











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Several studies in fully close apices report the response of teeth and supporting tissues to orthodontic movement.1)(2) Tooth movement with fixed appliances creates constant and continuous forces allowing bone remodeling with no apparent deleterious effects,3) according to the theory of presion-tension,4) which states that reabsorption occurs in the area of pressure and apposition in the tension zone.3) The cells responsible for and regulators of this mechanism are osteoclasts, osteoblasts, osteocytes, and their chemical mediators.5)(6) When these forces are excessive, they cause a larger area of hyalinization,7)(8) necrosis, and bone resorption, producing damage in periodontium, pulp, and teeth roots.3)(9) Of these effects, the most commonly attributed to orthodontic treatment is external root resorption.10)(11) This condition has been widely studied and is defined as loss of organic and inorganic component of hard radicular tissue, such as dentin and cement,12)(13) associated with other factors such as age,13)(14) gender,15) trauma,11) malocclusion,16)(17) root anatomy,18)(19) device type,20) used mechanism,16) characteristics of tooth movement,21)(22) force type,23)(24) and treatment time.25) We can say that its cause is in general multifactorial.10
Tooth movement with open apices which have not completed root formation has not been sufficiently studied. Some authors 26)(27) suggest that tooth movement in immature apices could be a risk factor for root resorption or reduced root length by premature apical closure, as described by Oppenheimen in 1942 and Phillips in 1955, who attributed it to the deformation of Hertwig sheath, which alters the calcification of apex and therefore root development preventing it from reaching maximum length.26)(27) In 2001, Consolaro et al noted that the movement of teeth with incomplete root formation creates a decrease in root length by early apex closing-which depends on embryo maturation of papillary and pericoronal tissue of dental follicle-and not by root resorption.28) On the other hand, some authors 25)(29) report that tooth movement does not produce adverse effects on teeth with immature apices, as described by Sameshima and Sinclair in 2001, who observed greater resistance to root resorption.25
The goal of this review is to determine the longterm effects of orthodontic tooth movement in teeth that have not completed root formation.
MATERIALS AND METHODS
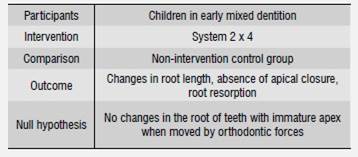
This systematic review was based on the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). It used the PICO format for systematic reviews (Table 1).
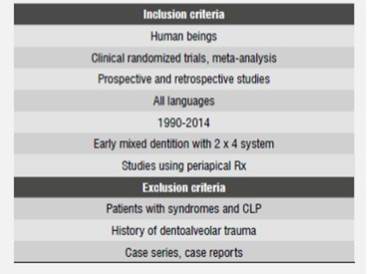
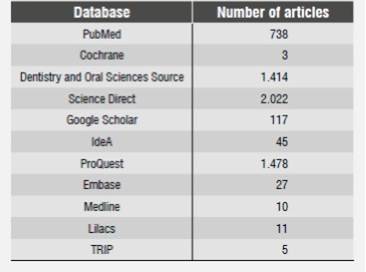
An electronic search was conducted in the following databases: PubMed, Cochrane, Dentistry and Oral Sciences Source, Science Direct, Google Scholar, IdeA, ProQuest, Embase, Medline, Lilacs, TRIP. A manual search was also conducted for grey literature in Universidad El Bosque Juan Roa Vásquez Library.The following inclusion criteria were used for article selection: articles published since 1990 to 2014, studies in humans, clinical randomized trials, meta-analysis, prospective and retrospective studies in all languages, studies in early mixed dentition with 2 x 4 system using periapical radiographs. The exclusion criteria were: studies on patients with syndromes and cleft lip and palate (CLP), history of dentoalveolar trauma, case series, and case reports (Table 2).
The following key words were used for both the electronic and manual search: orthodontic fixed appliances, orthodontic tooth movement, incomplete root formation, apical root closure, root maturation, root resorption (Table 3).
The initial selection of articles involved reading titles and abstracts to choose the most relevant studies according to the inclusion criteria; the full texts of selected articles were then reviewed.
The research question was: ¿Can orthodontic tooth movement in immature teeth induce changes in root length, absence of apical closure, root resorption, or no alteration at all, compared with a group that has not been intervened?
Key words, inclusion criteria and article selection were carried out by four independent researchers, and all disagreements were resolved by discussion.
The methodological qualification of studies was based on the systematic review by Lagravere et al,30) which was modified as described in Table 4.
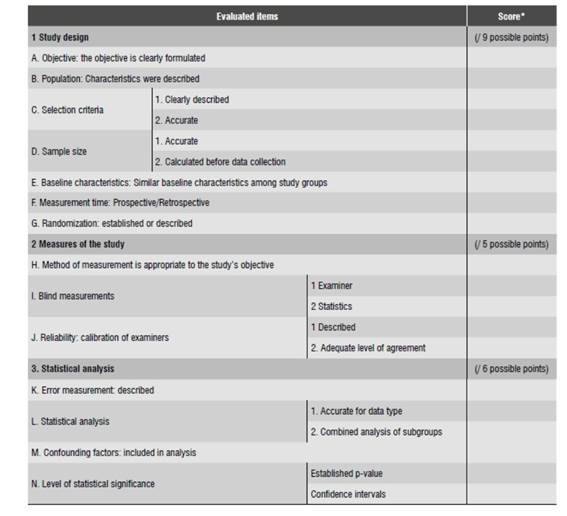
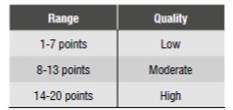
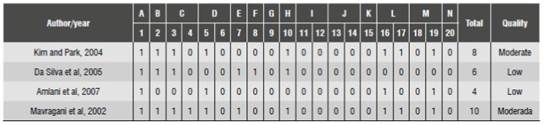
All selected full-text articles were subjected to this qualification. The maximum score was 20 points (Table 5). The researchers independently scored each of the selected articles, obtaining a methodological assessment scale by calculating ITC (intraclass correlation coefficient). The values ranged from 0.97 to 1, which are appropriate concordance values (Table 6).
RESULTS
The search results are described in the flow diagram (Figure 1). The electronic search yielded 5,870 articles (PubMed 738, Cochrane 3, Dentistry and oral Sciences Source 1,414, Science Direct 2,022, Google Scholar 117, IdeA 45, ProQuest 1,478, Embase 10, Medline 27, Lilacs 11, TRIP 5).
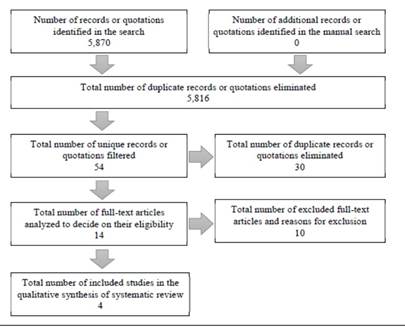
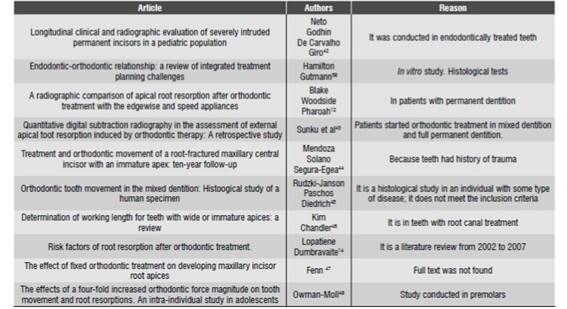
The manual search did not yield any results. After reviewing titles and eliminating duplicate records and quotations, 54 articles met the inclusion criteria. After reading the abstracts, 14 articles were selected for reading in full-text; 10 articles were excluded for the following reasons: they were histological studies, the treated teeth showed trauma or previous endodontic treatment, or were opinion articles by experts or literature reviews (Table 7). Finally, 4 articles were selected and the methodological evaluation was conducted. The characteristics of articles are listed in Table 8. This sample was not sufficient to run tests of statistical heterogeneity such as the Cochran′s Q test, I2 or H test. Therefore, the results will be presented in a qualitative manner to answer the following research question:What are the effects of orthodontic tooth movement in teeth that have not completed root formation?
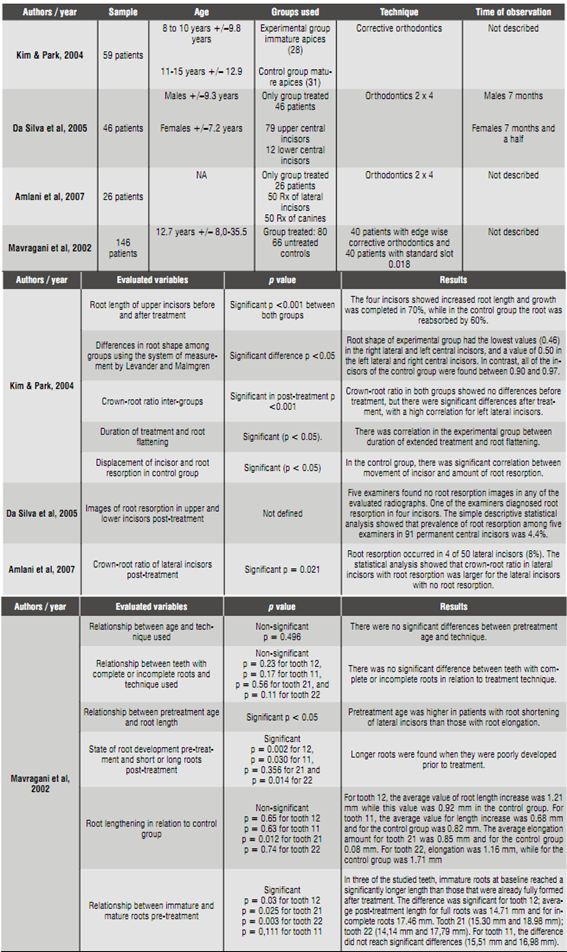
In 2005, Da Silva et al 31) found out that 5 examiners found no root resorption images in any of the evaluated radiographs. Only 2 examiners detected small signs of root resorption in periapical radiographs after leveling. One of the examiners diagnosed root resorption in 4 incisors, and the other in a single incisor that coincided with one of the 4 incisors already identified. Simple descriptive statistical analysis showed that the prevalence of root resorption among 5 examiners in 91 permanent central incisors was 4.4%.
In 2004, Kim & Park 32 found out that 4 incisors showed increased root length and that root growth was completed by 70% in the experimental group, while in the control group the root was reabsorbed by 60%. Changes in root length between the two groups were statistically significant (p < 0.001).
In 2002, Mavragani et al 33) found significant differences for three of the maxillary incisors when considering the pretreatment state of root development between shortened and elongated roots. They found longer roots when they were poorly developed prior to treatment (p= 0.002 for tooth 12,p= 0.030 for 11,p= 0.356 for 21 andp= 0.014 for 22).
Age of treatment start up
In 2002, Mavragani et al 33) observed that pretreatment age was higher in patients with root shortening of lateral incisors compared with patients with root elongation (p < 0,05). For the central incisor, age differences were not significant. Regression analysis showed that post-treatment root length in all studied teeth was related to age at baseline. The state of root development showed significance of correlation coefficient for lateral incisors only. In three of the studied teeth, immature roots at baseline reached a significantly longer length than the ones that were already fully formed after treatment. The difference was significant for tooth 12, with an average posttreatment length of 14,71 mm for complete roots and 17.46 mm for incomplete roots (p= 0.03). Tooth 21 (15.30 mm and 18,98 mm;p= 0.025); tooth 22 (14.14 mm and 17.79 mm;p= 0.003). For tooth 11, the difference did not reach significant differences (15.51 mm, 16.98 mm;p= 0.111).
Pre-treatment root length
Kim & Park 32) found out that, in the experimental group, root length was longer before treatment in 24 right lateral incisors (85.7%), 19 right central incisors (67.9%), 22 left central incisors (78.6%), and 21 left lateral incisors (75%). While in the control group root length was shorter in 19 right lateral incisors (61.3%), 23 right central incisors (74.2%), 20 left central incisors (64.5%) and 20 left lateral incisors (64.5%). Crown-root ratio between the two groups did not show statistically significant differences before treatment, but differences were significant after treatment, with a high coefficient of correlation for left lateral incisors (p< 0.001).
In 2007, Amlani et al 34) found root resorption in 4 of 50 lateral incisors (8%). Statistical analysis showed that crown-root ratio in lateral incisor was larger for the lateral incisors with no root resorption (p= 0.021).
Root length during treatment
Mavragani et al 33) found that evaluation of changes in root length during treatment showed an average of root length loss of 1.86 mm for tooth 12 (0.26 SE, −3.8 to 6.54 mm range); 1.82 mm for tooth 11 (0.26 SE, −3.82 to 8.9 mm range); 1.93 mm for tooth 21 (0.25 SE, −5.7 to 6.27 mm range) and 1.78 mm for tooth 22 (0.33 SE, −8.39 to 7.48 mm range). Negative values were found in 50 of 280 teeth, suggesting root canal elongation.
Post-treatment root length
Kim & Park 32) found statistically significant differences in root shape by means of the Levander & Malmgren measuring system, which uses five resorption degrees to identify levels of root resorption. The experimental group had the lowest value (0.46) in the right lateral and left central incisors, and a value of 0.50 in the left lateral and right central incisors. In contrast, all of the incisors in the control group were found between 0.90 and 0.97. The difference was statistically significant for the four incisors, with <0.05pvalue. Crown-root ratio in both groups showed no pre-treatment differences, but there were significant post-treatment differences, with a high correlation for the left lateral incisor (p < 0.001).
Mavragani et al 33) found out that roots which elongated during treatment had a root length similar to that of un-treated roots in individuals of the same age. For tooth 12, the average value of root length increase was 1.21 mm and in the control group the increase was 0.92 mm (p= 0.65). For tooth 11, the average value of length increase was 0.68 mm, and for the control group was 0.82 mm (p= 0.63). The amount of average elongation for tooth 21 was 0.85 mm and for the control group was −0.08 mm (p= 0.012). For tooth 22, elongation was 1.16 mm, while for the control group was 1.71 mm (p= 0.74).
Technique used and pre-treatment age
Mavragani et al 33) found no significant differences between pretreatment age and technique used (p= 0.496). Similarly, there was no significant difference between teeth with incomplete or complete roots in relation to treatment technique (p= 0.23 for tooth 12,p= 0.17 for tooth 11,p= 0.56 for tooth 21 andp= 0.11 for tooth 22).
Duration of treatment and root resorption
Kim & Park 32) found correlation between treatment duration and root flattening (p< 0.05) in the experimental group.
DISCUSSION
This systematic review included four articles with low to moderate levels of evidence. Of the four articles, three were retrospective and one was prospective. None of them calculated sample size, and they did not report randomization nor researcher or statistician blinding. Also, none of them reported intra-examiner concordance and none established confidence intervals. Only one study considered confounders, measurement error, or intra-examiner calibration.
There are few studies on root behavior in teeth with open apices where the biological process of root formation is still in process. There is controversy over the biological risk of orthodontic movement in immature apices. On the one hand, some authors 30)(36)(37) agree that teeth that have not completed root formation are less prone to resorption after inducing movement with fixed appliances. In addition, Linge et al 37) and Mavragani et al 33) report lower root damage in apices with incomplete root formation. However, Hendrix et al 29) found out that teeth with open apices which do not achieve the average standard length usually have longer roots compared to teeth with closed apices, probably due to apex displacement during treatment. Hamilton & Gutmann 38) reported that premature apical closure occurs when applying orthodontic forces on immature apices. In consequence, the main variable evaluated in their systematic review was the changes occurring when tooth movements were applied on apices that had not completed root formation.
Concerning changes in root length before and after treatment, the study by Kim & Park 32) found statistically significant differences between both groups, reporting increased root length that is complete by 70%, while in the control group the root reabsorbed by 60%. Their study concludes that the resorption degree was low because participants were treated without extractions and therefore both displacement distance and duration were short.
Concerning crown-root ratio, Kim & Park 32) reported no significant differences before treatment between roots with immature apices and those that had completed their development. However, there were significant post-treatment differences between the two groups, since immature roots tend to grow while roots with mature apices are reabsorbed and shorten.
Kim & Park 32) found significant differences in terms of root shape after orthodontic treatment in both groups, using the measuring system described by Levander and Malmgren,39) which can be explained because the final shape of immature apices was similar to the shape of mature apices.
Similarly, the change in root shape was associated with treatment duration: longer treatment periods allowed complete root formation, followed by reabsorption and shortening. In conclusion, while the possibility of reabsorption in immature apices is low, in longer treatments one should not expect differences with mature apices.
Concerning changes in root length and shape, Kim & Park 32) concluded that starting orthodontic treatment before full root formation is convenient for reducing root resorption. However, their study is based on changes observed in x-rays of immature apices, excluding other factors such as histological aspects, history of trauma, or habits.
On the other hand, Da Silva et al 31) reported that the risk of resorption or any other alteration in roots in formation during induced movement in permanent incisors with open apices is practically non-existent. In the same way, Rudolph 35) agrees that orthodontic treatment is less damaging in roots in formation, i.e., when it is started early. However, this result should be taken carefully because of the methodology used (panoramic radiographs), since the authors took chronological age as a reference instead of the stage of root formation, thus providing little information on the stage of root formation.
Subsequently, by means of periapical radiographs, Linge et al 37) studied the incidence and extent of root resorption in maxillary incisors, finding out that root resorption was two times higher in apices which had completed their formation, compared with immature apices.
Da Silva et al 31) concluded that, from a radiographic perspective, there is no evidence of iatrogenesis in root integrity during orthodontic movement in permanent central incisors with incomplete formation.
Mavragani et al 33) agree, as in their study they found out that teeth with partial root formation prior to treatment reach longer root length than teeth with fully formed roots when treatment starts. Therefore, they conclude that orthodontic treatment does not cause root resorption in teeth with immature apices.
Based on the obtained results, we must bear in mind that most orthodontic studies were scarce and had methodological weaknesses. However, the findings of the present review agree with those of several authors,30)(36)(32) who suggest that orthodontic treatment in teeth with incomplete root formation does not represent a biological risk for its development.
CONCLUSIONS
Based on the results of the present study, the following conclusions can be drawn:
1. There are no alterations in the final root length of incisors that have not completed apical closure and which are moved with fixed orthodontics.
2. The technique used does not seem to be relevant in final root length.
3. These results should be taken cautiously because the resultant evidence was low to moderate.
4. Long-term randomized clinical trials are needed in order to show root alterations in teeth that have received early treatment with forces.

