











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
Despite the first cases of COVID-19 having been reported in December 2019, in Wuhan, China, it would take two months for the first Brazilian patient to be identified a man living in São Paulo, on February 25th (Croda et al., 2020). The Brazilian government’s response was swift, with both international and local health organizationscoordinating efforts to harmonize, plan and organize activities with the stakeholders involved (Croda & Garcia, 2020). Channels for direct contact with the population were established early on, through instant massaging apps and cell phone apps, to provide reliable information and prevent the propagation of fake news and/or distorted facts (Oliveira, Duarte, França, & Garcia, 2020). Guidance for prevention behaviours were also provided, which included recommendations for social distancing, hand washing procedures and, as of April 22nd, the use of cloth face masks in public venues (Oliveira et al., 2020)
In sharp contrast to the rapid governmental response, public opinion has been confused due to different measures and proposals from different official agencies (Statelevel vs. Central government) and the inevitable rise of fake news, along with the propagation of distorted facts. The Brazilian Ministry of Health itself acknowledges the necessity for heterogeneous strategies across States and Regions, considering the continental size of the country (Oliveira et al., 2020) and this may have contributed to the uncertainty faced by the population regarding the procedures to be adopted. If there is something certain about the first trimester of the year 2020, it is that people are uncertain about what is going to happen in the immediate and distant future. In commenting on the situation in Brazil, Gomes Mello and Rodrigues (2020) state that there is pervasive uncertainty about the disease, how to tackle it, and its economic, commercial, and political toll.
Although seldom confused in laymen terms (De Groot & Thurik, 2018), uncertainty and risk appear to describe two different scenarios. If you are capable of describing, not only the outcomes of a situation, but the distribution of probabilities of ex-ante outcomes, you are dealing with a risk scenario; on the other hand, if you only know the outcomes, but have little information regarding their probability distribution, then you are facing an uncertain scenario (see Knight, 1921, for the canonical definition). While betting on a single outcome from a die toss exemplifies a risky situation, betting on a horse in a horse race seems to involve an even greater deal of uncertainty. There are several findings from behavioural economics (Baillon, Cabantous, & Wakker, 2012) to psychology (Slovic, 2010) that corroborate the difference between these phenomena and the extent to which they are related to other psychological events (such as Depression, Anxiety and Stress).
Those findings also point to the fact that sensitivity to uncertain events is heterogeneously distributed in a population and there has been considerable efforts to devise and sharpen measurement tools to detect it (Gosselin et al., 2008; Greco & Roger, 2001; Roma & Hope, 2017). One aspect of our reactions to uncertainty frequently studied has been our intolerance to it. Intolerance of uncertainty (IU) has been defined as “the tendency of an individual to consider the possibility of a negative event occurring as unacceptable, irrespective of the probability of occurrence” (Carleton, Norton & Asmundson, 2007, p. 105). Although the concept was initially proposed to be associated with generalized anxiety disorder (GAD) (Dugas, Gosselin & Ladouceur, 2001; Dugas, Gagnon, Ladouceur & Freeston, 1998), it has recently been discovered as a contributing factor to a variety of mental disorders, from obsessive compulsive disorder (OCD) (Holaway, Heimberg & Coles, 2006), to social anxiety (Carleton, Collimore & Asmundson, 2010), depression (McEvoy & Mahoney, 2011) and panic disorder (Tolin, Abramowitz, Brigidi, & Foa, 2003). McEvoy and Erceg-Hurn (2016) go as far as to consider it a trans-diagnostic and trans-therapy factor, which means that treatment for several distinct mental disorders, from different theoretical backgrounds, should benefit from tackling intolerance of uncertainty. In a study following standardized treatment of 256 participants diagnosed with either GAD, social anxiety depression or depression, the authors found consistent evidence that changes in IU were closely related to changes in different symptoms related to the disorders.
In a scenario involving viral illness in a pandemic situation, Taha Matheson, Cronin, and Anisman, (2014) addressed the sequential interplay between IU, coping strategies, and anxiety based on 1,027 self-reported questionnaires during the 2009 H1N1 pandemic. The authors warn that, should the government officials fail to prevent the worry and hysteria related to viral contraction, the uncertain estimates related to the threat may increase perception of uncertainty and thus increase anxiety. Elledge, Brand, Regens and Boatright, (2008) investigated the public understanding of the Avian Flu, a threatening viral illness, around 2006, in a North American city, and found little evidence of solid knowledge in the population researched. Results indicate that participants were ill-informed about the severity of the illness, about the United States’ coping potential and about the proximity of a vaccine or effective treatment. Although authors consider it safe to assume that participants were exposed to information about the avian flu, it seems clear that “accurate communication of risk (and uncertainty) was faulty”. Satici, Saricali, Satici and Griffiths (2020) have studied a large sample of Turkish nationals and established an inverse relation between IU and Mental Wellbeing, measured by the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS; Tennant et al. 2007). Rumination and a Fear of COVID-19 (measured by the FCV-19S Scale; Ahorsu et al. (2020) partially mediated the relation, elucidating possible psychological mechanisms responsible for the decrease of mental wellbeing in high IU participants facing the pandemic. Bakioğlu, Korkmaz, and Ercan (2020) found similar results in another Turkish sample, presenting evidence for the relation of Fear of Covid-19, IU, mental health indicators (depression, anxiety and stress) and positivity. The authors’ proposed model indicates the role of IU and mental health indicators as mediators of the relation between fear of COVID-19 and positivity, again designating a relevant role played by IU.
As of May 25th, 2020, the COVID-19 pandemic has escalated into a major world-wide health crisis, with 5,304,772 confirmed cases and 342,029 deaths (BRASIL, 2018). In Brazil, there have been 22,013 deaths and 347,398 confirmed cases, even though lack of effective testing makes this estimate less reliable. Lipsitch, Phil, Swerdlow and Finelli, (2020) question the use of confirmed cases as good indicators to model the current epidemic’s dynamics, partially because of the relevant role of asymptomatic infected people in spreading the virus, so the correct number of infections will remain uncertain for some time. An additional problem is the lack of criteria for differential clinical diagnosis, since clinical features of COVID-19 are non-specific and may be seen in several different respiratory illnesses (Phua et al., 2020). This situation may characterize the COVID-19 pandemic as a particularly challenging situation to cope with. Uncertainly about the disease’s transmission and about the effectiveness of prevention procedures may be related to severe psychological distress, including anxiety, depression, and acute stress disorder (Gardner & Moalef, 2015; Jiang et al., 2020; Tavares Lima et al., 2020). These factors warrant research on mental health assessment, support, treatment, and services related to COVID-19 (Xiang et al., 2020).
The current study investigates how differential responses to the uncertainty of events (measured by IUS-12) may be related to depression, anxiety and stress symptomatology (measured by DASS-21) during the early days of the COVID-19 pandemic in Sergipe, a north eastern state in Brazil. The research presented here is a part of the first of a three-wave monitoring project aimed at describing mental health indicators during the initial, intermediate, and final moments of the COVID-19 pandemic in Brazil.
Method
Participants
The sample comprised of 924 participants, from both genders, from 18 to 72 years old (mean (M) = 36.8; standard deviation (SD) = 11.70), residing in Sergipe, a state in the north eastern region of Brazil. The majority reported being in the capital (69.7%; n = 613) during the survey, and the others in different cities of the state (30.3%, n = 267). Most of the sample (95.5%; n = 882) reported having complete or incomplete higher education and the rest (4.5%; n = 42) said they had complete or incomplete high school education. Regarding skin colour, people who declared themselves to be Brazilian Asians, indigenous or other, were excluded from the sample, due to the small amount. More than half declared themselves to be “pardo” - Brazilian mixed ethnicity (54.3%, n = 502), followed by white (34.2%, n = 316) and black (11.5%; n = 106). Most (61.7%, n = 570) said they had a fixed income and the rest said they were unemployed or did not have a fixed income (38.3%; n = 354).
Instruments
Sociodemographic Questionnaire. Used to collect information such as self-identified gender (male, female), age (in years) and education (complete or incomplete high school, and complete or incomplete higher education).
Reduced Intolerance Uncertainty Scale (IUS-12) (Carleton et al., 2007;Kretzmann, 2018). Composed of 12 items on the scale of the type of agreement (01 to 07), distributed into two dimensions: (1) Prospective Anxiety and (2) Inhibitory Anxiety. Cronbach’s alpha was .79; .86 and .88 for Prospective and Inhibitory Anxiety subscales and total scores, respectively.
Depression, Anxiety and Stress Scale Short Form (DASS-21) (Apóstolo, Mendes & Azeredo, 2006;Vignola & Tucci, 2014). Likert scale of occurrence of symptomatic changes (4 points), distributed into 21 items, which generates independent scores on anxiety symptoms, depression and stress over the last week. Cronbach’s data in this research were .83, .88, .89 and .94 for the factors of anxiety, depression, stress and the whole scale, respectively.
Procedures and Ethical Aspects
A survey was conducted from April 3 to April 16, 2020, which corresponded to a period of quarantine and social isolation imposed by the government of Sergipe (Decreto 40560 de 16 de Março, 2020). The sampling was made by convenience and snowballing methods. Participants received a public invitation on social media to participate in an online survey regarding mental health in the confinement period. The first research screen presented a free and informed Consent Form online. The project was approved by the National Council for Ethics in Research (Conselho Nacional de Ética em Pesquisa (CONEP); register n. 3.954.144).
Data Analysis
Data were analysed using SPSS (v. 24) for descriptive statistics (absolute and relative frequencies, media, media and standard deviations), and inferential statistics (binomial logistic regressions and a multinomial). For binomial logistic regressions, the dependent variables were scores for anxiety, depression and stress, all dichotomized by the median, considering the non-parametric distribution of the total sample. In the binomial models, the factors were Prospective and Inhibitory Anxiety, gender (male or female) and age (divided into four groups: up to 30 years old, between 30 to 40 years old, between 40 to 50 years old, and more than 50 years old).
All regressions were performed through the Backward LR methods (binomial logistic regression), which do not require the selection of variables before the final modelling (Field, 2009). For the evaluation of binomial models, the following indicators were observed: Omnibus test (expected to be statistically significant), Nagelkerke’s R² (expected the higher the better, corresponding to the explained variance of the final model), Hosmer and Lemeshow test (expected not be statistically significant) and correct predictive capacity of the model (expected to be around 70%). The multicollinearity assessment was carried out for all models and no problems were found in the composition or final solution of the models. It is worth noting that all Odds Ratio (OR) values below 1 were converted by the formula 1 / OR to standardize the description of the findings. The p-value adopted was less than .05 for all steps of binomial regressions.
Results
Sample Profile
The sample’s mean age was 36.8 years old (SD = 11.70). After categorization, the proportion for each age group was 35.3% (n = 326) up to 30 years of age, 26.7% (n = 247) between 30 and 40 years of age, 23.8 % (n = 220) between 40 and 50 years old and 14.2% (n = 131) over 50 years old. Most of the participants were female (79.0%; n = 730).
Due to the non-normal distribution of anxiety, depression and stress scores in the present sample, its median was obtained as the most reliable indicator of the sample midpoint. The median was 2, 4 and 6 points for anxiety, depression and stress, respectively. After categorizing the outcomes according to the midpoint, 48.8% (n = 451) of the participants were above the median of the anxiety score, 41.9% (n = 387) above the median depression, and 44.8% (n = 414) above the median in the stress variable. On IUS12, the factors Prospective Anxiety and Inhibitory Anxi ety averaged 21.3 (SD = 6.31) and 13.0 (SD = 5.63) points, respectively. When classified into three strata of scores, the distribution in the Prospective Anxiety factor was as follows: low (up to 18 points) with 34.5% (n = 319), moderate (between 18 and 24 points) with 32, 6% (n = 301) and high (greater than 24 points) with 33.1% (n = 306). For the Inhibitory Anxiety factor, the low group (up to 9 points) was 33.4% (n = 309), moderate (between 9 and 15 points) with 33.4% (n = 309) and high (greater than 15 points) with 33.1% (n = 306) individuals.
Logistic regressions
Three binomial logistic regressions were performed, one for each DASS-21 outcome, categorized by a median. Table 1 shows the results of each model, as well as their adjustment indicators. In stress outcome, all independent variables were included in the final model. The female gender had three times more chances to be in the group above the stress median (OR = 2.7) and the age showed a relatively linear relationship. People up to 30 years old had a higher presence among those above the median of anxiety compared to the other age groups, namely: almost twice as many chances than those between 30 and 40 years old (OR = 0.5 and 1/OR=1.9), two and a half times more chances than those between 40 and 50 years old (OR = 0.4 and 1/OR = 2.5) and also twice as many chances than those over 50 years old (OR = 0.5 and 1/OR = 2.0). On IUS-12, Prospective Anxiety factor, individuals in the high group (greater than 24 points) exhibited chances about twice as high (OR = 1.9) as those in the low group (up to 18 points). There was no significance for the moderate group (greater than 18 and up to 24 points) in relation to the low BP group. In the factor Inhibitory Uncertainty, the participants classified as moderate (between 9 and 15 points) had twice as many chances to score higher on the stress scale (OR = 2.1). The high group (more than 15 points) had almost four times more chances of being above the stress median (OR = 3.9).
Table 1 Binomial Logistic Regression Indicators for Stress, Anxiety and Depression in DASS-21
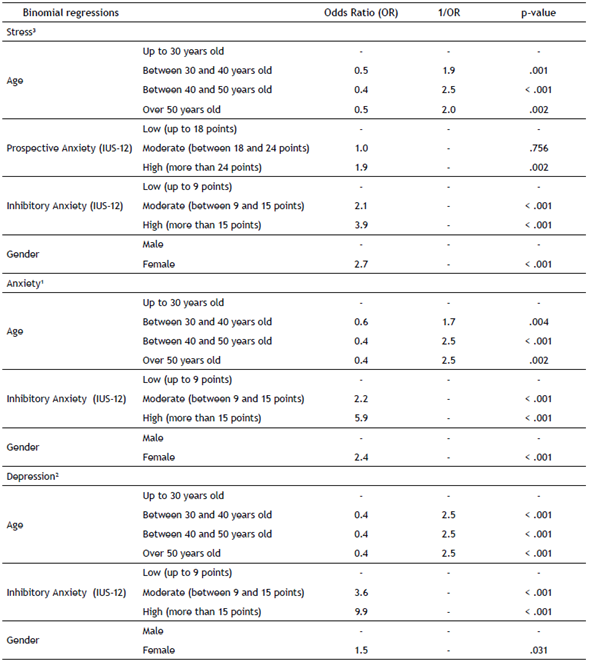
Notes. * Variables with no statistical significance in each model were excluded from the table.
1. Stress outcome: Omnibus test = 166.952 (p < .001). Hosmer and Lemeshow X² test = 4.672 (p = .792). Nagelkerke R² = .221 (22.1%). Percentage of correctly predicted cases = 68%.
2. Anxiety outcome: Omnibus test = 160.686 (p < .001). Hosmer and Lemeshow X² test = 3,484 (p = 0.900). Nagelkerke R² = .213 (21.3%). Percentage of correctly predicted cases = 69%.
3. Depression outcome: Omnibus test = 205,600 (p < .001). Hosmer and Lemeshow X² test = 5,513 (p = .598). Nagelkerke R² = .268 (26.8%). Percentage of correctly predicted cases = 72%.
On the anxiety scale, it was seen that the final model was composed by the variables gender, age and Inhibitory Anxiety, a subscale of the Intolerance of Uncertainty Scale. The female model showed higher chances to be in the group above the anxiety median compared to the male model (OR = 2.4). Regarding age, the proportion was similar to that found for stress: the youngest had higher chances. Those up to 30 years old had higher chances for high anxiety scores compared to those between 30 and 40 years old (OR = 0.6; 1/OR = 1.7), those between 40 and 50 years old (OR = 0.4; 1/OR = 2.5) and those over 50 years old (OR = 0.4; 1/OR = 2.5). The factor Inhibitory Anxiety of IUS-12 also exhibited a relative progression of risk. Individuals who scored moderate (between 9 and 15 points) and high (greater than 15 points) had higher chances of composing the stratum of people with scores above the anxiety median (OR = 2.2 and OR = 5.9, respectively).
Finally, for the depression outcome, the same variables independent of the anxiety model remained in the final solution. The female gender with high odds (OR = 1.5) and age followed a similar pattern: younger (up to 30 years old) were more exposed, and in all comparisons the OR values were 2.5, i.e. two and a half times more likely to be in the group with scores above the median depression. The factor Inhibitory Anxiety was also significant, with high Odds ratio. The group with a moderate score showed 3.6 more chances and those with a high score had 9.9 times more chances of being in the group with depression scores above the median.
Discussion
Our results corroborate existing findings in regards to the higher propensities of depression, anxiety and stress in women (Novais, Monteiro, Roque, Correia-Nevez, & Sousa, 2016; Rincón-Cortés, Herman, Lupien, Maguire, & Shansky, 2019; Salk, Hyde, & Abramson, 2017) and young age groups (e.g., Flint et al., 2010; Novais et al., 2016). Stress and Anxiety, in particular, were found to be up to three times more prominent in women, a result in line with those obtained by Bakioğlu, et al., (2020) and Wang et al., (2020). Several factors have been considered as causes for this robust finding, including physiological and socio-economical differences (Kuehner, 2017). A recent rise in the role of female headed households (BRASIL, 2018) may add to the explanation of these results, considering the heavy economic impact of the COVID-19 pandemic. Younger participants in our research also demonstrated a higher chance of manifesting Depression, Anxiety and Stress, consistently displaying 2 to 2.5 times the odds of being over the median in regards to all of these measures. These results are not spurious and appear to show a trend in recent COVID-19 mental health monitoring studies. Huang and Zhao (2020) have observed a similar trend in a Chinese sample, while Liu et al., (2020) found the same result with an American sample and attributes this to the distress in managing work and school responsibilities, the latter being one of the first areas hit by social isolation and quarantine protocols. Although not directly investigated, it is feasible that underdeveloped coping skills and other psychological adaptive factors (such as Self-Esteem, Orth, & Robins, 2014) in younger participants play a relevant role throughout this public health crisis.
The association between the scores of intolerance of uncertainty and the results of the DASS-21 scale are also evident in our results, and these too corroborate the existing literature (Bottesi, Noventa, Freeston, & Ghisi, 2019). Participants over the 3rd tertile on the Prospective Anxiety subscale of IUS-12 were almost twice as likely to have higher than median scores when it comes to Stress. Greco and Rogers (2003) had similar results, although with a physiological measure of stress and a different instrument to measure intolerance of uncertainty. It is worth noting that the Prospective Anxiety was only significantly associated with Stress. As defined by Hong and Lee (2015, p. 606), Prospective Anxiety “seems to represent a desire for predictability of future events, triggered by anxious apprehension about uncertainty, and prompting engagement in strategies (e.g., seeking more information) to reduce uncertainty” and is closely related to worrying and symptoms of Obsessive-Compulsive Disorder.
The Inhibitory Anxiety subscale was significantly related to all three DASS-21 subscales, and participants in the 3rd tertile on this scale were 4, 6 and 10 times more likely to have higher than median scores of Stress, Anxiety and Depression, respectively. This concept measures paralysis and the compromised functioning in reaction to uncertainty (Berenbaum, Bredemeier & Thompson, 2008), so its extreme impact on depression measures should be expected, but also the expressive effects on Stress and Anxiety can be highlighted in the current results. Hong and Lee (2015) obtained results similar to ours, with Depression and Anxiety being the most impacted by higher scores on the Inhibitory subscale of IUS-12.
In sum, our results describe a scenario in which intolerance of uncertainty plays a relevant role in the mental health of participants during the initial phase of the COVID-19 pandemic. All measures employed were significantly and positively related to uncertainty intolerance, so our research is in line with the evidence suggesting that Intolerance of Uncertainty may be regarded as a transdiagnostic factor (McEvoy & Erceg-Hurn, 2016) related to Depression, Anxiety and Stress, even though we did not investigate any behavioural or psychological mechanism that could be responsible for the observed results. Some features of our study must be considered before extrapolating our findings. First, our participant sample was big (n > 1000), but recruited in a non-systematic fashion, through social media apps, rendering it unrepresentative of Sergipe´s population. Second, since this is the first wave of a three-part monitoring research project, it remains to be evaluated how possible changes in the public perception of the threats posed by the pandemic will affect the inhabitants of Sergipe, and how these changes will affect mental health, and behavioural and psychological measures. For future research, it is suggested that the link between mental health measures and specific behavioural indicators (such as propensity to remain socially isolated or to adopt prevention strategies) be directly investigated. Additionally, the impact of the pandemic on the development or the severity of specific anxiety disorders should be investigated (e.g. social phobia, health anxiety, generalized anxiety disorder, and agoraphobia), as well as the role of different coping strategies and positive emotions (e.g. hope) to deal with the daily adversities related to COVID-19. And finally, following the results obtained by Bakioğlu et al., (2020) and Satici et al. (2020), more work investigating possible variables mediating the effects of IU on mental health, such as optimism, worry and hope, should be conducted. This would help to elucidate whether IU plays a role as a predictor, as suggested by Carleton (2016) or as a mediating variable, as proposed by Bakioğlu et al., (2020).

