











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Universal Health Coverage (UHC) is part of the global development agenda, particularly within the health and wellness areas of the Sustainable Development Goals.1,2 UHC refers in particular to universal access to health services and medicines as needed, with quality and equity, as well as protection against financial hardship caused by disease3 Although oral health (OH) or dental services are not explicitly mentioned within UHC, health systems must ensure at least basic services for all and care to priority groups such as mothers, children, and patients with chronic diseases such as HIV/AIDS and diabetes.4,5
Colombia is approaching universal coverage, with 95% of the population covered by the social health security system and a 15% out-of-pocket expense for health spending, which results in good financial protection.6 Health Maintenance Organizations (HMOs)** are responsible for enrolling the population; they receive per capita income (PCI) and must have a network of providers to provide care to their members under the Health Benefits Plan (plan de beneficios en salud, here on PBS).7 In terms of OH, this plan includes a wide range of services, from general and specialized dental consultation, operating procedures, maxillofacial surgery and endodontics, to oral rehabilitation with full muco-supported prostheses. According to the classification of health procedures, the OH services to which the affiliated population is entitled to correspond to 89% of the services available in the country, although the technologies used may be lower than those offered on the market.
However, despite promises and achievements in coverage, the Colombian population still face difficulties especially for access to health services. The 2015 National Health Care Quality Report found that 46% of users found it difficult to access the services of their HMO.8 For dental services, care coverage is estimated to be low,9 although according to the 2017 National Quality of Life Survey 55.6% of people consult the dentist for prevention at least once a year, suggesting that a substantial part of services are requested outside the system, with private pay. Some publications show that access barriers may be of various nature, including economic and geographical accessibility issues, the population’s lack of knowledge of their rights, and the perception of not needing health care.10
Concerning the resources to finance OH coverage, while at the start of the system in 1995 it was decided to allocate 17.5% of the PCI to “basic oral health”,11 subsequent analyses found lower expenditure,12,13 and financial adequacy studies on PCI show that this percentage could be as low as 4% in 2017.14
An illustration of what can happen to the dental services run by HMOs, especially in large cities, can be seen in the problems uncovered by those who participated in the formulation of the 2013-2022 Medellin Public Oral Health Policy, who pointed out the lack of a frame of reference to understand OH and to address it from a holistic perspective; they also point out that the resources allocated to meet the needs are insufficient, as shown by supply shortages and low coverage.14 The data offered by the twelve providers participating in this policy show that less than 20% of the population access dental care in HMOs.15
In this context, the aim is to analyze the coverage of OH services in the Medellin population who use HMOs using information from the year 2015, analyzing the factors that could explain coverage levels. This study seeks to establish expected coverage based on regulatory criteria and the need arising from the epidemiological profile, in contrast to actual coverage or use of services. This helped identify gaps in the scope of HMOs’ services to meet the needs of their patients.
METHOD
A mixed study with a central quantitative component and a complementary qualitative component was conducted for the city of Medellin, Colombia’s second largest city with 2.6 million people in 2018 and 96% health insurance coverage. The reference population were users of the health system who in 2015 accessed dental services in the city’s HMO network. The population was analyzed according to the stages of life defined in Resolution 3280 of 2018 by the Ministry of Health and Social Protection: early childhood, childhood, adolescence, youth, adulthood, and old age.
Sources of information
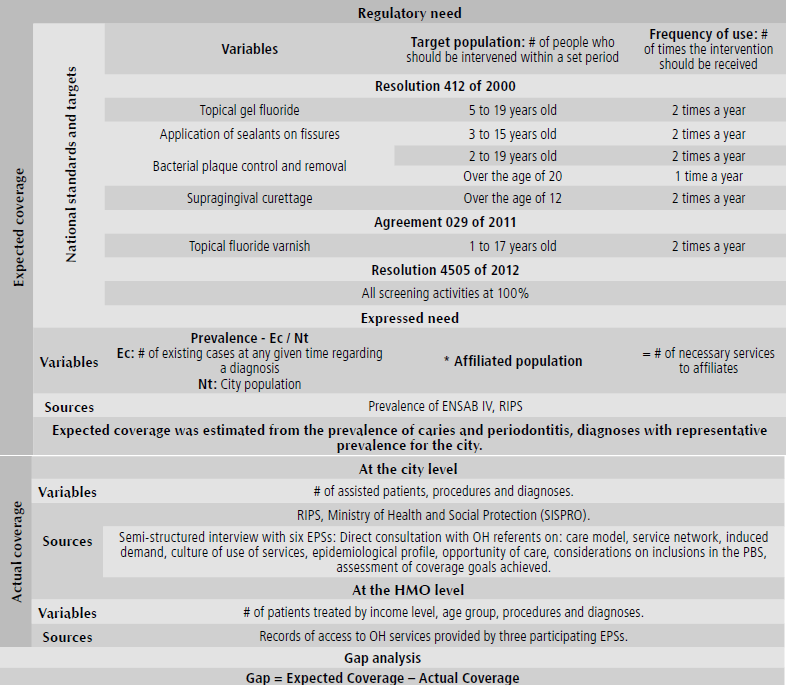
The study included the city’s six main HMOs, which account for 92.2% of the affiliated population. Quantitative information used epidemiological data from the IV National Oral Health Study (IV Estudio Nacional de Salud Bucal, ENSAB IV),16 the HMOs’ individual service records (registros individuales de prestación de servicios, RIPS), and records provided directly and confidentially by three of the six HMOs in the study (Table 1). The analysis considered the following variables: prevalence of major oral diseases (caries and periodontal disease), the total number of people served and number of services provided, age group, income level, and diagnoses for caries and periodontal disease.
The qualitative information came from a semi-structured interview with OH referents from the six HMOs, including regional leaders, auditors, coordinators, and dental area directors. The purpose of the interview, developed after an informed consent, was to hear contributors about aspects related to coverage and access to services (Table 1).
Processing and analysis
Expected coverage was calculated, first from national standards on specific protection and early detection, and then as the fraction of the affiliated population who could use dental services, based on caries and periodontal disease prevalence rates reported in ENSAB IV. Actual coverage was assumed as the proportion of patients who actually accessed HMO services, calculating the gaps between the two indicators (Table 1).
Qualitative information was subjected to content analysis, taking into account the categories previously defined by the researchers.
The present study complies with the requirements for research in human beings according to the international standards and Colombia’s legislation, considering Resolution 08430 of the Ministry of Health. This is considered a no-risk research project.
RESULTS
Expected coverage
Expected coverage from regulatory need
Table 2 shows the number of specific protection and early detection activities to be carried out in 2015 among the affiliated population of Medellin (2,515,509) to comply with Resolution 412 of 2000. This standard contains the national guideline on promotion and prevention activities in OH to be carried out by HMOs classified by age groups, so some users require several actions simultaneously.
Table 2 Medellin: Expected coverage in specific OH protection and early detection actions, 2015
| Activities | Target population | Number of users | Frequency of use a year | # Activities |
|---|---|---|---|---|
| Topical fluoride application | (5-19 years) | 521,066 | 2 | 1,042,132 |
| Fluoride varnish application | (0-5 years) | 147,701 | 2 | 295,402 |
| Sealants application | (3-15 years) | 411,799 | 2 | 823,598 |
| Bacterial plaque control | (2-19 years old) | 597,732 | 2 | 1,195,464 |
| Bacterial plaque control | (20 years and older) | 1,873,617 | 1 | 1,873,617 |
| Supragingival curettage | (12 years and older) | 2,174,620 | 2 | 4,349,240 |
| Total specific protection and early detection activities | 9,579,453 | |||
Source: Resolution 412 of 2000 (modified by Resolution 4505/12) and SISPRO
Expected coverage from expressed need
Table 3 shows the estimate of the affiliated population that had to be served in 2015 for caries and periodontitis care, according to the prevalence rates in ENSAB IV, which are lower in the Medellin population compared to the national average. According to ENSAB IV, 24.3% of the city’s children aged 1,3 and 5 years had some prevalence of deciduous teeth cavities, compared to 33.8% nationally. For children 5 to 12 years of age, the prevalence in Medellin was 36.6% in mixed dentition, while for the population of 12, 15, 18 and 20 to 79 years this indicator was 28.9% in permanent dentition. These figures amounted in the country to 47.1% and 55.8%, respectively. In terms of periodontitis in the population over 18 years of age, ENSAB IV reported a city prevalence of 40.5% in its different degrees of severity, which places Medellin well below the national figure of 61.8%.
Table 3 Medellin: Expected coverage for caries and periodontitis care, 2015 (Population to be treated according to diagnosis and dentition type)
| Description of prevalence | Affiliated population | Prevalence (%) | Population to be served |
|---|---|---|---|
| Caries | |||
| Prevalence of caries in primary dentition* | 128,524 | 24.28 | 31,206 |
| Prevalence of caries in mixed dentition** | 253,539 | 36.60 | 92,795 |
| Prevalence of caries in permanent dentition*** | 2,115,432 | 28.94 | 612,206 |
| Periodontitis | |||
| Periodontitis from 18 to 79 years of age | 1,898,388 | 40.53 | 769,417 |
| Total people | 1,505,624 |
Source: ENSAB IV prevalence: * Temporal dentition: Reference population: 1, 3 and 5 years, ** Mixed dentition: Reference population: 5 and 12 years, and *** Permanent teething: Reference population: 12, 15, 18, 20 to 79 years. Periodontitis: includes mild, moderate, and severe classifications of the disease
Services or actions to the target population
Caries services
For patients diagnosed with caries, 3,430,754 health services were required, of which 81.6% (2,800,842) should target the population with permanent dentition (>12 years), 12.5% (430,477) patients with mixed dentition, and 5.9% (199,435) the primary dentition population. Table 4 lists the weighter and services needed for the population by type of dentition, with first-time consultation by general dentistry being the input. The weighter used in this estimate reflects the likelihood for a patient to receive a certain type of treatment given their diagnosis of either caries or periodontitis and depending on their age group.
Table 4 Medellin: Estimation of the OH procedures needed to address the prevalence of caries and periodontitis, 2015
| Services and procedures | Caries | Periodontitis | ||||||
|---|---|---|---|---|---|---|---|---|
| Temporary dentition˟ | Mixed dentition˟˟ | Permanent dentition˟˟˟ | 18 to 79 years old | |||||
| Weighter* | Total activities | Weighter* | Total activities | Weighter* | Total activities | Weighter* | Total activities | |
| First-time consultation for general dentistry | 1.00 | 31,206 | 1.00 | 92,795 | 1.00 | 612,206 | 1.00 | 769,417 |
| Dental sealing by surface, with amalgamation | 0.19 | 5,773 | 0.20 | 18,559 | 0.21 | 129,788 | 0.07 | 53,859 |
| Supragingival curettage | - | - | 0.02 | 1,392 | 1.00 | 612,206 | 1.00 | 769,417 |
| Dental plaque control ncoc | 1.00 | 31,206 | 1.00 | 92,795 | 1.00 | 612,206 | 1.00 | 769,417 |
| Dental sealing by surface, with photocuring resin | 0.11 | 3,464 | 0.06 | 5,289 | 0.12 | 74,689 | 0.04 | 30,777 |
| Individual health education, by dentistry | 1.00 | 31,206 | 1.00 | 92,795 | 1.00 | 612,206 | 1.00 | 769,417 |
| Topical gel fluoride | 1.00 | 31,206 | 0.22 | 20,322 | 0.04 | 22,039 | 0.02 | 15,388 |
| Millimeter periapical intraoral x-rays | 0.02 | 530 | 0.03 | 3,062 | 0.07 | 41,018 | 0.02 | 15,388 |
| Extraction of permanent multiradicular teeth | - | - | - | - | 0.03 | 18,978 | 0.02 | 15,388 |
| Unirradicular surgical extraction | - | - | - | - | 0.02 | 12,244 | 0.02 | 15,388 |
| Incisal angle reconstruction, with photocuring resin | 0.02 | 499 | - | - | 0.02 | 9,795 | 0.01 | 7,694 |
| Photocuring sealant application | 1.00 | 31,206 | 1.00 | 92,795 | - | - | - | - |
| Application of preventive resin | 0.01 | 437 | 0.03 | 2,505 | - | - | 0.01 | 7,694 |
| Topical varnish fluoride | 1.00 | 31,206 | - | - | - | - | - | - |
| Extraction of temporary teeth sod | - | - | 0.02 | 1,670 | - | - | - | - |
| Other services | 0.05 | 1,498 | 0.07 | 6,496 | 0.07 | 43,467 | 0.10 | 76,942 |
| Total | 199,435 | 430,477 | 2,800,842 | 3,316,186 |
*Weighter: Corresponds to the probability of performing each service (caries by type of teething and periodontitis)
**Activity frequency: Corresponds to the average of the activity
˟ Temporal dentition: Reference population: 1, 3 and 5 years
˟˟ Mixed dentition: Reference population: 5 and 12 years
˟˟˟ Permanent dentition: Reference population: 12, 15, 18, 20 to 79 years.
Source: Ministry of Health and Social Protection, Resolution 412 of 2000
Periodontitis services
To address periodontitis, it was necessary to provide 3,316,186 services, including first-time consultation services, supragingival curettage, dental plaque control and individual health education by dentist (Table 4).
Approach to city coverage
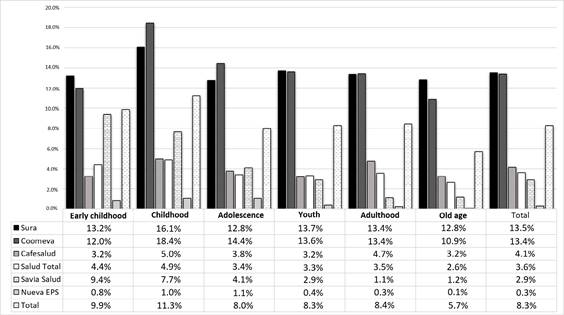
According to the individual service records (RIPS) reported by the HMOs to the Ministry of Health and Social Protection, 266,512 people would have used some OH service in Medellin in 2015, indicating a coverage of 10.6% compared to the total number of users. This coverage ranged from 7.4% for the old age group population to 14.1% for children. For other population groups, the coverage was like this: adolescence (9.6%), youth (10.5%), adulthood (10.9%) and early childhood (13.1%).
In terms of HMO coverage, taking into account the number of patients cared for and registered users, Coomeva (22.0%) and Sura (17.4%) have the highest overall coverages. By age groups, early childhood and childhood concentrate the highest coverage levels. In terms of first-time consultation coverage, there are records of 191,556 users, indicating coverage of 8.3%. Sura and Coomeva remain the HMOs with the most coverage (Figure 1).
Coverage in three HMOs, 2015 and 2016: case analysis
With the information collected from three HMOs participating in the study, coverage was estimated in first-time consultation, classified by age group. A coverage concentration was found in early childhood (0 to 5 years) and childhood (6 to 11 years), reaching an average percentage of 28%, which is above the average coverage in the total population. Also, coverage decreases as age increases, so that segments of adults and older adults registered the lowest percentages of dental appointment attendance. For these groups, first-time consultation ranges between 15.9% and 22.7%, which is considered low in view of regulations and public policy.
As for coverage per users’ income, two HMOs from which this information was obtained show a negative relationship between the two variables, with remarkably similar results. Among the low-income population (less than two minimum wages), first-time consultation coverage was 22.6% and 23.6% in the two HMOs, among the middle-income population (2 to 5 minimum wages) this value was 21.6% to 19.7%, and among the high-income population (more than 5 minimum wages) it was 13.7% and 13.6%.
Care gaps
Taking into account that expected coverage, according to regulations, consider about 12 million specific protection and early detection activities that includes 2.9 million dental care consultations, and according to the records of service provision reviewed in this study, only 3.8% of the activities would have been carried out, which means a gap of more than 11 million activities that were note done by the HMOs.
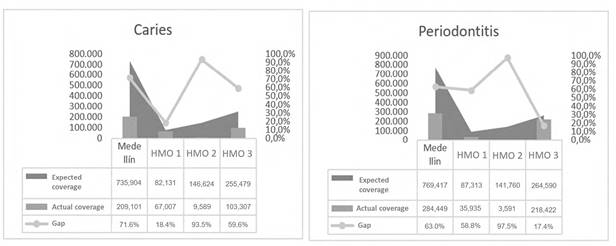
The gap in caries and periodontitis care, according to expected coverage, would be 526,000 services for caries and 485,000 for periodontitis. The results of the HMOs that contributed the most information to the study stand out, since the care gap is only 18.4% for caries in HMO 1 and 17.4% for periodontitis in HMO 3. Similarly, the results for HMO 2 are noteworthy, as the gap between expected and actual care exceeds 90% in the two evaluated pathologies (Figure 2).
Coverage from the perspective of HMOs
In the interviews with OH referents from the six HMOs in the study, they conclude that the main diseases among the affiliated population in Medellin are caries, gingivitis, and periodontal disease. Some consider that the Health Benefits Plan (plan de beneficios en salud, hereon PBS) is generous and offers the required care, and in general has increased in recent years without adequate funding: “Inclusions in the benefit plan have increased (total prosthesis, fluoride varnish), without an adequate increase in PCI to ensure coverage and funding for these treatments” (interview at HMO 6).
Concerning coverage of the affiliated population, the HMOs admit that it is low to medium compared to the goals set by policies and regulations. They also recognize that low levels of coverage account for the users’ perception of the service, as such services are basically sought for curative purposes, but much of the demand is also assisted through private services: “Dental services are primarily sought as a curative (pain relief) instead of a preventive approach” (interview at HMO 5); “Coverage is low because we know that much of our population consult privately” (interview at HMO 2).
In general, all HMOs develop programs aimed at prioritized groups such as mothers, early childhood, diabetics, or hypertensive. In these population segments, coverage indicators exceed the population average. However, the interviews expose the difficulties faced by both insurers and providers in attracting healthy adult populations, which in their words is due to several reasons, ranging from the users’ perception of low-quality services included in the PBS, to insurers’ financial difficulties in providing care to all their users while complying with current regulations.
The HMOs recognize the need to strengthen induced demand strategies for greater coverage, while it is also key to increase resources for such strategies, improving the quality of information circulating between HMOs and IPSs (institutions providers of health services).
DISCUSSION
While Colombia’s PBS is an instrument for universal health coverage, access or actual coverage in terms of HMO’s dental services in a city like Medellin is very low, as stated in other estimates.9 This study exposes this low coverage in terms of both preventive services and care of the two main pathologies affecting the population.
Based on the coverage offered in the PBS and considering the city’s epidemiological profile as well as the goals on specific protection, expected coverage should be connected to the volume of services required by the population. By 2015 it would have been necessary to carry out around 12 million activities to achieve universal coverage in different population groups, including application of topical fluoride, sealants, bacterial plaque control and curettages. In addition, taking into account caries and periodontitis prevalence, it would have been necessary to conduct about 7 million actions to treat these pathologies.
While these figures can be very ambitious and it might be accepted that coverage analysis should not be limited to one-year only, but instead expand to a two-to-three-year period in order to cover a larger number of people in that period to improve OH levels, the information available shows that the population who seek OH services provided by the HMOs does not reach 30% in a year, and the proportion could be as low as 10%.
The studies that focus on the assessment or description of access to oral health services get to relatively homogeneous conclusions, implying that the entry level and the existence of health insurance are the main facilitators, while recognizing other user intrinsic factors, such as the perception of not requiring the service, the fear of procedures, or being unaware of the rights as insurance beneficiaries.20,23 So, according to such studies, access to oral health services is not always limited by economic barriers; it is also important to take into account the perception of users and the personal reasons that block the use of services. This situation highlights the three determinants of health services demand, in particular the preventive ones: I know, I want, I can.23 These three factors, specifically in the field of OH, may be more influential than others such as infrastructure, geographical location, economic constraints or out-of-pocket spending.
For instance, the study by Franco et al10 identifies barriers to accessing dental services by children under the age of 6 in a vulnerable population in Medellin. The study used a structured survey aimed at mothers or caregivers, inquiring about categories such as predisposition to consultation, perception of care needs, and satisfaction with provided services. The results indicate that while 97.5% of the assessed population is affiliated, there are access barriers that are not necessarily linked to economic reasons or geographic location, but to information issues (92% of mothers were totally or partially unaware of care rights), or perceived needs (only a low number of mothers perceived oral problems in their children as requiring care).
It is important to note that real coverage indicators may be higher when one considers that data are underreported and that many people rely on private services. However, the HMOs recognize that coverage is low, citing reason like lack of information and need perception, as pointed out in the literature. It is generally accepted that more effective actions are needed to expand coverage.
An important section has to do with demand for services and its determinants, something that should be further analyzed. The information obtained in this study, at least for two HMOs, suggests that the demand for basic care is inversely proportional to income level, i.e. the population segment with higher income levels tend to meet their needs outside the PBS. Estimating the determinants of demand for oral health services is suggested as a future research topic.
One of the limitations of the present study has to do with the source of information for caries and periodontitis prevalence, which is necessary to estimate expected coverage. The data were taken from ENSAB IV, which contains representative information at the national level but not at the municipal level, as patients surveyed in Medellin do not represent a statistically significant number to reflect the oral health conditions of the entire population. Therefore, the number of oral health services expected to be conducted for caries and periodontitis could be overestimated, as the prevalence of these health conditions in the city tends to be lower than those reported in the rest of the country.
Although only quantitative information was provided by three of the six HMOs contacted for this study, this did not affect the obtained results or their validity, since these data only served to carry out a case analysis to contrast the coverage obtained through RIPS, and the perceptions collected in the qualitative analysis.
Limitations regarding quality of the data used for analysis should also be mentioned. It is necessary to strengthen information systems at the national and local levels, requiring providers and insurers to offer complete and truthful information, as decision-makers should have reliable tools to build health policies and estimate the sector’s resources. While the information contained in RIPS is perceived as low quality, they must essentially contain basic data required by the system as support for payment of benefits and to direct regulatory and control processes.
In conclusion, as was evident in the case of Medellin, there are low levels of dental services coverage-which in Colombia is part of the benefits plan and must be guaranteed by the HMOs-. The gap between need and care is particularly high in prevention services, so compliance with regulatory goals is far from ideal. In addition to reviewing and weighing the applicability and feasibility of these goals, it is important to provide users with more information and induced demand strategies, and to allocate additional resources, monitoring HMOs closely.

