











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
In recent decades, providing patients with increased safety during the provision of healthcare services has become a challenge for public and private health service providers and for higher education institutions devoted to the preparation of practitioners.1 Patient safety and healthcare quality are key aspects in the search for universal and comprehensive health coverage.2 International institutions like the World Health Organization (WHO) have considered this aspect, placing it as a key item on the political agenda. Thus, in 2004 the WHO proposed the World Alliance for Patient Safety, which promotes awareness and political commitment to improve healthcare security and supports state members in formulating policies and practices in patient safety.3
Colombia in particular has issued the Patient Safety Policy, closely connected to the components of the Enforced Health Quality Assurance System (Sistema Obligatorio de Garantía de la Calidad en Salud, SOGCS).4 In addition, we have technical guidelines known as “Best practices in patient safety and health care provision”, with technical recommendations to be implemented by healthcare providers in their processes. Another important component is the Observatory on Healthcare Quality, which has recently been improved. It is therefore important to search for mechanisms to enable the epidemiological surveillance of actions or events that may potentially impact healthcare quality and patient safety.5
Patient safety-related issues have been thoroughly investigated in hospital settings, using the IBEAS study as reference. The IBEAS study was carried out in 58 Ibero-American institutions with a population over 11,000 patients, with the intention of characterizing the prevalence and incidence of lesions and/or harm caused to patients during the processes of healthcare provision.6,7 In the dental field, in recent years there has been a growing interest in analyzing the frequency and factors associated with the reporting of adverse events in public and private oral health services8-16 (it should be noted, however, that the reporting of these events in our field is lower compared to other medical areas).11,12 The efforts should then be focused on research in order to approach the problem in epidemiological terms and to identify actions related to the culture of patient safety from different methodologies.
The first efforts made in Colombia in this field were aimed at analyzing the frequency of unsafe acts in dentistry (including adverse events, incidents, and failures) by means of a research project carried out in 10 institutions devoted to the preparation of dental practitioners.17 This study monitored health services in the period 2015-2016, reporting 817 unsafe acts in dentistry (UAD). 53% of these were classified as healthcare failures, 23% were incidents, and 22% were listed as adverse events. Similarly, significant differences were found (p < 0.0001) in terms of frequency of UAD in the study period, as well as type of UAD, type of institution, practitioner’s education level, and other sociodemographic characteristics.
The Universidad de Antioquia School of Dentistry is an oral-health higher education institution founded in 1932. Working under a teaching-service model,18 the School receives lots of patients from various social and economic strata, thanks to its geographical location and recognition as a public university. These patients are referred from different clinics according to the complexity of their condition and are assisted by undergraduate and graduate students under the supervision of specialized professors. The implementation of quality and safe oral health protocols requires systems to identify unsafe acts, in order to establish strategies not only in the School’s clinics but also in its academic curriculum, in line with the guidelines set for by international strategies such as the WHO Multi-professional Patient Safety Curriculum Guide.1
In consequence, this study aims to characterize unsafe acts in dentistry (UAD) using several variables in a public teaching-service institution in the city of Medellín, in the period 2015-2017.
MATERIALS AND METHODS
A longitudinal descriptive study was conducted at the Universidad de Antioquia School of Dentistry. The unit of analysis were all the UADs reported in patients being helped at the institution. This study is part of a multicenter project carried out in 10 dental schools in the country with a 2-year follow-up, but for this article in particular the observation period was extended to October of 2017.17
An online notification system was implemented for data collection by means of the Google Docs™ tool (https://goo.gl/forms/ytkvfJ5Watq2Krv92), complying with the conditions of confidentiality and anonymity of the individuals who filed the reports and the patients involved in the unsafe healthcare situations. Two of the researchers (MTH, DAGA) conducted awareness sessions with the institution staff members, in order to achieve timely and efficient reporting.
The main variable of the study was called Unsafe Acts in Dentistry (UAD), defined as: “actions or omissions that can potentially cause damage or failures in healthcare, or adverse events or behaviors that occur during the healthcare process, usually by action or omission by members of the health team”.5 Other variables were: date of occurrence of the event, type of person to whom the event occurred (administrative, professor, student, practitioner), age and sex of the person to whom it occurred, education level of the person who reported the event, type of clinic, specialty, and sex and age of the patient involved in the UAD.
In order to classify the various types of events that occurred in this period, enough room was left in the report card for staff members to freely and spontaneously narrate the events in their own words. A research team member (DAGA), who is an expert in healthcare quality and patient safety, later interpreted and classified the actions based on the guidelines set for by the Enforced Health Quality Assurance System, defining three categories: 1) Adverse event: the result of a healthcare service that produced unintentional harm. Adverse events can be preventable and non-preventable; 2) Healthcare failure: a deficiency in performing a planned action as scheduled, or the use of an inappropriate plan, which becomes evident by performing incorrect processes (action failure) or by not performing the correct processes (omission failure) during the planning or execution phases. Failures are by definition unintentional; 3) Incident: an event or circumstance occurring during the provision of healthcare service without producing harm but leading to failures in healthcare processes. Of the 547 reports produced during the study period, 541 that could be classified were included in the analysis (99% of the total), and 6 were excluded for not being specific in their definition.5
Data quality control was carried out to observe inconsistencies among the variables collected in the instrument. A database was built in Excel according to the results of the Google Docs™ tool and the data were transferred to IBM® SPSS 21.0 for statistical analysis. A descriptive analysis of the variables was carried out first, using absolute and relative frequencies. The frequency of UADs was described according to the period of occurrence. Then, bivariate analysis of the various UADs was carried out in relation to the variables of the study, calculating chi squared tests of statistical significance to observe the relationship or dependence among them.
The present study complies with the requirements for research in human beings according to the international standards set for by the Declaration of Helsinki19 and Colombia’s legislation, considering Resolution 08430 of the Ministry of Health.20 This is considered a no-risk research project as no investigation was directly conducted in patients, but a properly anonymized secondary data analysis was conducted. This article’s source project was approved by the Committee of Bioethics in Research of the Universidad de Antioquia School of Dentistry by means of Act 05/2015. Finally, it is important to point out that the STROBE guidelines for the reporting of observational studies were taken into account in the preparation of this article.21
RESULTS
During the period from February 2015 to October 2017, 541 UAD reports were observed in the institution. Figure 1 shows the overall occurrence of UADs during the 33 months in which they were reported. In general, there was not an even tendency in the presentation of these events. It should be noted that 65% of the reports were filed in the year 2015. The highest absolute frequencies of UAD occurred during the months of April and July of 2015, August and September of 2016, and August and September of 2017.
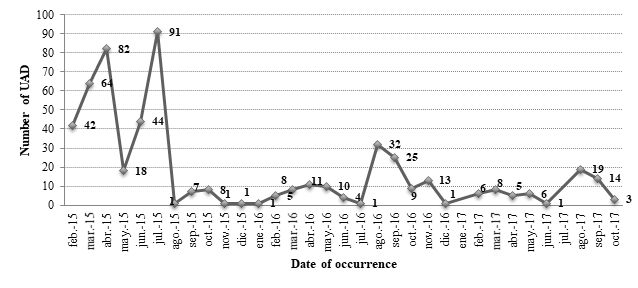
Figure 1 Frequency of unsafe acts in dentistry (UAD) per month-year during the follow-up period in the study population. Medellín, 2015-2017
In relation to the frequency of these UAD according to the month of occurrence and type of clinic (Figure 2), most events in the studied period occurred in the Children’s Clinic (n = 456). Both the Children’s and the Adult’s Clinics showed a marked decrease in UAD frequency in the years 2016 and 2017 compared to 2015. In the case of the Adult’s Clinic, the highest frequencies of UAD occurred in April and July of 2015, and August of 2016. Concerning the Children’s Clinic, the UADs were more frequent during the months of April and July of 2015, August and September of 2016, and August and September of 2017. In general, there were statistically significant differences according to the period of occurrence of these events and type of clinic (p < 0.0001).
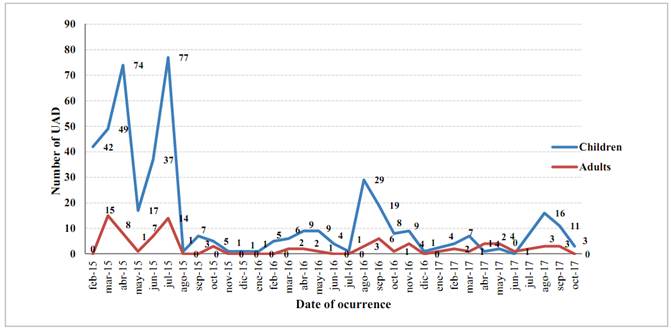
P < 0.0001* * Χ2 Frequency Distribution tests
Figure 2 Frequency of unsafe acts in dentistry (UAD) according to type of clinic and month-year of follow-up in the study population. Medellin, 2015-2017
Table 1 shows the percentage distribution of the UADs considered in the analysis according to their classification and different sociodemographic variables. Adverse events were more frequently reported by administrative personnel, females, staff members aged 34 years or older, as well as in the graduate clinic, in the Adult’s Clinic, in female patients and in persons aged 19 to 44 years. On the other hand, healthcare failures were more frequently reported by students, males, persons under 25 years of age, in the undergraduate clinic, in the Children´s Clinic, and occurred in male patients and in persons over 44 years or under 13 years of age. Finally, incidents were mostly reported by professors, females, persons over 34 years, in the postgraduate clinic, in the Children’s Clinic, and occurred in male patients and in persons 18 years of age or younger. There were significant differences (p < 0.05) between the different types of UAD and the sociodemographic variables included in the analysis.
Table 1 Percentage distribution of unsafe acts in dentistry (UAD) classified according to diverse variables in the study population. Medellín, 2015-2017
| Variables | Total Sample | Adverse event | Healthcare failure | Incident | p-value* | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Person to whom it occurred | ||||||||
| Administrative | 2 | 1 | 50.0 | 1 | 50.0 | 0 | 0.0 | < 0.0001 |
| Professor | 5 | 2 | 4.0 | 0 | 0.0 | 3 | 60.0 | |
| Student | 533 | 20 | 3.8 | 457 | 85.7 | 56 | 10.5 | |
| Professional | 1 | 0 | 0.0 | 1 | 100.0 | 0 | 0.0 | |
| Sex of the person to whom it occurred | ||||||||
| Male | 491 | 14 | 2.9 | 436 | 88.8 | 41 | 8.4 | < 0.0001 |
| Female | 49 | 9 | 18.4 | 22 | 44.9 | 18 | 36.7 | |
| Age of the person to whom it occurred | ||||||||
| ≤ 24 | 482 | 15 | 3.1 | 427 | 88.6 | 40 | 8.3 | < 0.0001 |
| 25-34 | 48 | 5 | 10.4 | 28 | 58.3 | 14 | 31.3 | |
| ≥ 35 | 3 | 1 | 33.3 | 1 | 33.3 | 1 | 33.3 | |
| Level of education of the person to whom it occurred | ||||||||
| Undergraduate | 530 | 21 | 4.0 | 453 | 85.5 | 56 | 10.6 | 0.01 |
| Graduate | 11 | 2 | 18.2 | 6 | 54.5 | 3 | 27.3 | |
| Type of clinic | ||||||||
| Child | 456 | 7 | 1.5 | 398 | 87.3 | 52 | 11.2 | < 0.0001 |
| Adult | 85 | 16 | 18.8 | 61 | 71.8 | 8 | 9.4 | |
| Sex of patient involved in the event | ||||||||
| Male | 505 | 15 | 3.0 | 442 | 87.5 | 48 | 9.5 | < 0.0001 |
| Female | 35 | 8 | 22.9 | 17 | 48.6 | 10 | 28.6 | |
| Age of patient involved in the event | ||||||||
| ≤ 12 | 405 | 6 | 1.5 | 352 | 86.9 | 47 | 11.6 | < 0.0001 |
| 13-18 | 44 | 4 | 9.1 | 35 | 79.5 | 5 | 11.4 | |
| 19-44 | 52 | 9 | 17.3 | 40 | 76.9 | 3 | 5.8 | |
| ≥ 45 | 30 | 3 | 10.0 | 26 | 86.7 | 1 | 3.3 | |
| Total | 541 | 23 | 4.3 | 456 | 84.3 | 59 | 10.9 | ---- |
* Χ2 Frequency Distribution tests
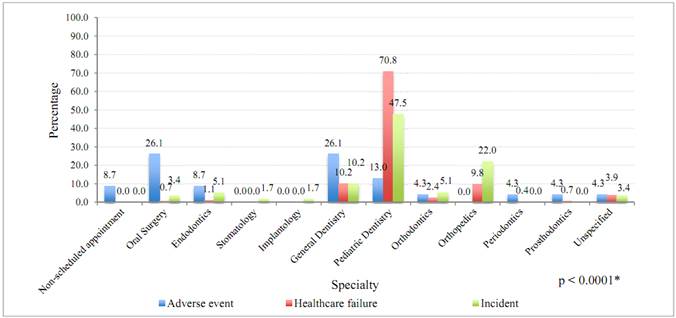
As for UAD frequency per specialty (Figure 3), the relative frequency of healthcare failures was higher in Pediatric Dentistry, while adverse events were more frequent in Oral Surgery and general dentistry. Incidents were more frequent in specialties like Pediatric Dentistry and Orthopedics. There were statistically significant differences in frequency distribution according to type of event and specialty (p < 0.0001).
DISCUSSION
During the follow-up period, 541 UADs were observed in the institution. While a tendency in terms of temporal distribution of these actions could not be observed, they occurred more frequently in the year 2015, with statistically significant differences between type of clinic (Children's or Adult's) and period of occurrence -as well as between the different types of UAD and the sociodemographic variables included in the analysis. To the best of our knowledge, this is one of the first studies that keeps track of UAD reporting in an institution devoted to the preparation of health practitioners with a high impact in the city and the country.
While a steady tendency was not found in the reporting of UADs in each follow-up month, the results show that a higher frequency of these UADs occurred during the year 2015, as well as in some specific periods of the years 2016 and 2017. This is influenced by factors related to the calendar of the institution’s clinical activities, and distinctive conditions of the geographical and social context of the population served. It would be important for future studies to inquire into the academic conditions among undergraduate and graduate students that can influence the reporting of these acts, or how patients, professors, administrative staff and others interact in view of the awareness-raising and training initiatives related to the reporting of patient safety events.
Most UAD reports were filed by undergraduate students, mainly in relation to healthcare failures. These results are consistent with a study conducted in 10 institutions in the country,17 but somehow differ from those reported in a study at a private university in Bogotá, Colombia,10 in which 34.8% of adverse events were reported by undergraduate students. Should be noted that there might be some differences in terms of UAD classification, since the latter study does include other types of events (such as failures and incidents). This can be explained by factors like the students’ lack of experience in patient care, some limited skills, and even lack of supervision, as concluded in other studies.22,23 It is also important to note that most UADs were reported by individuals under 24 years of age -a factor associated to academic and professional experience.
Similarly, most UAD reports occurred in the Children's Clinic, especially in the population of 12 years of age or less and in related clinical specialties such as Pediatric Dentistry, Maxillary Orthopedics, and Orthodontics. Several factors may be involved. On the one hand is the anxiety experienced by children during dental consultation, which can somehow affect the procedures. A systematic review found that the duration of treatment may influence dental anxiety, as well as other characteristics such as the type, complexity, and duration of the procedure.24 On the other hand, the practitioner’s appearance plays an important role in the frequency of dental anxiety and phobia, as shown by a study conducted in Turkey.25 It should be noted that, in recent years, professors have insisted on the practice of reporting these potentially unsafe acts as part of the preparation of students in the Children's Clinic of the institution.
A considerable number of adverse events occurred in the specialty of Oral Surgery. A study conducted in Argentina found that 49% of reports of these events in public and private settings occurred in this specialty,9 many of them by inaccurate planning or inadequate management of technique. Another study with information from the graduate clinics of Pathology and Oral Surgery at a university in Bogotá, Colombia,26 found a proportion of 7% of events listed as unfavorable. It is important for future analyses to make more detailed descriptions of the events, as well as possible causes and their corresponding managements.
The reporting of UAD in the specialty of Endodontics at the Universidad de Antioquia School of Dentistry was low (less than 10%). These results differ from those reported in the national study, which found 14% of UAD in the specialty of Endodontics (almost half of these cases were adverse events).17 Another study conducted in Bogotá10 found a proportion of 6.9% of adverse events in this specialty. A study in Argentina9 discovered a proportion of adverse events of 25%. However, a follow-up study of patients treated during the period 2007-2008 in an Endodontics graduate program in Bogotá15 found a much larger proportion of adverse events (more than 70%). The international literature identifies some specific related events, such as the accidental swallowing of endodontic elements when a rubber dam is not used,27 aspects related to re-treatment, fractures, pain, or treatments performed with inadequate techniques,28 breaks of endodontic instruments,29 or accidents with irrigators such as sodium hypochlorite.30 Deepening the understanding of aspects related to risk management in this specialty and offering the best alternatives is a priority to improve healthcare quality. It is also advisable to investigate if the low frequency of reports in the institution is due to underreporting or other underlying characteristics related to reporting practices.
As strengths of the present study, it is important to note that a properly standardized data collection instrument was used in accordance with the guidelines set for by the Health Quality Assurance System and its adaptation to the dental field. The analysis of UADs allowed to broaden the concept, as many studies take adverse events as the only unit of analysis. Quality was assured by means of information gathered by patient safety experts and the analysis of variables, especially in terms of UAD classification, which was done by reading each report, trying to avoid biases resulting from a wrong classification.
As limitations, we did not include additional variables such as characteristics of the healthcare services, classification of the severity of the events, possible causes of UADs, and aspects dealing with the approach and the response time of the institution in the presence of incidents, events, or failures. Although the culture of UAD reporting has been increasing in our School, it is not possible to control underreporting at 100%. However, underreporting is presumed to be very low, considering the different awareness strategies implemented in the institution-which can be corroborated by auditing the clinical histories. Similarly, it is important to clarify that this article only provides an initial characterization of UADs as a unit of analysis and that it has not been possible to calculate proportions and incidence rates on the total events that occurred in the institution according to the follow-up period and stratification by other variables. It is also important to note that the unit of analysis was the reports themselves instead of the patients; therefore, it is difficult to establish, according to the variables included in the data collection instrument, if several events occurred to a same patient.
Additional studies involving more follow-up time are required, including other health institutions in the public and private sectors. It is also necessary to validate data collection instruments on aspects related to safety in the dental field, and to incorporate qualitative approaches in order to identify the patient safety understandings among health service providers, students, and assistant technical personnel in training, as well as the institutions’ administrative personnel and patients..
The results of the present study validate the need for integrated systems for UAD reporting, incorporating new variables in the analysis. This suggests that any notification model should consider a converging route to homogenize the reporting mechanisms with a number of common variables to standardize the procedures in order to improve healthcare quality and therefore the quality of education. As an example, we have the Minimal Information Model for Patient Safety (MIM PS), a joint project of the European Union (EU) and the World Health Organization (WHO) funded by the European Commission (Directorate-General for Health and Food Safety, DG-SANTE). Also, the models must contain records with patient information, such as sex and age, date of occurrence, person involved, location, cause(s), type of situation, effect of the situation, resulting action(s), and safety barriers.31

