











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
There is mounting evidence that oral pathologies affect the most disadvantaged population in society, increasing the disease burden of these groups.1 In the case of dental caries, which used to affect a large part of the general population in the past and is currently concentrating on a segment of it, the efforts are now focused on non-biological aspects beyond the individual ones. Some authors state that overall improvements in dental caries and periodontal disease indicators in middle- and high-income countries have not modified the relationship of these indicators with social conditions and health inequalities. Various studies associate caregivers’ low schooling levels and low family income with a higher prevalence and severity of dental caries.2,3
Dental caries in children under the age of six-early childhood caries-commonly affect groups with higher poverty levels. In addition, the indicators of the disease experience at these ages are in contrast with the improvements in indicators among the school-age population, and have even increased in low- and middle-income countries.4,5 Hence the World Health Organization (WHO) states that this is a public health problem, impacting overall health and quality of life.6,7 Some authors point out that a large number of unmet oral health needs during early childhood and the presence of the disease during this stage of life is an indication of other inequalities in health.8,9
According to the latest National Oral Health Survey (Estudio Nacional de Salud Bucal 2013-2014, ENSAB IV), the oral health situation of this population group in Colombia has remained unchanged in the last two decades, considering that by 2014 a total of 62.1% of five-year-olds had experienced dental caries compromising cavities in dentine, compared with 60.4% reported in the III Estudio Nacional de Salud bucal, ENSAB III, 1998. The ENSAB IV also found out that 29.3% of children experience dental caries by the age of one year, 6% of them with severe lesions; by the age of three, dental caries experience involving dentin gets to 47.1%, a value that increases to 83% when all lesions are considered, and at five years of age the percentage of children with dental caries experience reaches 88%.10
This latest national survey shows some differences in caries experience in primary dentition by region and type of affiliation to the General System of Health Social Security, but the data do not allow further analysis, nor do they suggest differences in terms of inequality. On the other hand, a higher proportion of dental caries has been found in low-income children in the city of Medellín,11,12 and the latest population study, carried out in 2009 with a sample from all the city’s schools, yielded statistically significant differences in both experience and prevalence of the disease in five-year-olds attending schools located in middle- and high-income neighborhoods, in contrast with those in schools located in low-income neighborhoods.13)
An epidemiological study was recently conducted in the municipality of Andes, finding out differences in terms of basic indicators of dental caries experience and prevalence by area of origin and social segments identified in the study population.14,15
The issue of social inequalities and health inequities is complex and usually connected to conceptual and methodological controversies. The present study stems from the Pan American Health Organization’s proposal to use methods for measuring inequalities in health based on basic health indicators clustered by geopolitical units. In this proposal, the term ‘inequities’ refers to unnecessary, unjust, and avoidable unequal conditions, and this requires deeper analyses, as it can be the origin of health inequalities. Measuring such inequalities is a first step not only towards their identification but also for decision making.16
The aim of this article was to identify the distribution of indicators of dental caries experience in children under the age of six in the municipality of Andes, a population group that in Colombia has been defined as early childhood.
MATERIALS AND METHODS
An analysis was conducted using the records from a database created during a cross-sectional study for the construction of a baseline of health indicators in children aged 0 to 5 years, a project conducted in 2014 in the municipality of Andes (Antioquia) and approved by the Ethics Committee of the Universidad de Antioquia School of Dentistry (Act No. 22 of 2013).
The records correspond to 623 children from urban and rural areas, from a sample calculated based on a reference population of 3,525 individuals, with 95% confidence interval, 2% sampling error, and proportional allocation per area of residence. The final selection of children in the urban area was made by probabilistic sampling, and in the rural area a call for participation was done in health centers.
The information was recorded by two dentists calibrated in the IV National Oral Health Survey based on the criteria of the International Caries Detection and Assessment System (ICDAS).10 The proposal to merge the ICDAS lesions code 1 with those of code 2 was considered as the data were recorded.17,18 Prior to the clinical examination, an adult brushed the child’s teeth; the dental surfaces were dried with a gauze, conducting a detailed visual inspection of each surface.
The presence of one or more decayed (either cavitated or non-cavitated), filled or missing surfaces of primary teeth due to caries in the examined children was considered as early childhood caries (ECC), following the definition of the American Academy of Pediatric Dentistry,19 which includes children under six in this group, coinciding with the definition of early childhood by the Colombian state in Law 1098 of 2006.
The different progression levels of dental caries lesions proposed by the ICDAS system were taken into account, differentiating among initial or A lesions (ICDAS 1 and 2), moderate or B lesions (ICDAS 3 and 4) and extensive or C lesions (cavities that compromise the dentin, ICDAS 5 and 6).20,21 Additional records included the condition of healthy surfaces (with no caries experience), as well as missing and filled teeth due to caries.
The definition of dental caries experience was taken from the IV National Oral Health Survey, as the proportion of people who at the time of examination show signs of treated or untreated caries at some point in their lives, including the presence of carious lesions in any of its phases (initial, moderate or advanced) or any sequelae of it (filled or missing surfaces due to caries). Similarly, calculations were performed for the d ICDAS5-6 mfs index, which include the experience of extensive lesions, and d ICDAS1-6 mfs index, when the initial stages of caries were also included.10
Data were analyzed in version 23.0 of the IBM-SPSS® software, as well as Excel and Epidat 4.1, calculating the mean and median values of the affected dental surfaces for the different ICDAS codes, and estimating the d ICDAS5-6 mfs and d ICDAS1-6 mfs indexes. The quantitative variables of the indexes components were subjected to normality tests by age, finding out no normal distribution; therefore, the data were analyzed by means of non-parametric tests (Kruskal-Wallis). If these yielded no statistically significant differences, multiple range analyses (Games-Howell) were performed to determine which ages showed differences.
The Mann-Whitney U test was used to compare the medians of d ICDAS5-6 mfs and d ICDAS1-6 mfs indexes between urban and rural areas in each age.
Inequality in distribution of early childhood caries was assessed through the Lorenz curve and the Gini index, sorting out the population in a hierarchical manner by means of the cumulative proportion distribution of the d ICDAS5-6 mfs and d ICDAS1-6 mfs indexes (Y-axis) and the cumulative proportion of the studied population (X-axis).16,22
RESULTS
In total, 551 children (88% boys and 89% girls) had early childhood caries. When considering the number of surfaces with cavitated carious lesions compromising dentine and the number of filled and missing surfaces due to tooth decay, an average d ICDAS5-6 mfs index of 3.3 ± 7.4 was observed, with values of 3.5 ± 8.0 in the rural area and 2.7 ± 5.7 in the urban area, although the differences were not significant. When initial and moderate carious lesions were included, the d ICDAS1-6 mfs index increased to 14.3 ± 15.1, reaching 15.7 ± 15.8 in the rural area and 11.3 ± 12.8 in the urban area-statistically significant differences according to the Mann-Whitney U test (p value < 0.001)-. Table 1 shows the values of d ICDAS5-6 mfs and d ICDAS1-6 mfs indexes and their standard deviations, as well as the medians with their interquartile range by age and area of residence.
Table 1 d ICDAS5-6 mfs and d ICDAS1-6 mfs indexes mean (x̅) ± ,standard deviation (SD) and median (Q2) with their interquartile range (IQR) by age and area of residence in children under 6 years from the municipality of Andes, 2014
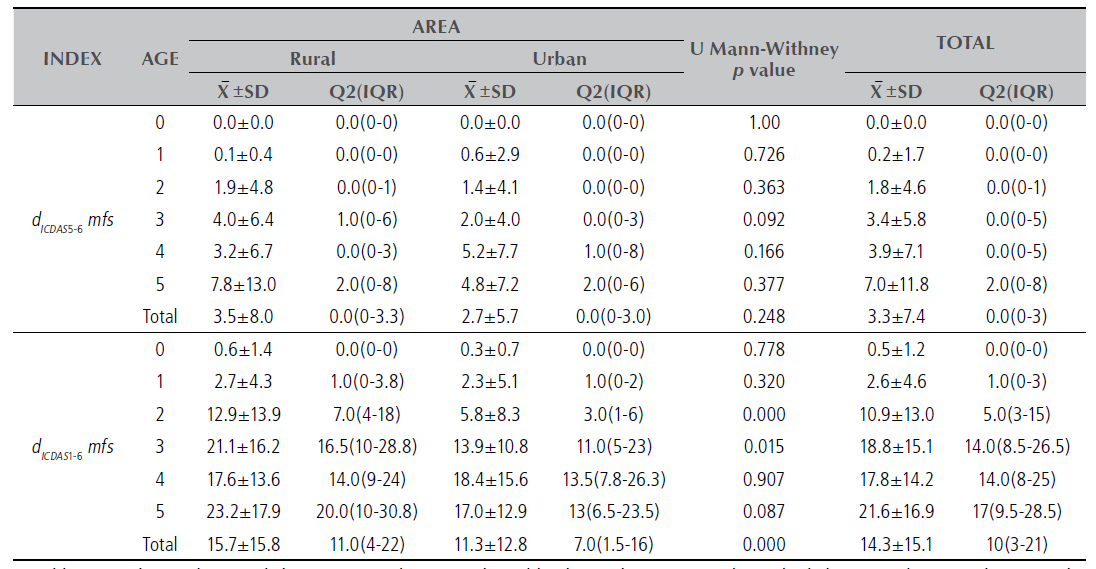
In addition to the medians and their interquartile range, this table shows the means and standard deviations because these are the benchmarks of comparison with other studies.
The distribution of the components of d ICDAS5-6 mfs and d ICDAS1-6 mfs indexes shows a greater share of surfaces with initial dental carious lesions compared to moderate and extensive lesions and to filled or missing surfaces due to dental caries. Table 2 shows the indexes values and their components by age.
Table 2 Surfaces mean (x̅) and standard deviation (SD), median (Q2) and interquartile range (IQR) by dental status per age in children under 6 years, municipality of Andes, 2014
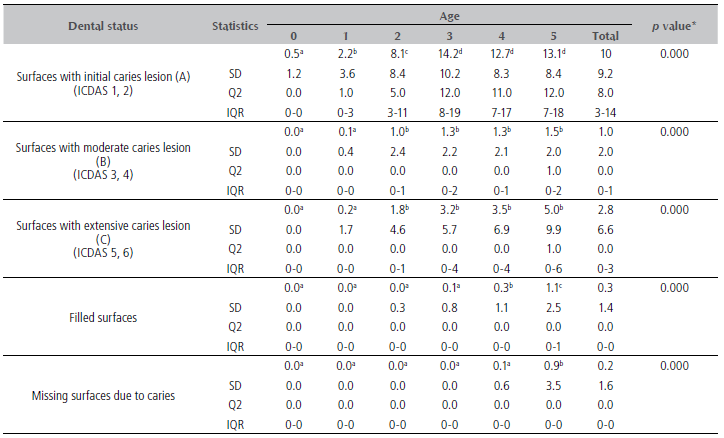
* Kruskal-Wallis test. Different superscript letters indicate mean differences among ages (Games-Howell’s multiple range test)
The values distribution of the d ICDAS5-6 mfs index shows that 61.8% of the examined children did not have experience of extensive dental caries lesions; and of the remaining 38.2%, 19.3% had indexes of 1 to 5, while the values ranged from 6 to 10 in 9.8% (Figure 1a). When all dental caries lesions were included, the d ICDAS5-6 mfs index was 1 to 5 in 25.2% of the examined children, and 15.1% showed values of 6 to 10 (Figure 1b).
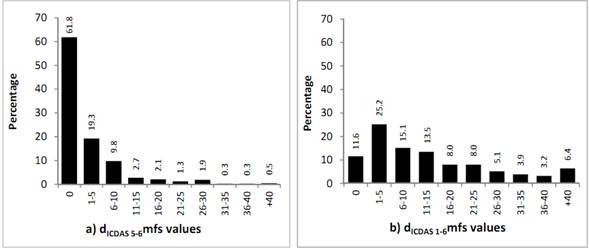
Figure 1 Percentage distribution per the d ICDAS5-6 mfs and d ICDAS 1-6 mfs index values in children under 6 years of age from the municipality of Andes, 2014
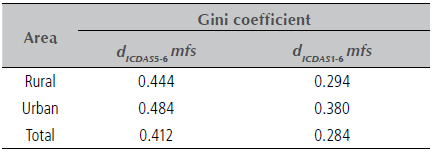
The analysis of inequality in the distribution of the disease among the evaluated children was carried out by means of Lorenz curves and the calculation of the Gini coefficient for the accumulated distribution of values of the d ICDAS5-6 mfs and d ICDAS1-6 mfs indexes, in accordance with the proposal of the Pan American Health Organization (Figure 2). The curves show greater inequality when built based on the more extensive lesions than when all lesions are included. Figure 3 shows the Lorenz curves of the d ICDAS5-6 mfs and d ICDAS1-6 mfs indexes by area of residence, and Table 3 displays the Gini coefficients values for the accumulated frequencies of the d ICDAS5-6 mfs and d ICDAS1-6 mfs indexes, with a similar distribution by area of residence in the most extensive lesions.
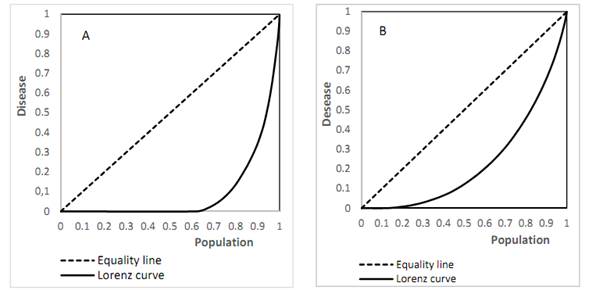
Figure 2 Lorenz curve for the accumulated distribution of the d ICDAS5-6 mfs (A) and d ICDAS1-6 mfs (B) indexes in children under the age of five. Municipality of Andes, 2014
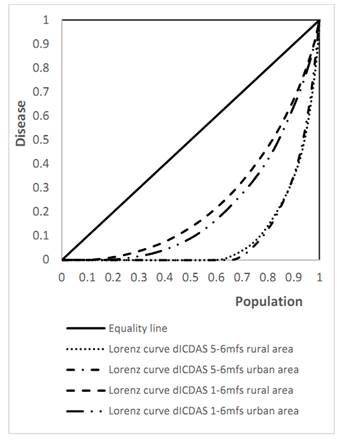
Figure 3 Lorenz curve for accumulated distribution of the d ICDAS5-6 mfs and d ICDAS1-6 mfs indexes in children under the age of six, by area of residence. Municipality of Andes, 2014
DISCUSSION
The presence of early childhood caries in a high proportion of children aged 0 to 5 years from the municipality of Andes is a challenge for the design of programs, plans and policies.14 In addition, the performed analyses show differences in terms of severity of the disease, according to the indicators calculated by surfaces, their distribution in the examined children, and the use of measuring methods, suggesting the existence of inequalities in both urban and rural areas.
The severity of the disease, expressed in the number of decayed, filled or missing surfaces due to caries, reflects not only the cumulative character of the disease but also the unmet health care needs in this population group. An average of 0.2 surfaces with dental caries in dentine at the age of one year increases to 7.0 at the age of five, with higher values if including initial enamel lesions, which require other types of treatment options to control their progress. The analysis of lesions per tooth surface also shows the tendency to increase with age and a greater presence of the decayed component (largely represented by initial and moderate dental caries lesions) than filled and missing teeth due to cavities.14 It is not possible to compare the data in Andes with the national survey, since no indicators by surfaces have been published yet; however, these data are higher than those reported in an area of low and medium socioeconomic stratum of the city of Medellin with the same indicators.12
What is most striking, however, is the presence of large variations in the disease values among the examined children. This variations are expressed in high standard deviation values with respect to the means and in a skewed distribution of the disease-and these values become higher if the analyses focus on the most severe lesions (ICDAS 5 and 6 already compromising dentin) instead of considering all lesions-. This phenomenon has already been identified; in fact, Bratthall highlighted the issue,23 and other authors have incorporated it in their analyses24 because it reflects how, while the majority of the population is free of dental caries lesions compromising dentine and can be treated with simpler measures (61.8% in the present study), the greatest burden and severity of the disease concentrates in a segment of the population.
Analyzing differences in a population can be useful not only to identify the challenges faced by dental services but also to identify situations of inequity, which not only stem from the assessment of health indicators but have also been suggested in this population in evaluating the averages of the disease by social segment. This has marked implications for how to address oral health problems,3 especially in early childhood. In addition, the Lorenz curve calculation showed that the area between the distribution of dental caries in the examined population and the equality line reflects an uneven distribution of dental caries indicators-a situation also reported in Brazil by the age of twelve.25
As is the case with the disease distribution, the Lorenz curve shows a greater inequality when considering the most severe lesions than when all lesions are included, and the same occurs with the Gini coefficients, which move further away from zero when the disease is analyzed in its most severe forms. This shows that the greatest differences occur in terms of severity of early childhood caries rather than in prevalence of all lesions, regardless of progression-a first step towards the identification of inequalities that may reflect inequities in access to goods and services.
The present study describes a finding regarding inequality in the distribution of dental caries in the general population-a situation observed in urban and rural areas- and is not aimed at verifying the hypothesis of inequality per area of residence. It is not a measurement of inequities either; the analysis of inequalities using the Lorenz curves and the Gini index is based exclusively on a basic indicator of oral health, without considering other aspects of living conditions.
While oral health studies like this and others22,24-25are making progress in recognizing differences, and the issue of inequalities has been incorporated in the analysis of various publications and consensus, most actions and recommendations deal with interventions based on risk analyses, which may be useful in terms of individual care provided by health services, but are limited in scope. In this regard, Watt questions such approaches and, while recognizing the progress in incorporating oral health into general health, points out that the actions are still limited to proximal causes related to individual behaviors.3 To this author, the evidence validates the need to impact the broader determinants and policies requiring structural changes, legislation controls, fiscal policies, a greater focus on the earlier years of life, community actions, reorientation of health services, improvements in access to health services, and prioritization of groups with greater needs, to name just a few aspects.3
Some progress has been made in Colombia with the inclusion of children aged 1, 3 and 5 years in the IV National Oral Health Survey and with the emergence of research accounting for the prevalence of dental caries in children under six years of age, like the one carried out in the municipality of Andes. This is a first step and makes part of the recommendations made by groups of experts and health agencies.6 However, more attention to inequalities is required, moving forward in the analysis of inequity underlying these indicators in Colombia, a country that has a childhood policy and prioritizes the right to comprehensive development since gestation, especially during early childhood.26 The relevance of ensuring this right in the first stage of life becomes not only an essential strategy to fight poverty and the vicious circle producing it, but also a strategy for the human and social development of a country, as it helps improve living conditions.27
In conclusion, the dental caries indicators shows a skewed distribution of the disease in children under six years of age in the municipality of Andes, and a greater inequality in terms of experience of dental caries in its most severe form, based on the analysis of the Lorenz curve and the Gini coefficient.

