










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAvances en Enfermería
Print version ISSN 0121-4500
av.enferm. vol.33 no.1 Bogotá Jan./April 2015
https://doi.org/10.15446/av.enferm.v33n1.47855
http://dx.doi.org/10.15446/av.enferm.v33n1.47855
Atypical nature of coronary artery disease in women: a proposal for measurement and classification
Atipicidad en la mujer con enfermedad coronaria: propuesta de medición y clasificación
Atípica em mulheres com doença cardíaca coronária: medição e proposta de classificação
Viviana Marycel Céspedes Cuevas1
1 Doctora en Enfermería. Profesora Asociada, Facultad de Enfermería, Universidad Nacional de Colombia. Bogotá, Colombia. E-mail: vmcespedesc@gmail.com, vmcespedesc@unal.edu.co
Recibido: 20/09/2011 Aprobado: 15/12/2014
Abstract
Objective: To identify subgroups of women with Acute Coronary Syndrome according to symptom experience: perception, evaluation and response, based on the Symptom Management Conceptual Model.
Methodology: Quantitative, descriptive, exploratory, cross-sectional study. The sample was made of 380 women positively diagnosed with Acute Coronary Syndrome, hospitalized in two institutions in Bogotá, Colombia. A measurement instrument was designed and validated.
Results: Final instrument was made of 37 items that reported content validity, scale validity, discriminant validity, and construct validity. A Cronbach's Alpha coefficient of 0,76 was obtained, which guarantees homogeneity in the measurement according to the Maximum Validity-Maximum Reliability Model. A total of 11 subgroups of women with Acute Coronary Syndrome were identified, those were characterized by atypical coronary heart disease symptomatology, evaluation processes related to extra-cardiac causes and inadequate symptom management strategies. It was possible to demonstrate that psychosocial factors, previous coronary heart disease and delays were variables making a significant influence on the components of symptom experience.
Conclusions: Women with Acute Coronary Syndrome, belonging to the 11 subgroups that were identified and studied, showed atypical symptoms. The instrument designed features a proven psychometric quality; it was valid, reliable, and useful for clinical research and practice.
Descriptors: Scales; Coronary Disease; Women's Health (source: DeCS BIREME).
Resumen
Objetivo: Identificar subgrupos de mujeres con Síndrome Coronario Agudo según la experiencia del síntoma: percepción, evaluación y respuesta, a partir del Modelo Conceptual del Manejo del Síntoma.
Metodología: Estudio cuantitativo, descriptivo, exploratorio, transversal. La muestra fue de 380 mujeres con diagnóstico confirmado de Síndrome Coronario Agudo, hospitalizadas en dos instituciones de la ciudad de Bogotá, Colombia. Para la recolección de la información se desarrolló un instrumento de medición validado.
Resultados: El instrumento final constó de 37 ítems que reportaron validez de contenido, validez de escala, validez discriminante y de constructo. Se obtuvo un Coeficiente de Alpha de Crombach de 0,76, el cual garantizó homogeneidad en la medición de acuerdo con los valores de referencia del Modelo de Máxima Validez-Máxima Confiabilidad. Se identificaron 11 subgrupos de mujeres con Síndrome Coronario Agudo, caracterizados por sintomatología atípica de enfermedad coronaria, procesos de evaluación relacionados con orígenes extra-cardíacos y estrategias inadecuadas de manejo de los síntomas. Se evidenció que los factores psicosociales, la enfermedad coronaria previa y los tiempos de demora fueron variables influyentes sobre los componentes de la experiencia del síntoma.
Conclusiones: Los 11 subgrupos identificados evidenciaron atipicidad en las mujeres estudiadas con Síndrome Coronario Agudo. El instrumento desarrollado obtuvo una calidad psicométrica demostrada; fue válido, confiable y útil para la investigación y la práctica clínica.
Descriptores: Escalas; Enfermedad Coronaria; Salud de la Mujer (fuente: DeCS BIREME).
Resumo
Objetivo: Identificar os subgrupos de mulheres com Síndrome Coronariana Aguda na experiência da percepção dos sintomas, avaliação e resposta, do Modelo Conceitual da Gestão Sintoma.
Metodologia: Estudo quantitativo, descritivo, exploratório e transversal. A amostra incluiu 380 mulheres com diagnóstico de Síndrome Coronariana Aguda confirmada, e hospitalizadas em duas instituições da cidade de Bogotá, Colômbia. Para a coleta de dados, um instrumento de medição foi desenvolvido.
Resultados: O instrumento final foi composto por 37 itens que relatam a validade de conteúdo, validade da escala, discriminante e validade de construto. Um coeficiente de Cronbach Alpha de 0,76, o que garante a consistência na medição de acordo com os valores de referência do Modelo Validade de alta confiabilidade elevada foi obtida. Nos 11 subgrupos de mulheres com Síndrome Coronariana Aguda, caracterizados por sintomas atípicos de doença coronária, foram identificados processos de avaliação relacionados com extra-cardíacas e inadequadas estratégias de gerenciamento de origens e sintomas. Era evidente que os fatores psicossociais, doenças coronárias e atraso em vezes anteriores, foram variáveis influentes sobre os componentes da experiência do sintoma.
Conclusões: Os 11 subgrupos identificados mostram atípica estudada em mulheres com Síndrome Coronariana Aguda. O instrumento desenvolvido provou qualidade psicométrica, válido, confiável e útil para a pesquisa e a prática clínica.
Descritores: Escalas; Doença das Coronárias; Saúde da Mulher (fonte: DeCS BIREME).
Introduction
Current research topic is about cardiovascular nursing and phenomenon under study is Symptom Experience. From a perspective of the importance of field, cardiovascular healthcare system has focused on the needs of male gender for making decisions dealing with diagnose, treatment and treating patients with cardiovascular diseases (1). In most research studies, women have been considered as a mini-man, therefore results of those investigations carried out in men have been extrapolated to women (2). This is due to the fact that women are believed to be less prone to cardiovascular disease. As a result, nursing in the cardiovascular field has been unaware of the importance of gender related issues, which makes difficult to deal with and treat on time the symptoms of Acute Coronary Syndrome (ACS) in female population (3).
Current study has a holistic approach to symptom treatment. It pays special attention to the person, symptom perception, its evaluation, and the range of possible treatments that should be started as a response, instead of what nurses think are the most urgent needs to be found as a result of what they know about the patient's pathology. Approach of the symptoms gives nurses opportunity to become competent in dealing with them helped by an approach that promotes search of creative ways to understand and appreciate the experience of ACS in women.
From the perspective of social impact of this study, it deals with worldwide epidemics (4). According to statistics, one person dies every minute from coronary disease in the world (5). It is impossible to understand whether anyone has in mind that this disease can be prevented to a large extent.
As to knowledge contribution, research in the field has always focused on the waiting time. The current study aims to understand complex behavioral phenomenon that precedes consultation (6, 7, 8, 9, 10, 11, 12). Also, this work makes a contribution to the basic elements in psychometrical research and theoretical verification of the Symptom Management Conceptual Model (SMC) (13). These items make the present work a relevant and original clinical study that promotes qualification of nursing and generates a significant social and research contribution to the field of cardiovascular studies.
Research question
Which are the women subgroups with Acute Coronary Syndrome according to symptom perception, evaluation and response?
General objective
To identify women subgroups with Acute Coronary Syndrome according to symptom management: perception, evaluation and response, on the basis of the Symptom Management Conceptual Model.
Conceptual framework
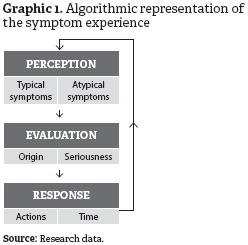
The SMC, developed by the Faculty of Nursing in the University of California, San Francisco, is foundation for this study. Such model states that symptoms must be studied as "subjective experiences that reflect changes in the bio-psychosocial functioning, sensations or cognition of an individual (13)".
This model studies three dimensions: symptom experience, strategies of symptoms management, and symptoms results. Also, it is based on the interaction of these three dimensions. It also states that such three dimensions depend on context external variables.
First dimension is Symptom experience. This has been thoroughly studied in the current research. Graphic 1 presents the algorithmic representation. It includes the individual's perceptions of symptoms, the evaluation of the meaning of symptoms and its response. These have a bidirectional relationship between them as well as with the environment.
Materials and Methods
Current investigation was cross-sectional, quantitative, descriptive and exploratory. A group of women older than 20, who were diagnosed with ACS —those with evidence of more than 75% of injuries demonstrated for cardiac catheterization— and without complications was studied. This study had three phases: pilot pre-test, pilot test and main study. The study was carried out in cardiology service, intensive care units and chest pain units of two institutions in Bogotá, Colombia.
Despite the fact that this is a cross-sectional study, phenomenon under study was an event located in the past. For this reason, one of the threat factors which were identified in the study can be known as maturation (14). Also, another threat factor for this study could be possibility of a decrease in remembering original experience. This risk was lowered by choosing women who were hospitalized due to Acute Myocardial Infarction (AMI) or unstable angina.
Technological tools and programs for processing and analyzing data were: SPSS (Statistical Product and Service Solutions) and AMOS (Analysis of Moment Structures). Sampling was purposive. It was made up of women who fulfilled the requirements of inclusion and hospitalized in chosen institutions from March 2007 to August 2008.
A modification of sample size determination for Finite Population Model (15) was used to estimate sample size. In this model, standard deviation was used in order to calculate approximated error of the Population Mean (K). Variant proposed with this formula has the advantage that it is not required to consider the standard deviation as coming from a proportion. In addition to that, it is not necessary to know such proportion. Sample size for the pilot test was 81, (0,2 error, acceptable). For final study, sample was 380, (0,05 error, optimum). It was calculated from the standard deviation of the pilot test.
Research tool used was validated since there were not any assessment systems for the phenomenon under study and its original version had 76 items with dichotomous answers. 33 of them measured Perception in two subcategories named Typical and Atypical symptoms, 14 measured Evaluation in two subcategories named Origin and Seriousness, finally 29 measured Response in two subcategories named Management and Waiting time.
Framework analysis
The analysis processes for each of phases were as follows:
Content validity: it was calculated through an agreement between four expert nurses based on their cognitive competence and existing procedures in cardiovascular nursing field. Agreement between judges was reached by applying the Modified Lawshe's Content Validity Ratio (CVR) (16, 17) using a scale from 1 to 3. 1 was considered necessary, 2, useful but not important, and 3, unnecessary. Among panelists it was agreed that items exhibiting CVR' ≥ 0,58 were the only ones accepted.
Scale validity: it was made by creating graphics and an interpretation of the items means according to each one of the theoretical dimensions —perception, evaluation and response—. Scale validity was analyzed based on Wright & Stone interpretation (18). It was used to focus the study on the quality of the theoretical criterion that supports the scale. A graphic was used to evaluate the quality of the scale validity. It represents items that are part of each dimension in the questionnaire in a map "p vs. item number". They are ordered from positive to negative in relation to p —average of positive answers in each item—. If there is a perfect scale, all items should be aligned in straight line that goes from lower p = 0,2 to upper p = 0,8.
Construct and discrimination validity: it was useful for the identification of item clusters. It was done through:
-
Analysis of discrimination validity by item-total correlation (point biserial correlation). It aims at identifying sets of items that measure different features and have consistency in the group. However, they are not correlated to other features that are measured by other sets of items. Three different sets were created depending on the fact that they had positive correlation, negative correlation or low correlation (lower than 0,196) (19).
-
Identification of item clusters using factor analysis. Method applied was Principal Components Analysis (PCA), as well as Varymax method of data rotation, in order to make interpretation easier. All factorial loads higher than ±0,35 (17) were selected. The procedure used to select items in each factor, where the loading was 2 or more factors, was selecting the item in the factor with higher loading (closer to 1 or –1) and a mathematical difference of factorial load above 0,01 in relation to the rest of the factors.
-
Mixture of groupings found using total-item correlational analysis and factor analysis. The group-ings were created by simple mixture technique.
-
Construction of the multitrait-multimethod matrix. Based on Campbell and Fiske's proposal (21), it was developed a matrix that aimed at verifying construct and discriminant validity of the instrument used in the current study. Because of it, high inner dimension correlations were required as evidence of construct validity and low inter dimensional correlations when the traits are considered to be different and there was discriminant validity.
Reliability
Internal consistency and tool stability were estimated. Internal consistency was calculated by Cronbach's Alpha Coefficient (22, 23) in relation to the reference values of the maximal reliability-maximal validity model (24, 25) in each grouping identified and in total test. Stability was estimated by applying a test and re-test the third day of first measurement in those women who consented and who did not show new experiences of the Acute Coronary Syndrome symptoms during hospitalization. For this purpose, Pearson correlation coefficient was used.
Results
Table 1 presents main results of the research.
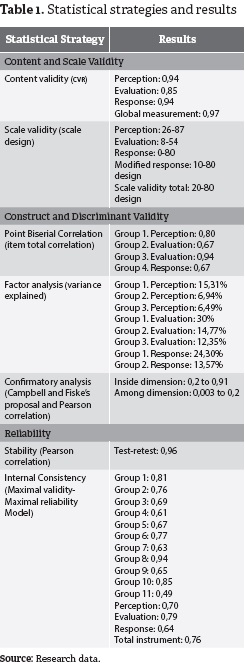
Content validity: Results showed that the content validity index for instrument of global measurement was 0,97. For each scale, estimation was 0,94 for perception, 0,85 for evaluation, and 0,94 for response. These values indicate that items are representative units of analysis of elements such as perception, evaluation and response to symptoms that were to be measured. In spite of the fact, 7 items showed content validity index 0,5 —according to the criterion, it would make them be left out—, it was decided that they were going to still being part of the instrument because in the pre-pilot test such items were significant in women with Acute Coronary Syndrome.
Scale validity: It was used to know objectively if the distribution of the items in each one of the theoretical dimensions matched a certain external theoretical criterion. If there was a perfect scale, all items had to be aligned in a straight line —20-80, which are theoretically, suggested values—. When items in questionnaire were far from straight line distribution, it was called into question whether it was or not a variable that defined a scale.
Results displayed that components perception and evaluation showed a behavior scale in contrast to components response that behaves like a non-scale component, due to that behavior of response component an analysis on the nature of items was carried out. This showed that 58 out of 75 were non-scale items. For these reasons, it was decided to eliminate these 18 items from the tool so that they could be analyzed as contextual items.
The item distribution in component response was modified (11 items) in new tendency line, which makes adjustments in a 10-80 design. After changing to the third component, it can be stated that each of three theoretical components has an independent measurement scale. Three components in just one scale showed that instrument with 58 items fits in the 20-80 linear model design. Based on this, it can be said that a scale of measurement was created for symptom experience with its three components —perception, evaluation and response— in independent scale.
Construct and discriminant validity
Based on Point Biserial Correlation. 4 groupings were obtained: 1 for perception, 2 for evaluation —origin and seriousness— and 1 for response, which is confirmed by the original structure of the Symptom Management Conceptual Model.
Based on factor analysis. 8 groupings were obtained: 3 for perception, 3 for evaluation, and 2 for response.
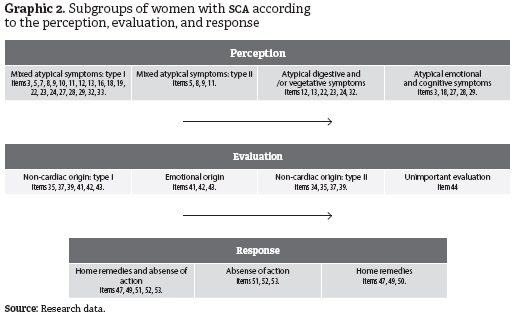
Mixing of groups. By mixing groups identified by the total-item correlation and factor analysis, the following groups were obtained (see Graphic 2):
-
4 groups for perception characterized by the presence of atypical symptoms. 2 groups were mixed atypical symptoms, 1 group with atypical digestive and/or vegetative symptoms, and 1 with atypical emotional and cognitive symptoms.
-
4 groups for evaluation characterized by evaluation with a non-cardiac origin and unimportant seri- ousness. 2 groups showed with evaluative process with non-cardiac origin, 1 group with emotional origin, and 1 group with unimportant evaluation.
-
3 groups of response were characterized by inadequate actions such as the use of home remedies and absence of action.
Another important finding was that there was warranty of discriminant and construct validity, as well as the presence of 11 groups for perception, evaluation, and response of women with Acute Coronary Syndrome, which were useful to direct practice. It is worth highlighting that there were four items left out in the process of building the groups. Such items did not fulfill the requirements of discriminant and construct validity.
Confirmatory analysis. Based on Campbell and Fiske's proposal, a matrix was developed. It aimed at corroborating construct and discriminant validity. For that, high intra dimension correlations were demanded as evidence of construct validity and low inter dimension correlations as evidence of discriminant validity.
High Pearson correlations can be seen (higher than 0,196) inside each theoretical component, which is evidence of construct validity. In the same way, low Pearson correlations are low (lower than 0,196) among different theoretical components. This shows presence of discriminant validity.
Reliability. Stability and internal consistency were estimated. Stability was calculated by applying a test-retest the third day after first measurement in those women who consented and who did not show new experience of the symptoms of Acute Coronary Syndrome during hospitalization. Stability in items of the instrument was calculated with Pearson correlation coefficient 0,96. Perfect correlation between pre-test and post-test was proven.
Internal consistency was estimated by means of calculating the Alpha Crombach's coefficient taking into account the reference values of Maximal Validity-Maximal Reliability Model in each of identified groups and in total test.
As to reliability per grouping (from 0,5 to 0,94), per theoretical dimension (from 0,64 to 0,70) and total one from original instrument (0,76), it can be stated that it fits in the reference values of the Maximal Validity-Maximal Reliability Model. This displays the optimum internal consistency or homogeneity in measurement.
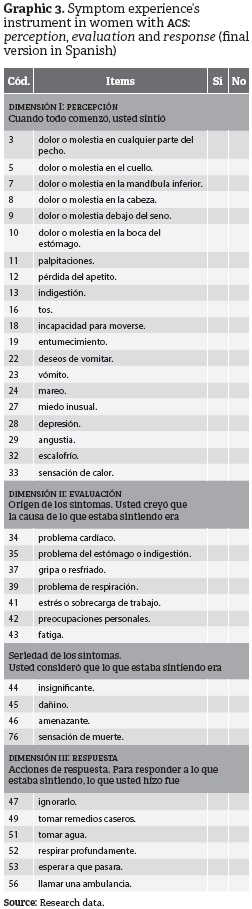
Maximal Validity-Maximal Reliability Model allowed evaluation of reliability required based on a determined validity. This avoids metric redundancy, which can be generated when increasing the length of tests. Final instrument was made up of 37 items: 20 about perception, 11 about evaluation and 6 about response (see Graphic 3).
Conclusions and Contributions
Methods. Creating instrument for the project was an important result from research. For this, a series of methodological strategies were used, those aimed at looking for warranties of validity and reliability so that it could be applied. Analyzing this study from measurement, it can be said that a valid, objective, reliable and a high quality instrument was designed.
Theory. By using same strategies for creating instrument and assuring construct and discriminant validity, 11 groupings of women with ACS were created. That made possible to understand different types of perception, evaluation and response to symptoms. These findings showed to nursing area that:
-
The so-called atypical symptoms become the typical ones in the female gender.
-
Heart attacks in women are not properly identified.
-
Women can assume self-care behavior; can also seek for professional assistance or not to take any self-care behavior at all when ACS symptoms appear.
-
Women try to create a hypothesis about their symptoms and to minimize them; that might increase the waiting time.
Women subgroups with ACS —based on three elements of symptom experience— are a tool to redirect nursing practice.
From nursing area. Results of this research generate a revolution in cardiovascular nursing, specifically in evaluation, classification systems and education settings. With products of the research there is a new opportunity for change, since more accuracy can be given to the measurement of the phenomenon. This provides valid and reliable evaluations to identify seriousness of classification systems and identification of education issues that can be adjusted to real needs.
A transformation in basic semiology of cardiovascular nursing will be source of deep changes, not only in evaluation and consequent diagnose treatment and prognosis of women with Acute Coronary Syndrome, but also in redirecting the contents of education. These possibilities open new opportunities to have a more specific, relevant and pertinent nursing to women with coronary disease.
References
(1) Shirato S, Swan BA. Women and cardiovascular disease: an evidentiary review. Medsurg Nurs. 2010;19(5):282-286. [ Links ]
(2) Gallegher R, Marshall AP, Fisher MJ. Symptoms and treatment-seeking responses in women experiencing acute coronary syndrome for the first time. Heart Lung. 2010;39(6):477-488. [ Links ]
(3) Carter LW, Ski C, Scruth E, Campbell M, Page K. Systematic review of cardiovascular disease in women: assessing the risk. Nurs Health Sci. 2011 Dec;13(4):529-535. [ Links ]
(4) Emslie C. Women, men and coronary heart disease: a review of the qualitative literature. J Adv Nurs. 2005;51(4):382-395. [ Links ]
(5) Alfonso F, Bermejo J, Segovia J. Enfermedades cardiovasculares en la mujer: ¿por qué ahora? Rev Esp Cardiol [revista en Internet]. 2006 [acceso:17 sep 2009];59(3):[aprox. 4 p.]. Disponible en: http://www.revespcardiol.org/es/enfermedades-cardiovasculares-mujer-por-que/articulo/13086083/. [ Links ]
(6) Turris SA. Women's decisions to seek treatment for the symptoms of potential cardiac illness. J Nurs Scholarship. 2009 Mar;41(1):5-12. [ Links ]
(7) Burnett RE, Blumenthal JA, Mark DB, Leimberger JD, Califf RM. Distinguishing between early and late responders to symptoms of acute myocardial infarction. Am J Cardiol. 1995;75(15):1019-1022. [ Links ]
(8) Dracup K, Moser DK, McKinley S, Ball C, Yamasaki K, Kim CJ et al. An international perspective on the time to treatment for acute myocardial infarction. J Nurs Scholarship. 2003;35(4):317-323. [ Links ]
(9) Rosenfeld AG. Treatment-seeking delay among women with acute myocardial infarction: decision trajectories and their predictors. Nurs Res. 2004;53(4):225-236. [ Links ]
(10) Askham J, Kuhn L, Frederiksen K, Davidson P, Edward KL, Worral L. The information and support needs of Faroese women hospitalised with an acute coronary syndrome. J Clin Nurs. 2010 May;19(9-10):1352-1361. [ Links ]
(11) DiGiacomo M, Davidson PM, Zecchin R, Lamb K, Daly J. Caring for others, but not themselves: implications for health care interventions in women with cardiovascular disease. Nurs Res Pract. 2011;2011:1-5. [ Links ]
(12) Kling JM, Miller VM, Mankad R, Wilansky S, Wu Q, Zais TG et al. Go red for women cardiovascular health-screening evaluation: the dichotomy between awareness and perception of cardiovascular risk in the community. J Womens Health. 2013 Mar;22(3):210-218. [ Links ]
(13) Dodd M, Janson S, Facione N, Faucett J, Froelicher ES, Humphreys J et al. Advancing the science of symptom management. J Adv Nurs. 2001;33(5):668-676. [ Links ]
(14) Polit D, Hungler B. Investigación científica en ciencias de la salud. 6ª ed. México D.F.: Mc Graw Hill; 2000. [ Links ]
(15) Tristán LA. Cálculo del tamaño de muestra y establecimiento de criterios y el problema del tamaño de la población. Guía de usuario Kalt Criterial®. México D.F.: Instituto de Evaluación e Ingeniería Avanzada San Luis Potosí; 2003. [ Links ]
(16) Lawshe CH. A quantitative approach to content validity. Pers Psychol. 1975;28(4):563-575. [ Links ]
(17) Tristán LA. Modificación al modelo de Lawshe para el dictamen cuantitativo de la validez de contenido de un instrumento objetivo. Av Med. 2008;6(1):37-48. [ Links ]
(18) Wright BD, Stone MH. Making measures. Chicago: The Phaneron Press; 2004. [ Links ]
(19) Tristán LA, Vidal UR. Manual de fórmulas de correlación: Correlación punto-biserial. Victoria: Trafford; 2006. [ Links ]
(20) Cea MA. Análisis multivariable: teoría y práctica en la investigación social. Madrid: Editorial Síntesis; 2002. [ Links ]
(21) Campbell DT, Fiske DW. Convergent and discriminant validation by the multitrait-multimethod matrix. Psychol Bull. 1959 Mar;56(2):81-105. [ Links ]
(22) Cronbach LJ, Shavelson RJ. My current thoughts on coefficient Alpha and successor procedures. Educ Psychol Meas. 2004 Jun;64(3):391-418. [ Links ]
(23) Barragán JA, Manrique FG. Validez y confiabilidad del SERVQHOS para enfermería en Boyacá, Colombia. Av Enferm. 2010;28(2):48-61. [ Links ]
(24) Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951 Sep;16(3):297-334. [ Links ]
(25) Céspedes VM. Síntomas en la mujer con síndrome coronario agudo: desde las pruebas de validez. Av Enferm. 2012;30(2):25-38. [ Links ]
