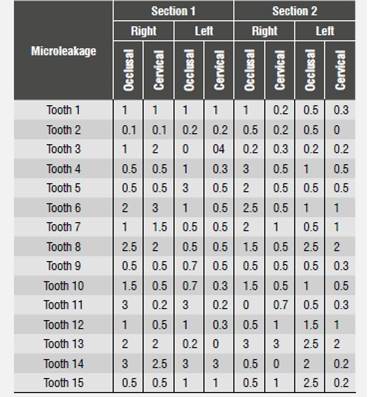
Source: Prepared by Gabriela Falconí Borja

DISCUSSION
Composite resin restorations are considered to have proper marginal sealing when bond strength forces exceed the forces created by polymerization shrinkage as well as those created by changes in thermal dimensions following polymerization, so that the efficient adhesion of composite resin to enamel and dentin will be fundamental for a successful restoration9 in the short and long term.
Composite resin adhesion to tooth surface pose challenges to clinicians due to the variety of tissues involved in this process, operator experience, variability of techniques, and above all because of the multiple available protocols. Hence the difference in microleakage degrees in this study at the occlusal and gingival margins, where the presence of enamel at the cavo-surface margin, mainly at the occlusal margin, is a key factor for success, which is expressed as sealing and subsequent absence of microleakage in this area -which did not occur at the gingival margin, where enamel structure is minimal, or even null in many cases-.10) This is consistent with similar studies 11)(12) assessing the two types of adhesive systems evaluated in the present study.
Restoring class V preparations is a challenge for clinicians due to their location and to the concentration of forces accumulating on these surfaces after contact with occlusal forces, and also because dentin in this area is usually of a tertiary type and its reaction to reparations make it unsuitable in terms of the histological interaction of the adhesive system to this type of dentine.13) Not to mention the series of tensions following the occlusal contacts accumulating in this area, which coupled with the contraction factor, or factor C -which is relatively high in this type of cavities-,12) the cavity shape itself, and even the difficulty in applying adhesive materials, promote the formation of marginal gaps between restoring material and dentinal tissue, resulting in marginal microleakage.
While this study used intact teeth, the cavities performed at the cervical third of the dental crown involve enamel in the occlusal side of the treated cavities, as well as dentin in the gingival sides of the cavities, which in part explains the findings in this study.
Advances in manufacturing dental biomaterials have provided clinicians with single-dose systems which apparently simplify the technique while minimizing possible handling errors; however, the findings of the present study showed that the totaletch adhesive system, which requires the application of orthophosphoric acid on enamel and dentin surfaces, was the system with the lowest microleakage degrees, which is explained by the demineralizing process produced after applying 37% orthophosphoric acid on the surfaces, with the subsequent removal of smear layer and fiber collagen exposure at the dentine, allowing better interaction of dental tissue and adhesive system.9)(12) This does not occur with self-etching systems, which in this study showed the highest microleakage degrees, agreeing with similar studies 14)(8) which findings are explained by their poor action on enamel.
The fact that the composition had acidic elements with low demineralizing and high moistening properties, coupled with the apparent easiness in using these systems, are factors that have traditionally promoted the use of self-etching adhesive systems in current dentistry; however, this requires prior training because dental professionals have traditionally been trained in using totaletching adhesive systems and their protocols, and therefore using different adhesive systems can cause problems during clinical protocols,22) resulting in errors-often irreversible-in the adhesive processes and its results.
The statistical analysis in this study showed that none of the two types of adhesive systems was totally resistant to infiltration of methylene blue, which was used as a coloring and penetration agent; the two tested adhesive systems had traces of marginal microleakage,13) being less noticeable with the totaletching system. The literature reports that selfetching adhesive systems, due to their characteristic composition, do not have an effective action on enamel, which may be related to their low pH (about 0.9), creating poor interaction on enamel;14) however, the results showed a similar behavior of the two adhesive systems evaluated, demystifying the poor action of self-etching systems on enamel.
While bonding agents and their compositions are determining factors for the presence of microleakage regardless of type, the care provided during restorative process, such as cleanliness and the preliminary actions to reduce contaminants, are essential.12) While microleakage tests are just one point of analysis on restorations durability, the fact of not requiring rinsing after acid conditioning would be a plus to be considered as part of the self-etching systems, as it reduces the possibilities of alterations in tissues, especially on collagen, and when used in total-etch systems, it often causes irreversible alterations, modifying the behavior and performance of the bonding system.15)(16
On the other hand, the possible antibacterial action of orthophosphoric acid when applied on tooth structures,17)(18) in addition to the increase in micropores on the surface where it is applied after partial dissolution of prismatic structures,19) with an increase in its microscopic rugosity and surface energy (which converts the acid in a proton donor and the enamel in a receiver), should be evaluated by comparing the integration of smear layer with adhesive systems,16) which is triggered by the action of self-etching systems on dental tissues-a factor that should always be considered and assessed in the decision of using any of the two systems-.
The restoration technique in itself is highly sensitive. The composition of composite resins requires rigorous and controlled conversion mechanisms where the incremental placement technique is fundamental to trigger the deleterious effects of polymerization shrinkage 9) on dental bonding. In this study, the amount of resin was carefully controlled, using 1.5 mm per layer, and it was applied in two increments with a single source of halogen light to cause its conversion-an element that was used despite different perceptions about devices for this purpose, as it is one of the most traditional and widespread procedures-.20
The method used for aging the adhesive interface and the restorative material, by storing samples in water at different temperatures for different periods of time, is a process of artificial aging widely used and recognized to assess the capacity of sealing material on tooth restoration,21) as hot water accelerates the hydrolysis of components generating stress at the interface by triggering a higher coefficient of thermal expansion of resins in relation to tooth structure.22) The careful performance of the protocols indicated for each adhesive system is fundamental to avoid failures during restorative processes. Further research in this regard should be conducted, as well as clinical longitudinal studies.

