











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
The long-term stability of orthodontic treatment is one of the objectives of orthodontists. This implies maintaining the results of the mechanical actions performed on teeth and effectively controlling the reaction to the movements performed by the periodontal ligament and muscles, among other factors, until achieving a balance of forces that maintains the occlusal characteristics that initially triggered the corrective treatment.1
In orthodontic terms, relapse can be defined as a retrogression towards the starting position in any direction once the orthodontic retention appliance is removed. This is due in part to the recovery of the previous muscle balance which fails to adapt to the dental arches shape or cannot oppose the reaction of periodontal fibers. At the end of orthodontic treatment, the operational action is installed on the relapse-retention pair, understood as the use of the appropriate mechanism to maintain the results achieved during the treatment period and preventing recurrence.1
The literature has covered topics such as the answers to the need for correct interventions and with the right appliance, and malocclusion type once it has been corrected; other studies focus on the duration of retention, how it should be applied, the best adaptation system for patients, and more recently molecular and pharmacological approaches, in addition to the use of removable, fixed, and surgical techniques such as supracrestal fiberotomy.2
Some studies retrieve general information to improve clinicians’ knowledge.3 In contrast, others try to collect the type of retention procedures used by orthodontic professionals in some countries. Such is the case of Padmos, Fudalej, and Renkeman,4 who used questionnaires to collect information on this issue from 306 specialists. However, this was done by retrieving evidence through systematic reviews.5,6 Few documents analyze the use and importance of produced information and the relationships among research projects on this topic.
Reviews usually provide specific content quality information. Wasserman et al7 show the periodontal effects of long-term retainers but fail to consider the scale of research and the possible scope of academy in the study of the relapse-retention couple. Another example is Gómez et al8, who state that it is not possible to determine the type of fixed retainers that may be best in their systematic review of post-orthodontic retention in patients aged 12 to 35, by comparing two types of fixed retention. This shows that the available information on this topic is unclear, and therefore a review is required to indicate the scope and map the analyses.
This means that obtaining information from research niches and analyzing the most relevant articles is useful not only for clinicians but also for editors and researchers, as they can obtain a panoramic view with an additional perspective, not provided by other types of data collection.9 The objective of this review is to map the issues related to relapse and retention, as well as some relevant aspects related to research gaps and academic production from the articles retrieved on this topic.
METHODS
Research type
This was a review of the available research evidence (scoping review) coupled with some bibliometric indicators obtained from articles in Web of Science Core Collection.10
Procedure
In order to comply with the panoramic exploration and to add some bibliometric indicators to retrieve information, a few methodological processes for data collection were combined, in strict compliance with the structure of the review. To that end, the following steps were taken: a) question formulation, b) search for publications, c) identification of studies, d) systematization and data extraction, e) analysis and report of final results.11 For the selection of publications to be reviewed, bibliometric citation information and keyword analysis were used for two individual searches. The files were saved in plain text and exported to Excel 2016 to conduct both article selection and analysis.
A total of 1,263 documents were found, excluding those not directly related to the subject of this review, as well as those not cited, for a final list of 120 articles, selecting the ones to be included in the analysis through two mechanisms: a group discussion by the members of the study, who used a ten-point scale to previously and individually grade the relevance of each article based on GRADE recommendations (the Grading of Recommendations Assessment, Development and Evaluation).1This procedure yielded 60 articles that were reviewed by two external orthodontists experts in the subject, for a final selection of the 31 most relevant documents. Bibliometric data were run through the VOSviewer 1.6.14 software to present citations and authors, as well as the frequency of terms in titles and abstracts only.12 This free software helps analyze and visualize the relationships and patterns produced when relating the available information from bibliometric data.13
Articles were searched in Clarivate Analytics’ Web of Science (WoS) database14 on April 10, 2020. Two separate searches were performed using the terms “relapse” and “retention” in combination with the Orthodont* keyword using the Boolean operator AND. Various keyword combinations were tested until finding those that allowed the retrieval of the largest number of articles.
The search included reviews and full articles in English for the period 2010-2019, using the search algorithm in topics, titles, and keywords for “Dentistry Oral Surgery Medicine” and for all types of documents: scientific articles, reviews, editorials, letters, etc. included in the database. The “relapse and orthodontics” combination yielded 518 articles and the “retention and orthodontics” combination yielded 745 articles.
RESULTS
Analysis of citations regarding publications
The “relapse and orthodontics” combination yielded 518 articles. Of these, 111 (21.4%) have not been cited; 148 (58.6%) were cited at least 10 times, 52 publications (10.0%) have been cited at least 20 times, and 9 articles (1.73%) have been cited more than 50 times.
The “retention and orthodontics” combination yielded 745 articles. Of these, 164 (22.0%) have not been cited; 172 (23.0%) were cited at least 10 times; 61 publications (8.2%) have been cited at least 20 times and only 5 articles (6.7%) have been cited more than 50 times.
The article “Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth”17 appears as the most cited in relation to both topics, with 67 citations. And “Long-term effectiveness of canine-to- canine bonded flexible spiral wire lingual retainers”21 has 53 citations in both topics, but in different positions; it ranks fourth in the “retention and orthodontics” list and eighth in the “relapse and orthodontics” list. The most cited article in the first group has 79 citations and the least cited has 49 citations; in the second group, the most cited article has 78 citations and the least cited has 43 citations (Table 1).
Table 1 Most cited articles on the topic “relapse and retention in orthodontics”
| Most cited documents on relapse and orthodontics | Main author and year - relapse and orthodontics | Citations | Most cited documents on retention and orthodontics | Main author and year - retention and orthodontics | Citations |
|---|---|---|---|---|---|
| Stability of treatment for anterior open-bite malocclusion: A meta-analysis15 | Greenlee (2011) | 79 | White-spot lesions during multibracket appliance treatment: A challenge for clinical excellence16 | Enaia (2011) | 78 |
| Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth17 | Baek (2010) | 67 | Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth17 | Baek (2010) | 67 |
| Comparison of Progressive Cephalometric Changes and Postsurgical Stability of Skeletal Class III Correction With and Without Presurgical Orthodontic Treatment18 | Ko (2011) | 57 | Results of a survey-based study to identify common retention practices in the United States19 | Valiathan (2010) | 56 |
| Progressive condylar resorption after mandibular advancement20 | Kobayashi (2012) | 55 | Long-term effectiveness of canine-to-canine bonded flexible spiral wire lingual retainers21 | Renkema (2011) | 53 |
| The orthodontic-periodontic interrelationship in integrated treatment challenges: a system- atic review22 | Gkantidis (2010) | 55 | How does orthodontic treatment affect young adults’ oral health-related quality of life?23 | Palomares (2012) | 52 |
Source: by the authors
Analysis of citations regarding authors
There were 1,948 authors associated with publications on “relapse and orthodontics”. The most cited author is Kee-Joon Lee from the Yonsei University’s School of Dentistry in Korea, with 7 publications and 142 citations related to the subject under study. On the other hand, 2,529 authors have publications on “retention and orthodontics”; Christos Katsaros, from the University of Athens, has produced 15 publications linked to 256 citations. None of the first 10 authors share publications on the same topic. The largest number of citations and publications is linked to “retention and orthodontics” (Table 2).
Table 2 Most cited authors for “relapse and retention in orthodontics”
| Most cited authors on relapse and orthodontics | Number of documents per author | Citations | Most cited authors on retention and orthodontics | Number of documents per author | Citations |
|---|---|---|---|---|---|
| Lee, Kee-Joon | 7 | 142 | Katsaros, Christos | 15 | 256 |
| Ko, Ellen Wen-Ching | 4 | 114 | Ruf, Sabine | 12 | 170 |
| Huang, Chiung Shing | 3 | 111 | Pandis, Nikolaos | 13 | 126 |
| Choi, Yoon-Jeong | 3 | 110 | Eliades, Theodore | 10 | 120 |
| Huang, Greg J. | 3 | 106 | Kuroda, Shingo | 12 | 111 |
Source: by the authors
Analysis of co-occurrence on relapse and retention
The words surgery, effect, and retention are the most common within the “relapse and orthodontics” group; on the retention group, the three most used words are retainer, significant difference, and retention period. Both groups show the words retention, expansion, and day, though in different positions and with different occurrences (Table 3).
Table 3 Occurrence of the words “relapse” and “retention” in orthodontics in titles and abstracts
| Words related to relapse and orthodontics | Occurrences | Words related to retention and orthodontics | Occurrences |
|---|---|---|---|
| Surgery | 132 | Retainer | 141 |
| Effect | 106 | Significant difference | 135 |
| Retention | 103 | Retention period | 109 |
| Teeth | 80 | Case | 102 |
| Movement | 77 | Occlusion | 97 |
Source: by the authors
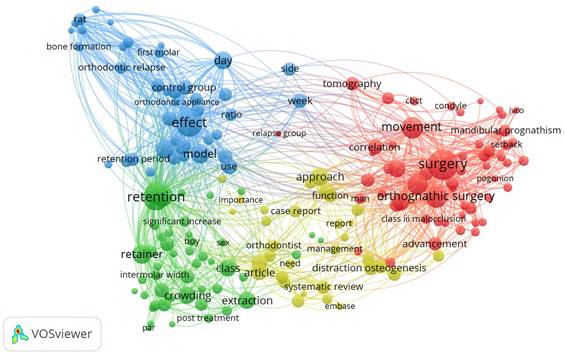
Regarding co-occurrence of terms related to relapse and orthodontics, there were 9,965 terms, 296 of which (3.0%) meet the threshold of appearing at least 10 times; these terms are clustered in four groups. The first group (in red) includes 57 terms, with the following being the most common: surgery, movement, orthognathic surgery, osteotomy, advance, angle, B point, and cephalometric analysis. In a second group (in green), with 49 words reaching the analysis threshold, there were common words such as retention, tooth, device, retainer, extraction, and post-treatment. A third group (in blue) includes 40 items reaching the analysis threshold, such as effect, model, retention period, number, control, proportion, dental movement, bone formation, osteoblast, osteoclast, animal. Finally, the fourth group (in yellow), with 32 terms, includes words like evidence, development, orthodontist, combination, intervention, distraction osteogenesis, and complication. The use of words over time is fuzzy and mixes words from all groups; the articles in recent years usually mention words like evidence, complication, review, retrospective study, and postoperative stability (Figure 1).
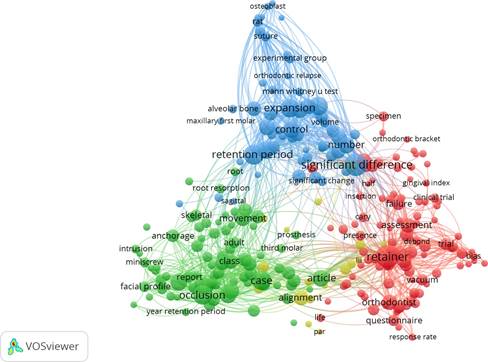
In the case of retention and orthodontics, there were 15,069 terms associated with titles and abstracts. Of these, only 427 (2.8%) meet the threshold of occurring at least 10 times. The results also yield four groups distributed as follows: the first group (in red), with 102 terms, include words like retainer, orthodontist, meta-analysis, review, questionnaire, duration, risk, evaluation, trial, evidence, criteria, and effectiveness; in a second group (in green), with 82 terms that meet the threshold, there are words like case, class, occlusion, growth, correction, long-term stability, relationship, diagnosis, case report, surgery, function, and treatment plan. In a smaller number, there is a third group (in blue) with 55 words like expansion, day, significant difference, retention period, expression, bone, experimental group, control group, parameter, and volume. Finally, the fourth group (in yellow), with 17 terms, includes words like alignment, arch length, intercanine, intermolar width, irregularity index, measurement analysis, pretreatment, post-treatment, significant reduction. At the time of analysis, the words in the red group are the most recently used, while those in the blue group are not recently used (Figure 2).
New and old protocols, research on effectiveness verification, and other proposals
An orthodontic treatment is considered successful if both functional and aesthetic results are maintained over time. Therefore, fixed appliances are preferred as a retention mechanism; protocols are tested in cases where this goal is missed.24 Some fixed mechanisms have been proposed with small modifications such as the addition of an elastic device, which exerts a free inclination force on teeth to correct slight crowding.25 There are recent, more innovative proposals that tend to measure the effectiveness of new protocols with modified devices; such is the case of the study by Armstrong et al, who verified the effectiveness of a magnetic retainer compared to common forms of retention such as adherence to each tooth. To measure efficacy, the researchers used Little’s Irregularity Index, intercanine width, and discrepancy in arch length by tooth size. The study was prospective to two years and found that there were no significant differences between the two forms of retention.26
Tests using controlled and randomized studies are other methods to measure retention under various conditions. They are usually two-year prospective studies. A test of this nature was carried out by Tynelius et al, who verified the retention of three methods in Class I with premolar extractions. The sample consisted of 75 patients aged 14.4 years in average, distributed in groups for all three methods. An analysis of variance showed the retention success in this observation period.24,27
Other studies exploring practical actions in relation to orthodontists’ knowledge, attitudes, and practices concerning retention use questionnaires that are sent through orthodontists associations in each country, such as Lithuania,28 the United States,29 Saudi Arabia,30 Malaysia,31 and the Netherlands,32 asking respondents for information on the selection of retention systems, the details of the most commonly used fixed and removable retainers, the duration of retention periods, the characteristics of follow-ups, and the instructions given to patients. In most cases, retainers are prescribed after meeting treatment targets, and fixed retainers are combined with removable retainers over time, but each system has its preferences when formulated.28,32
In these studies, orthodontists usually prefer the classic Hawley retainer in maxillary, and a proportion that varies within each study chooses the fixed retainer mainly in the lower arch. There is variability in retention duration, ranging from one year to “for life”29 in fixed retainers, or use for 20 hours indefinitely, in removable ones.31
In terms of stability, the study by Bjering et al assesses orthodontic treatment results after cement removal, at the end of clinical treatment, and 3 and 5 years after the end of procedure. The study also evaluates how these results can be influenced by the protocols chosen for retention in anterior teeth, thus becoming a key article for its contributions in this topic review. The research was conducted on a sample of 169 patients during four stages of treatment: pre-treatment T0, post-treatment T1, 3 years post-treatment, and 5 years post-treatment.
As a methodology, they used Peer Assessment Rating, comparing the scores assigned by the evaluators each time. The results showed that the retention protocol apparently did not influence stability at five years, and that anterior mandibular alignment was better with fixed retention compared to the group in which retention was removed three years after treatment.33
Molecular trials in relation to orthodontic retention
A significant number of studies aimed at explaining the molecular mechanisms related to relapse and retention have been conducted for some years. Some of them benefit from the advances on information in this field to propose new possible treatments. Much of the experimentation is done on cell lines and animal models.34
Unlike extractions, which clinically play an important role in orthodontics and relapse,35 the role of bones has been addressed by relatively important studies that increasingly show evidence of the importance of this tissue as a recipient of both critical cells and mediating molecules throughout this process.36 The process has been studied on the periodontal component in animal models; thus, the study by Franzen et al addresses the periodontal factors in treatment relapse after orthodontic dental movements. The study includes a detailed report on the remodeling of alveolar bone and related periodontal structures in rat molars. The findings in this animal model produces information that orthodontic relapse occurs quickly by the action of osteoclasts that act in the remodeling of alveolar bone.37,38
Similarly, since both periodontal ligament and bone play an important role in the response to mechanical strength performed during orthodontic treatments, the study by Feng et al shows that periodontal ligament progenitor cells (stem cells) can efficiently respond to mechanical forces and thus mediate the stability that leads to the recovery of collagen fibers within the ligament to regain its initial state after the force is removed. Feng provides information that relates the signaling of the transforming growth factor beta (TGF-β), as a signaling regulator that can modulate that process.39
In addition to the role of stem cells and the involvement of molecules present in periodontal tissues, other studies help recognize relapse as a complex system of response to the stimulus of orthodontic forces, which goes beyond clinical factors; in this regard, it has been reported that the increase in antioxidant enzymes in which the E2F and NrF2 gene mediates inhibits bone destruction. This implies that reactive oxygen species (ROS) may be mediating osteoclastogenesis processes, and therefore the expression of the NrF2 gene may be a therapeutic target for drug retention against relapse in orthodontics.40
Other studies focus on the role of osteoprotegerin as a therapeutic target. It has been used by applying physiological doses of its recombinant form in mice models subjected to orthodontic forces. It was observed that it inhibited relapse when applied locally, and produced minimal systemic and osseous effects; on the other hand, it was demonstrated that the effects in this model are localized on the applied area.41 A 2012 study by Zhao et al links the use of osteoprotegerin as an effective way to control the activity of osteoclasts; these results provide good evidence regarding the potential pharmaceutical use of this product in the control of post-orthodontic relapse.42 The studies point to this protein as a molecule with the closest potential for clinical use.43
There are many studies connected to this molecular and cellular topic. In addition to the ones reviewed above, some explain the etiological and physiological factors of cell and tissue responses to relapse, such as the production of apoptosis in relation to the response of the periodontal ligament involved in these movements.44 Others studies in treatment models, such as the application of strontium in Wistar rats, show an inhibitory effect of osteoclast production and osteoblast enhancer, which trigger a relapse stop by local use of injections on teeth affected by orthodontic forces.45 There are other relevant in-treatment studies with aspirin as an effective anti-relapse modulator through the control of Th1-mediated response, and molecules such as TNF-α and other immunomodulators.46
Use of low-intensity laser in relapse
Although the use of laser is relatively recent, its application in relapse following orthodontic treatment has a potential important use, in addition to the regular uses in acute pain management and in mechanisms of acceleration of dental movement.47
There has been recent information regarding the effectiveness of low-intensity laser therapy in molar relapse in animal models. A good part of the studies conclude that more research is needed to provide additional evidence; so far, laser seems to be effective in inhibiting osteoclastic action, possibly due to the role it plays in potential bone formation in areas that have been subjected to previous stress, and in the redistribution of these cells after remodeling the orthodontic force.37 However, further research is needed since the effects of low-intensity laser therapy on periodontal ligament remodeling during post-treatment relapses without retainers has shown to increase the recurrence rate after treatment.48
The role of third molars and special considerations in this regard
Another controversial topic that has long been in the field of orthodontics is the search for evidence regarding the problem of third molars and their role in crowding the anterior sector, as well as their influence on relapse, especially in the lower maxilla. Systematic reviews and meta-analysis on this topic have failed to provide strong evidence to resolve the discussion or to offer valuable data for a possible response, in part because the studies on this field are of low methodological quality and have questionable findings.49,50 It is worth noting that orthodontists consider the presence of third molars as a situation to ponder when it comes to choosing the most suitable retention mechanism for their patients.51
On the other hand, surgical approaches such as fiberotomy are additional study topics associated with relapse in orthodontic treatments; this technique is widely used to achieve rapid movements, and it also influences relapse. In a Wistar rat model, there was evidence that this type of intervention can improve the response by significantly decreasing relapse.52
DISCUSSION
The present study showed the retention and relapse scenarios in which teeth tend to return to their pre-orthodontic treatment state, mainly in anterior teeth. In this sense, the scientific literature has produced information regarding the characteristics of these processes and how they can be addressed to prevent changing results after a generally long clinical process.53 This means that an important post-treatment effort requires knowledge on retention mechanisms and their relationship to the causes of relapse.3
In this regard, when scientists make a publication as a result of their work, they list all the documents considered relevant to the subject, and thus the related works point to the ideas highlighted in the publication and help identify all the studies that happened prior to the publication and whose theories, concepts, methods, and contributions motivated the development of new research.54 Therefore, the analysis of citations and keywords can help other interested researchers identify the characteristic features of a publication, as well as the scientific interest in a particular community.
Despite being closely related, the two topics of this review-retention and relapse-have been widely researched by authors who analyze them and give each an argumentative and academic place. Based on the bibliometric indicators used in this document, scientific production seems to clearly show the information groups developed. The word graphics built with VosViewer 1.6.14 show that the two terms complement each other and run their own ways and interests among researchers. This is evident not only in keywords, titles, and abstracts, but also in the production by author and the fact that their values are similar.
Given the amount of information on relapse and retention-with sustained interest over time-55,56 and the information produced on the subject not only from etiology but also from treatment opportunities, the practitioners’ understanding, methodological options, the access and effectiveness of such options indicate that relapse is a highly important topic in orthodontics.57
A significant limitation of the present panoramic review has to do with the fact that other types of information analysis are sometimes required as recommended for these types of exploration, but were sacrificed in the present study for the sake of combining the two topics, and although it contains a significant amount of production, a full review is not always possible in large databases like WoS58-where all the revised articles were obtained-. Such databases contain a large number of articles and information available to interested readers, but do not always match their lists of interests, either because the source lacks focus or the readers simply fail to clearly see the field they want to interact with. This subjectivity determines the elements of the present exploration and explains the selection of some articles that are not necessarily among the main or most cited from the sources retrieved by the WoS search, but form the corpus of the content.
CONCLUSIONS
The two topics addressed in this review shed some light on the production of a theoretical body over the past ten years, with factors that can be summarized as follows: information related to surgical actions, assessments of the effect of treatments, studies related to molecular advances, experimental trials in search of evidence regarding the effectiveness of retention mechanisms, development of new forms of therapeutic approaches, recognition of practitioners’ attitudes and practices, the relationship with the periodontal structure in relation to antirelapse treatment and retention options.
Research on relapse and retention is not over yet, and on the contrary is required. Systematic reviews and meta-analysis on the subject have not yet provided sufficient evidence to clarify various debates on the two topics. This shows that the field is open for basic, clinical, and applied research. These two topics have been on the table for years, and they are undoubtedly still of uppermost interest in orthodontics as a discipline that relies on scientific evidence for its development, with knowledge being the base of much-if not all-of its clinical practice.

