










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAvances en Enfermería
versão impressa ISSN 0121-4500
av.enferm. v.28 supl.1 Bogotá jun. 2010
VIRGINIA INÉS SOTO LESMES1, MARÍA MERCEDES DURÁN DE VILLALOBOS2
1 Enfermera, profesora asociada, Facultad de Enfermería, Universidad Nacional de Colombia. Doctora en Enfermería, Universidad Nacional de Colombia. Directora programa de doctorado en Enfermería, Universidad Nacional de Colombia. visotol@unal.edu.co Bogotá, Colombia.
2 Directora de Tesis, enfermera, profesora titular emérita, Facultad de Enfermería, Universidad Nacional de Colombia. Profesora emérita Universidad Nacional de Colombia; máster en Ciencias de la Enfermería. mmvillalobos@gmail.com, Bogotá, Colombia.
Recibido: 12-06-10 Aprobado: 20-08-10
Abstract
Based on grounded theory, this study describes the experience with pregnancy in a group of teenagers and proposes a hypothesis on that experience. The data was collected through in-depth interviews with 30 pregnant teenagers. Seven categories were drawn from the analysis: unexpected pregnancy, accepting pregnancy, experimenting with ways to look after yourself, suffering loss due to pregnancy, blaming yourself for the pregnancy, resisting abortion and rebuilding support networks. To construct a central category and, ultimately, to arrive at the assumption that teenage girls "want to become pregnant, but not so soon." Accordingly, the concept of ambivalence is used as the thread to demonstrate how this sequence of actions/interactions evolves in response to the pregnancy experience and how they align themselves pursuant to the conditions and changes in their ambivalent context.
The conclusion is that pregnant teens leave contraception up to the male. However, when becoming pregnant, they assign no blame or responsibility to their sexual partner and even excuse him. Associate care or protection with changes in their social behavior and the physical changes are not significant. 21% of the teenagers in the study are in their second pregnancy. This is an indicator of dramatic proportions for the well-being of these young women and their unborn children. The parent-adolescent relationship is reinforced during the pregnancy. However, when the mothers of these teenagers learned their daughters were sexually active, they ignore it. Urgently calls for innovative strategies to provide individualized and contextualized care are made.
Key words: adolescent, pregnancy, qualitative research, nursing care, nursing
Resumen
Este estudio se apoyó en la teoría fundamentada, los objetivos fueron: describir la experiencia del embarazo de un grupo de adolescentes y generar un planteamiento hipotético sobre las experiencias de su embarazo. Se recolectaron datos a través de entrevistas a profundidad a 30 adolescentes gestantes, Del análisis emergieron siete categorías: "Embarazo inesperado", "Asumiendo el embarazo", "Experimentando formas de cuidarse", "Padeciendo pérdidas por el embarazo", "Culpándose por el embarazo", "Resistiéndose al aborto" y "Reedificando redes de apoyo". Emerge la categoría central y por ende el planteamiento hipotético afirmando que las adolescentes están "Deseando el embarazo pero no tan pronto". Se parte del concepto ambivalencia como hilo conductor para mostrar cómo evoluciona esta secuencia de acciones/interacciones en respuesta a la experiencia del embarazo y cómo se alinean según las condiciones y cambios que han experimentado en su contexto también ambivalente.
Se concluye que las adolescentes embarazadas delegan en el hombre la protección frente a un posible embarazo, sin embargo, cuando se enteran de estar embarazadas los excluyen y excusan de cualquier responsabilidad. Asocian cuidado con cambios en sus comportamientos sociales sin ser significativos los cambios físicos. El 21% de las participantes, están pasando por su segundo embarazo, indicador alarmante para el bienestar de estas jóvenes y sus hijos por nacer. La relación padres-adolescente se afianza durante el embarazo, aunque sus madres cuando tuvieron conocimiento de que sus hijas ya habían iniciado su actividad sexual, lo ignoraron. Se hace un llamado urgente a innovar estrategias de cuidado individualizado y contextualizado.
Palabras clave: adolescente, embarazo, investigación cualitativa, atención de enfermería , enfermería
Resumo
Este estudo foi realizado com base teórica e objetivou o seguinte: descrever a experiência de gravidez e gerar uma hipótese sobre esse processo em um grupo de adolescentes; coletar dados através de entrevistas em profundidade realizadas em 30 adolescentes grávidas.
Sete categorias surgiram da analise: "Gravidez inesperada"; "Assumindo a gravidez", "Experimentando métodos de prevenção", "Sofrendo perdas pela gravidez", "Sentindo culpa pela gravidez", "Rejeitando o aborto" e "Reconstruindo redes de apoio".
Surge a categoria central e, portanto, a hipótese afirmando que as adolescentes estão "Querendo engravidar, mas não tão cedo". O estudo está baseado no conceito de "ambivalência" como fio condutor para mostrar a evolução desta seqüência de ações/interações em resposta à experiência da gravidez e como elas se agrupam segundo as condições e mudanças que têm vivenciado também dentro de um contexto ambivalente.
Em conclusão, as adolescentes grávidas deixam no homem a tutela perante possível gravidez. Porém, assim que elas conhecem sua gravidez, rejeitam e desculpam os homens de qualquer responsabilidade. Elas relacionam cuidado com mudanças em seus comportamentos sociais sem considerar significativas as mudanças físicas. Dessa amostra de participantes, 21% está passando por sua segunda gravidez, isto é um indicador alarmante para o bem-estar das adolescentes e seus filhos por nascer. A relação pais/adolescentes se fortalece durante a gravidez, embora as mães não levassem em conta o fato de suas filhas terem iniciado sua atividade sexual. Fazemos um apelo urgente para a inovação de estratégias de cuidado individual e contextualizado.
Palabras chave: adolescent, gravidez, pesquisa qualitativa, cuidados de enfermagem, enfermagem
INTRODUCTION
The paper we are about to present outlines the experience of pregnancy for a group of teenagers. The authors found that teenagers "want to become pregnant… but not so soon."
In recent decades, adolescence (1, 2) has come to be regarded, and even experienced, as a time of life when "people live at full speed". In fact, most adults feel it is the happiest time of life. Pregnancy, at this stage in their development is an experience that transformed the lives of a group of teenagers from the Kennedy district in the city of Bogota. To cite only a couple of figures, according to the United Nations Population Division, the rate of teenage pregnancy in the Latin American and Caribbean region was 16.2% in 2002 (3). This represents approximately 2.3 million teens and is 36% higher than the world average.
In 2006, in Bogotá alone, there were 22.228 pregnancies reported among teenagers between 10 and 19 years of age. This amounts to 719 pregnancies more than the year before and, in 90% of these cases (18.205), the expectant mother was between 15 and 19 years of age (4). These alarming figures place Bogotá at the same level as countries such as Uganda and Sierra Leone. In Colombia, the teenage fertility rate in 2005 was estimated at 90 births per 1.000 women. However, in Bogotá, it was 170 per 1.000 inhabitants; in the aforementioned countries, the average is 200 for every 1.000 inhabitants (4).
Different approaches to the study of teenage pregnancy range from a focus on the physical risks, which are associated with biological maturity (5, 6, 7, 8, 9, 10), to the emotional risks, which are characterized by an increased need to be loved and the fear of being a failure (11). This makes pregnant teens vulnerable to pressure from partners or peers. In such cases, they can interrupt the process of separation and individualization, achieving only partial identity as an adult (12). Other approaches focus on the social risks associated with early sexual relations (13, 14, 15), violence (16, 11), ethnic minorities (17, 18), poverty (12, 13) and place of residence (13).
This study is an attempt to understand what the experience of pregnancy is like for teens and what elements intervene in that reality.
From a conceptual standpoint, pregnant teens experiences can be understood in light of the concepts of "Experience (32, 33, 34), Symbolic Interactionism (36, 37, 38) and Hermeneutics (21)." Mead (1934) analyzes experience from the perspective of communication, as an element that is essential to the social order, since individual autonomy development and self-awareness in the field of one’s own experience is preeminently social (19). As for symbolic interactionism, the same author recognizes that individual behavior cannot be analyzed without considering the social context in which the individual deals with life (20). For that reason, conscience is linked to the social context and is shaped through continuous social interaction (20). Hermeneutics becomes part of this conceptual framework, very much along the same lines as the other two concepts mentioned already, since the interpreter and the object subject to interpretation are understood as a single moment. This highlights the inter-subjectivity of communication through language, which is the means by which domination and social power are reproduced (21). It implies a discontinuous and intermittent effort at translation and understanding, one that occurs repeatedly. In other words, hermeneutics is associated with the art of understanding what is communicated linguistically and translating it in to what is understandable (21).
The design framework marks the transition from the conceptual to the empirical and, since this subjective reality is unknown, it becomes an interpretive study (35). Symbolic interactionism calls for fluid and dynamic processes with respect to interpersonal relations in which meaning is created as a result of that interaction, and where the assumption is that people construct their reality through social interaction in which they use shared symbols (e.g. words, clothing, gestures) to convey meaning. Accordingly, grounded theory (41) looks at the meaning created in these social relationships, attempting to discover how a group of pregnant teenagers defines the reality of their situation based on their understanding of interpersonal interactions (22).
The in-depth interview was the instrument selected to collect the information for this study, based invariably on the premise that an interview is inevitably, at some level, as personal and intimate a meeting as it is public (23). Thirty-one in-depth interviews were conducted. Each lasted 50 minutes, on average, and produced a wealth of information that amounted to 23 recorded hours. Scientific rigor was ensured from the auditability (43) through periodic assessments on committees tutorials. The credibility (44), collection of information took more than 18 months; in addition, participants recognized their own experiences through two focus groups.
Analysis began once the interview was recorded and transcribed. The substantive codes (39, 42) were identified; these are nothing more than the means by which segments of sentences are recorded. Accompanied by the notes (40) that are taken, they gave birth to construction of the categories, which are, in turn, the concepts derived from the data (24) and represent the experiences of pregnant teens in this particular context. Once a number of closely related concepts began to accumulate, they were grouped according to their properties and dimensions (24), which naturally were validated in each of the thirty-one interviews. Seven categories emerged from this analysis.
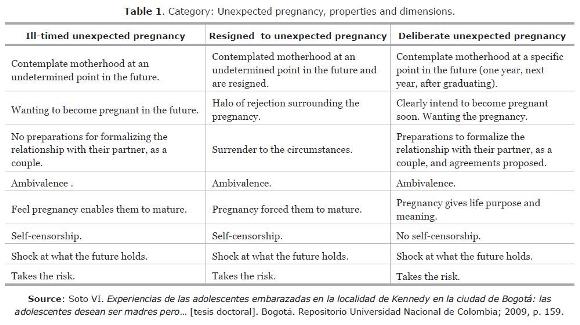
Unexpected pregnancy. In their transition to adulthood, teenage girls believe they should become mothers. In other words, they feed the need to assume a maternal role. Having a baby makes them feel they have something of their own, someone who depends solely on them. This is why the participants in the study admit to having contemplated the possibility of motherhood at some point in the future. Their stories show they equate motherhood with being an adult. Facing the responsibility of an early pregnancy is seen as a way to achieve the independence they long for.
Of course, because of that the very same transition, they go back and forth between being a child and being an adult. This creates a great deal of uncertainty, making it difficult for them to gauge the risks and consequences of an early pregnancy. Recognizing the pregnancy is ill-timed, generates contradictory feelings and a sense of loss, among other emotions.
Here, it is important to bring Mead into the equation. He sees the human experience as essentially dynamic (19). Pregnancy experience is constructed on a temporary and novel basis, not only with respect to the present, but to the past and future as well. The future lies beyond the current pregnancy, and the pregnancy unexpectedness is what makes it novel. Pregnancy creates a future that comes as a surprise.
Another dimension refers to an unexpected pregnancy that is met with resignation or is the result of conjunctural conditions. Some pregnant teenagers acknowledged their lack of preparation for pregnancy, accepting there is no alternative or nothing that can be done. This acceptance state is one of resignation. It is as if they are surrendering to the circumstances, and the experience is accompanied by a halo of rejection, as pregnancy forces them to grow up.
A third dimension of unexpected pregnancy becomes obvious when the participants manifest acceptance that is more deliberate, inasmuch as they had contemplated motherhood sometime in the future, had planned to formalize the relationship with their partner, and had proposed certain arrangements or agreements concerning a possible pregnancy (Table 1).
At this point, it is important to emphasize that the concepts that qualify as categories are abstractions and represent the life stories of all the teenagers who took part in the study, reduced in conceptual terms and represented by them (24).
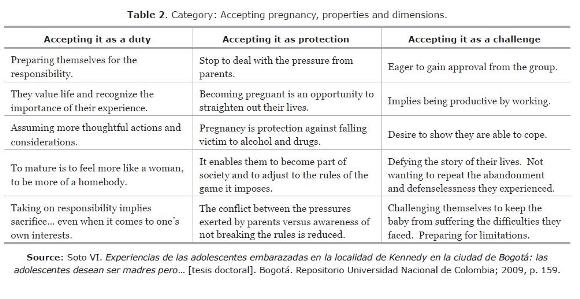
The category "Accepting Pregnancy" is addressed, seeing as it is when teenagers first give meaning to the experience and recognize it as an unavoidable responsibility, one they may not be prepared for but cannot avoid, regardless of whatever decision they make with respect to continuing the pregnancy. They reveal having experienced thoughts and deeds aimed at avoiding disadvantages for themselves and their babies. Pregnancy is recognized initially as a situation that implies more responsibility, which they must assume. This responsibility and maturity levels can be considered unusual for the development stage in which these teenagers find themselves and, therefore, should be used to advantage (25). They are willing to take on the motherhood responsibility, but are still not specific about the difficulties they will have to face. According, their course of life changes; they become more conscious of the fact that someone will depend solely on them.
A second variation of the properties in this category is evident when teenage girls recognize this experience is an opportunity for help them to straighten out their lives. It offers a kind of protection that helps them to integrate into society and adjust to the rules it imposes. In this way, they think they can avoid the conflict between peer pressure and the awareness of not having broken society’s rules.
Finally, teenage girls acknowledge pregnancy as a way to prove themselves and to demonstrate their abilities and potential to others. For them, taking on the pregnancy challenge means they must work and be productive, to prosper with their babies. One repeatedly hears the expression: "so they can take care of themselves". This could mean some of these girls were abandoned or neglected by their parents. For this reason, they want a child, recognizing, of course, their immaturity for the task, especially when they have to find work that will give them enough income to achieve the goals they propose for themselves (Table 2).
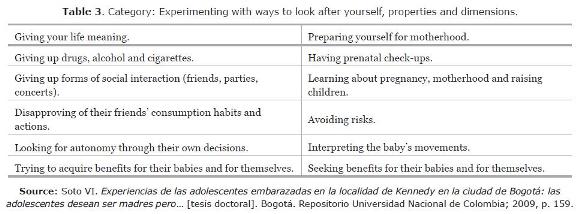
Experimenting with ways to care for themselves: this category reveals that teenagers carefully examine their new identity as pregnant women and believe they cannot do many of the things they did before becoming pregnant. They agree to exchange some things for others, and associate responsibility with abandoning the ways they had fun and interacted socially prior to the pregnancy. They claim to have quit smoking and drinking, and stopped doing drugs, despite pressure from friends or their partners, all for the sole purpose of protecting the baby. In this case, it seems that pregnancy is an opportunity for more freedom and autonomy; it is a positive change, besides being an interesting way to care for oneself. A strategy that benefits them physically, mentally and socially.
Forsaking certain habits and friends creates a feeling of strangeness; however, it does not seem to be a feeling of loss. When listening again to the testimonies, one finds that most of them contain no long silences, no substantial changes in tone of voice, nor sobbing or crying. Giving up friends and social relationships can be very painful, particularly when considering these two aspects of adolescence can be more important and more intense than the relationship teenagers have with their parents or relatives.
The participants acknowledge they are getting ready for motherhood by having regular medical check-ups, learning about pregnancy and preparing themselves for child-raising through experiences with other children (Table 3).
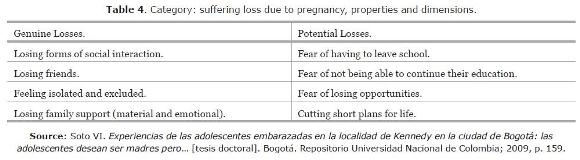
Suffering loss due to pregnancy. For these teenage girls, experiencing real or even potential loss is the price of continuing their pregnancy. They acknowledge being forced to make decisions that are painful and full of disappointment. These thoughts, which express suffering, are shaped by the form of social interaction that occurs during this stage of development. At school, they experience a greater loss when they feel rejected by their peers; it is a form of social exclusion. Similar case occurs in the study of Whitehead (26), reporting that teenagers succumb to the weight of social sanction and feel a sense of social death (26). In addition, when these girls talk about their lives, one detects expressions of loss when they emphasize how painful it is to lose the support of the immediate family (parents, siblings). The loss of emotional support is more significant than the loss of physical or material support, and it creates added insecurity and low self-esteem (Table 4).
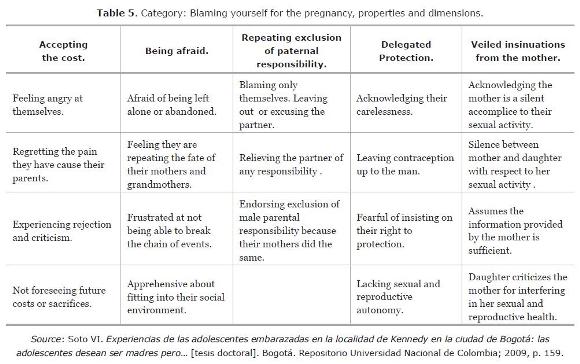
Blaming themselves for the pregnancy. The use of expressions such as I felt, I want-wanted, I had, I believe and to think is significant. They are repeated from three to seven times in the testimonies and are accompanied by silence, hesitation and changes in tone of voice. These expressions constitute part of the basis for the construction of this category. The feeling is mediated through a sense of grief. They acknowledge the suffering and disappointment they have caused their loved ones. Most of these girls want to make sure they do not fail and courageously grasp the consequences that lead them to assume responsibility through a feeling of guilt.
The dimensions in this category are significant. The first dimension concerns to recognize they have broken the rules and feel they must pay the price. Their conscience becomes more severe and sensitive to restrain aggression towards others (27). The price includes being angry with themselves, the pain of having disappointed their parents, the changes created in family dynamics, such as the mother having to go to work to support the teenager and her unborn child, so as to mitigate some of the tension generated by the father. In other cases, pain is manifested when they realize they did not make better use of their opportunities, such as access to education and the efforts of their parents to provide what they need to attend school (clothing and school supplies). These tensions, which generate guilt over having broken the rules, are associated with rejection and blame.
The second dimension deals with the harsh fear of being left alone with the responsibility of a pregnancy, since that is the experience of the women around them such as their mothers, sisters and friends. This reinterpretation heightens their feeling of guilt. On the one hand, they knew the consequences; on the other, they have disappointed their mothers, who had hoped their daughters would break the chain of events in terms of having to assume a pregnancy alone.
The third dimension becomes evident when the participants assume the pregnancy is their fault and relieve the partner of any responsibility or even try to exempt him of responsibility in a veiled way, particularly when they acknowledge the existence and accessibility of means to avoid pregnancy. Relieving the sexual partner of parental responsibility may be the result of what they have been told by their grandmothers, mothers, aunts, older sisters or their friends who ultimately were left alone to face the reality of pregnancy in a society where they had broken the rules. It is valid to infer that the replication of excluding or exempting the partner of paternal responsibility is almost automatic among the participants. Ideas about the role sons and daughters must play in society are conveyed to children early on, even in the womb, and are based on the mother’s way of thinking (the challenge is how nursing can help to break this chain of events).
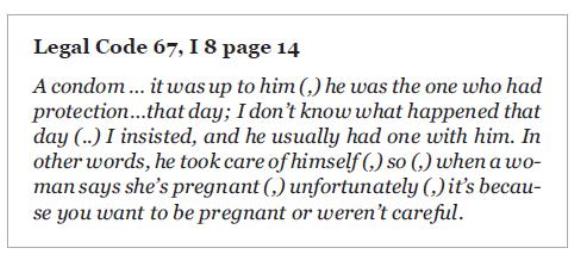
The fourth dimension refers to the participants’ admission of not having made frequent and disciplined use of condoms as a strategy to avoid pregnancy. They assume responsibility for the pregnancy that resulted from failing to do so and blame themselves. This feeling of guilt is aggravated when they admit their partner was the one who used contraception and confess to having delegated ultimate responsibility for contraception to the man. The perception is that these teenagers do not take responsibility for their own care and are not positioned to act autonomously with respect to their sexual and reproductive health.
Finally, it is clear that some participants were warned of the risk of pregnancy and admit their mothers knew they were sexually active. Therefore, in their minds, having the mother merely warn them to be careful about becoming pregnant seems sufficient in itself. Some mothers try to talk about the use of family planning methods, but in a veiled and shy way. Consequently, the explanation is not clear enough for teenage girls to acquire any real self-determination with respect to their sexual lives, much less to protect themselves and to plan properly. Some of the testimonies are significant in that pregnant teenagers believe their mothers have neither the criteria, nor the responsibility or the moral authority to educate them and to give them the tools they need to manage their sexual and reproductive health (Table 5).
In this respect, one wonders what happens with the sex education and health programs offered in schools. What happens to the messages published in the press and broadcast on radio and television about the use of condoms?
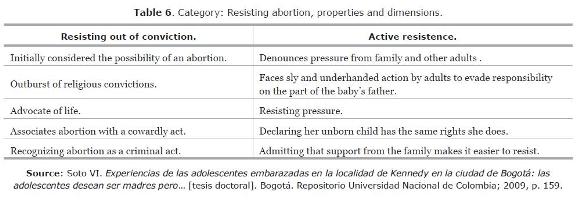
Resisting abortion. In these testimonies, one hears expressions such as I reacted, it never occurred to me, I wouldn’t be able to, it’s illogical, they don’t deserve it, and so much pressure. The indication seems to be that girls somehow feel capable of rejecting and opposing abortion as an unacceptable alternative. Although abortion is associated with unwanted pregnancy, as noted by Mngadi (28) and Drescher (17), the young women in this sample are able to assess the harm that could come from trying to have an abortion. For example, they look on abortion as a criminal act. They also suggest their unborn children should not have to pay for their neglect with their lives, especially since they see their unborn children equals. The participants in this study admit they initially opposed abortion out of conviction. At first, perhaps because of the suddenness of the experience, they see abortion as a way to deal with the tension generated by an unexpected pregnancy. There also is an outburst of religious beliefs, such as having the power to foster life, or believing God has sent them a child so they can provide it with a better life than they had. They claim to be defenders of life, recognizing the embryo is a person and declaring abortion to be a cowardly and criminal act. These teenagers believe that, by being mothers, they will not be alone and that motherhood may be the driving force that enables them to achieve their goals. Therefore, they resist opting for an abortion.
As for the second dimension, the participants in this study mount strong resistance to any kind of pressure. In some cases, it comes from the baby’s father and is influenced by a lack of security in terms of assuming paternal responsibility. There also is pressure exercised aggressively by adults other than the parents of the participants, as in the case of the partner’s adult relatives, who may attempt to exonerate or relieve him of any parental responsibility (Table 6).
Rebuilding support networks. Almost all the participants reported having some type of support when their primary network (parents) neglects to give them the support they need. In such cases, teenage girls cling to their partners or their mothers-in-law. In other cases, they take advantage of the support offered by friends.
Although virtually all the participants acknowledge having some kind of support, it is important to note that support is not always offered on acceptable terms with respect to quality. Occasionally, an offer of support is accompanied by some form of blackmail or conditioned in a way that implies increasing subordination for these girls. One aspect that stands out in this category is that some teenagers extol the support provided by the men around them (their sexual partner and the girl’s father). The father’s support gives them a sense of security they may not have experienced since early childhood. These forms of interaction reflect an effort to rebuild relationships that perhaps were cut short or ruined. On the one hand, this support helps to relieve a great deal of the tension created by the experience of unexpected pregnancy; on the other, it gives them tools to assume the pregnancy.
CENTRAL CATEGORY
A central category represents the main research topic. Its analytical power is based on the ability to bring together all the categories to arrive at an explanation of the whole (24). Ultimately, it focuses on interpreting the research topic and identifying the main issues with respect to pregnant teenagers.
A process that involves a series of sequential actions/interactions supports the theoretical framework. These evolve and occur at a given time and place, and change or sometimes remain the same in response to a situation or context (24).
The process is associated with the structure and aligned with the conditions surrounding the actions/interactions. In other words, as they change they provide feedback to the context and become part of the conditions that influence the next set of actions/interactions (24).
The central category, labeled Wanting to be pregnant… but not so soon, is the result of combining the seven categories that emerged from the collected data (Figure 1). Naturally, this central category responds to the hypothesis that is expected to emerge from the description of the pregnancy experience for these teens and an analysis of their narratives, based on the data that emerged from the interviews (31). Future research will very likely determine what parts of the concept "Wanting to be pregnant…but not so soon" apply or are valid for other groups of pregnant teenagers and what new concepts or hypotheses can be added to this initial conceptualization, to construct a substantive theory that specifically characterizes the phenomenon of teenage pregnancy.
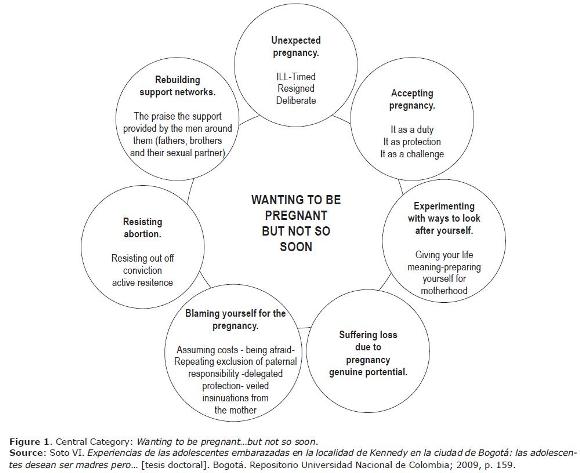
The central category uses the invariable word "but" to oppose the concept "wanting the pregnancy". The concept "not so soon" is associated with the concept of time. To contrast these two conditions it is important to note that in each of the categories they are seen as expressions and emotions. Therefore, we start with the concept of ambivalence as a highlight to show how the sequence of actions / interactions evolves in response to the context of the experience of pregnancy (30).
Ambivalence is one of the most relevant concepts to properly observe and understand modern and postmodern societies, a thorough understanding of problems that society today lives (29). From the language, ambivalence is described as linguistic correlate of the disorder, is deep sense of unease when unable to interpret the situation and to choose among alternative courses of action (30). In addition, ambivalence reveals when social consciousness arises that in all descriptions of our language are inclusions and exclusions, constitutes structure and disorder, establishing order and chaos (29).
That disorder evidenced in the pregnant teenagers for the constant use of expressions such as: " accident," "anger," "did not have basis," "not much," "not so," "fear," "believe," "you cannot do anything," "assimilated," "support," and of course "but"–experience recharged. Conflicting feelings such as anxiety and fear by recognizing not being ready and at the same time, feeling that was the opportunity that allowed them to mature.
When teenagers express feelings clashing between them, allow to support the first part of the central category Wanting pregnancy but…, through the categories "Unexpected pregnancy" with different variations in inopportuneness, resignation and deliberation, contemplating the desire for motherhood, running the risk and being surprised at facing an uncertain future, and Accepting the pregnancy, variations in accepting it as a duty that implies sacrifice. Even when it comes to themselves as a protective strategy that enables them to get their lives on track by avoiding alcohol and drugs, and as a challenge, defying the story of their lives in the sense of not wanting to repeat the abandonment and vulnerability experienced and, at the same time, preparing themselves for limitations.
Following with this inclusions and exclusions theme, the categories related with the consequences of continuing pregnancy emerge to support the second part of the central category ….Not so soon. Including time: Losses due to pregnancy vary between real and potential ones. Blaming themselves for the pregnancy as a side-effect of individualization Ways to take care of oneself: theory of distinction in relation to action.
Finally, Ambivalence is the driving force including the categories Resisting abortion given by religious and moral convictions and Support networks: provide comfort and relief.
CONCLUSIONS
The central category represents the main research topic and the proposed hypothesis, based on a process involving the actions/interactions of pregnant teens. The pregnant teenagers mother´s were aware their daughters had become sexually active, but chose to ignore the fact. The pregnant teenagers acknowledge having delegated ultimate responsibility for contraception to the man. The pregnant teenagers have limited autonomy with respect to their sexual and reproductive health.
During pregnancy, they absolve their sexual partner of any responsibility and even excuse him in a veiled or indirect way. They repeat the fate of women close to them, perhaps through oral transmission.
Challenge: how can nursing break this chain of events?
The physical changes during pregnancy are NOT significant. The important changes are social. They do not acknowledge or understand their bodies. A high proportion of teenagers (21%) are in their second pregnancy. Relationship with the father–pregnant teenager becomes more steady and established.–Room for nursing intervention.
CONTRIBUTIONS
Discipline: transform care from the traditional and standardized approach. A complex reality with no answer demands alternative solutions that include the context.
Practice: strategies for care related to social construction in function of the pregnancy. Need for schools to hire nurses who are experienced in working with teens. Urgently calls for innovative strategies to provide individualized and contextualized care and offer a model of nursing care for mothers and their teenage daughters
Research: on the epistemological debate to understand what the situation is like for pregnant teens. Replicate in future research for a more in-depth understanding of other similar groups.
REFERENCES
(1) Pulido S, Saldarriaga I, Escobar M. Proyecto educativo: Maternidad-paternidad como proyecto de vida de los adolescentes. Investigación educación en enfermería. 1998; 16(2): 89-107. [ Links ]
(2) Issler JR. Embarazo en la adolescencia. Revista de Posgrado de la Cátedra VI la Medicina. 2001; 107: 11-23. [Consultado 8 de abril de 2006]. Disponible en http://www.pediatria.org.ec/ bvs/2007/8.2.2007_full.pdf. [ Links ]
(3) Organización Panamericana de la Salud y Centro Latinoamericano de Perinatología. [Consultado el 10 de abril de 2009]. En: http://www.clap.ops-oms.org/web_2005/estadisticas% 20de%20la%20region/textos/e35%2068%20Embarazo%20 Adolescente.htm. [ Links ]
(4) Embarazos en jóvenes, Bogotá se acerca a Uganda. El Tiempo, sábado 16 de junio de 2007. [Consultado el 2 de febrero de 2009]. En: http://www.eltiempo.com/archivo/documento. [ Links ]
(5) Simões da Silva A et al. Characteristics of adolescent pregnancy in São Luis. Maranhão, Brazil. Revista de Saúde Pública 2003 [consultado el 30 de marzo de 2006] 37(5): 559-65.. En: http://www.fsp.usp.br/rsp [ Links ]
(6) Conde AA, Beltran JM, Lammers C. Maternal-perinatal morbidity and mortality associated with adolescent pregnancy in Latin America: Cross-sectional study. American Journal of Obstetrics and Gynecology. 2005; 192(2): 342-49. [ Links ]
(7) Eure C, Lindsay M, Graves W. Risk of adverse pregnancy outcomes in young adolescent parturients in an inner-city hospital. American Journal of Obstetrics and Gynecology. 2002; 186(5): 918-20. [ Links ]
(8) Bacon J. Adolescent sexuality and pregnancy. Current Opinion in Obstetrics and Gynecology. 2000; 12(5): 345-47. [ Links ]
(9) Lenders C et al. Nutrition in adolescent pregnancy. Current Opinion in Pediatrics. 2000; 12(3): 291-96 [ Links ]
(10) Olausson P, Cnattingius S, Haglund B. Teenage pregnancies and risk of late fetal death and infant mortality. Obstetrical & Gynecological Survey. 1999; 54(8): 484-85. [ Links ]
(11) Foster H Jr. et al. Teen pregnancy-problems and approaches: Panel presentations. American Journal of Obstetrics and Gynecology. 1999; 181 (Suppl 1): 32-6. [ Links ]
(12) Merritt V. Young, Poor, and pregnant: The psychology of teenage motherhood. Journal of the American Academy of Child & Adolescent Psychiatry. 1996; 35(2):256-57. [ Links ]
(13) Ministerio de la Protección Social, Dirección General de Salud Pública. Política Nacional de salud sexual y reproductiva; 2003. [Consultado el 23 de julio de 2008]. En:http:// www.minproteccionsocial.gov.co/acercaMinisterio/Paginas/ Pol%C3ADticasformuladasporelMinisteriodelaProtecci%C3 %B3nSocial.aspx. [ Links ]
(14) Feldmann J, Middleman A. Adolescent sexuality and sexual behavior. Current Opinion in Obstetrics and Gynecology. 2002; 14(5) 489-93. [ Links ]
(15) Foster H Jr, Keynote address: Taming the tempest of teen pregnancy. American Journal of Obstetrics and Gynecology. Julio, 1999; 181 (Suppl 1): 28-31. [ Links ]
(16) Hogan DP, Sun R, Cornwell GT. Sexual and fertility behaviors of American females aged 15-19 years: 1985, 1990, and 1995. American of Journal Public Health. 2000; 90(9): 1421-1425 [ Links ]
(17) Drescher KM, Monga M, Williams P. Promecene-Cook, P, Schneider K. Perceived quality of life in pregnant adolescent girls. American Journal of Obstetrics and Gynecology. 2003; 188(5): 1231-1233. [ Links ]
(18) Omar H, Richard J. Cultural sensitivity in providing reproductive care to adolescents. Current Opinion in Obstetrics and Gynecology. 2004; 16(5): 367-70. [ Links ]
(19) Meed GH. Movements of thought in the nineteenth century. In: Moore M H. editor. Reed Book. The Internet encyclopedia of philosophy. Chicago. 2007. [consultado el 30 de abril de 2008]. En: http://www.iep.utm.edu/1/about.htm Chicago. [ Links ]
(20) Miranda M. Pragmatismo, interaccionismo simbólico y trabajo social. De cómo la caridad y la filantropía se hicieron científicas. (Tesis doctoral). Tarragona. Universitat Rovira i Virgili; 2003. [ Links ]
(21) Reposo A, Valencia M. Actitudes posmodernas frente al positivismo. Consecuencias metodológicas. Diseño Urbano y Paisaje. 2004; 1(2): 21-42. [Consultado el 8 de abril de 2009]. En http://www.ucentral.cl/Sitio%20web%202003/ Revista% 20Farq/02.htm [ Links ]
(22) Fassinger Ruth E. Paradigms, Praxis, Problems, and promise: Grounded theory in counseling psychology research. Journal of Counseling Psychology. 2005; 52(2) 156-66. [ Links ]
(23) Banister P, Burman E, Parker I, Taylor M. Métodos cualitativos en Sociología. Una guía para la investigación. Guadalajara. Universidad de Guadalajara, centro Universitario de Ciencias de la Salud; 2004. [ Links ]
(24) Strauss A, Corbin J. Bases de la investigación cualitativa, técnicas y procedimientos para desarrollar la teoría fundamentada. Medellín. Universidad de Antioquia. 2002. [ Links ]
(25) Rentschler D. Pregnant adolescents' perspectives of pregnancy. American Journal of Maternal Child Nursing. 2003; 28(6): 377-383. [ Links ]
(26) Whitehead E. Teenage pregnancy: On the road to social death. International Journal of Nursing Studies. 2001; 38(4): 437-446. [Consultado el 20 de abril de 2005]. En: http://www.ncbi.nlm.nih.gov/sites/entrez. [ Links ]
(27) Freud S. Civilization and its discontents. En: Garland D. Castigo y sociedad moderna un estudio de teoría social. Barcelona. XXI editores; 1999. [ Links ]
(28) Mngadi P, et al. Quality of maternity care for adolescent mothers in Mbabane, Swaziland. International Nursing Review. 2002; 49(1): 38-46. [ Links ]
(29) Bauman Z. El concepto de la ambivalencia y la metodología de las distinciones. En: Beriain J; Iturrate J. editores. Para comprender la teoría sociológica; 1998. [ Links ]
(30) Bauman Z. Modernidad y ambivalencia. En: Beriain J. compilador. Las consecuencias perversas de la modernidad. Barcelona: Anthropos; 1996, pp. 73-119. [ Links ]
(31) Soto VI. Experiencias de las adolescentes embarazadas en la localidad de Kennedy en la ciudad de Bogotá: las adolescentes desean ser madres pero... [tesis doctoral]. Bogotá. Repositorio Universidad Nacional de Colombia; 2009, p. 159. [ Links ]
(32) Husserl E. Ideas relativas a una fenomenología pura y una filosofía fenomenológica. 2.a ed. México. Fondo de Cultura Económica; 1993. [ Links ]
(33) Simmons H. Philosophic and scientific inquiry: The interface. En: Kikuchi J, Simmons H. Philosophic inquiry in nursing. Newbury Park, SAGE Publications; 1992, pp. 9-25. [ Links ]
(34) Caru A, Cova. Revisiting Consumption Experience: A More Humble but Complete View of the concept. Marketing Theory. 2003; 3(2), 269. [Consultado el 15 de junio de 2008] En: http://www.sagepublications.com. [ Links ]
(35) Monti E, Tingen M. Multiple paradigms of nursing science. Advances in Nursing Science. 1999; 21(4): 64-80. [ Links ]
(36) Blumer H. Symbolic interactionism as defined by Herbert Blumer. The Society for More Creative Speech, 1996. [consultado el 15 de marzo de 2007]. En: http://www.cdharris.net/text/blumer.html. [ Links ]
(37) Blumer H. Interaccionismo simbólico: perspectiva y método. Berkeley. University of California Press; 1982. Citado por Miranda, p. 260. [ Links ]
(38) Joas H. Interaccionismo simbólico. En: Giddens A, Turner, J, et al. La teoría social hoy. Barcelona: Alianza Editorial; 1990, p. 117. [ Links ]
(39) Charmaz K. Constructing grounded theory. London. Sage Publications; 2006. [ Links ]
(40) Hutchinson S. Grounded theory: The method. En: Munhall P, Oiler C. Nursing Research. A qualitative perspective. Connecticut. Appleton-C; 1986, pp. 111-30. [ Links ]
(41) Chenitz C, S.. Qualitative research using grounded theory. En: Chenitz C, S. From Practice to Grounded Theory. Qualitative research in nursing. California. Addison Wesley Publishing Company; 1946, pp. 3-15. [ Links ]
(42) Goulding C. Grounded theory: A practical guide for management, Business and market researchers. London. Sage Publications; 2002. [ Links ]
(43) Strubert H, Carpenter D. Qualitative research in nursing. Advancing the humanistic imperative. 2.a ed. Philadelphia. Lippincott; 1999, p. 331. [ Links ]
(44) Trentini M, Paim L.. Pesquisa convergente assistencial: um desenho que une o fazer e o pensar na prática assistencial em saúde-enfermagem. 2 ed. Insular. Citado por Mota MF. Cuidado humaniza no prè-natal: Um olhar para além das divergências e convergências. Universidad Federal de Santa Catarina; 2006, p. 209. [ Links ]

