











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
It is estimated that there are about 382 million of people with diabetes mellitus (DM) nowadays, and that in 2035 this number will reach 471 million. In the 21st century, DM will be responsible for about 5.2% of deaths worldwide, becoming the fifth leading cause of mortality. Absence or insufficiency of information, as well as lack of skills necessary to live with the disease, are causes related to complications and deaths. In this sense, educational actions are highlighted for the care of DM patients and their families 1.
Many educational intervention designs based on theory, traditional or innovative practice references have been implemented in educational practice for people with DM and their families. It is observed that the intention of teaching and educational health strategies should subsidize diagnostics, in a trial to meet demands, to favor the teaching-learning process, and to generate consistent results for clinical adherence and disease control 2-3.
In this perspective, a multidisciplinary group developed Self-Management Education for Diabetes, based on international standards for the development of educational projects supported on self-management skills and self-care, based on the concepts of health and pedagogy 4.The first is Dorothea Orem's Theory of Self-Care Deficit 5, based on five premises. The main ones for this study are: capacity, the possibility of performance acquired by the individual, and action, the practice of these activities 6. The second is the concept of empowerment that aims to enable people to learn, to develop their potentials, to live life in its different steps and to deal with the limitations imposed by possible diseases.
Attention to people with DM is a challenge for health professionals, and it is also necessary to develop and/or improve educational plans with a multidisciplinary approach that favors the development of multidimensional abilities in people, considering their socioeconomic and cultural characteristics. Presenting the possibilities of education programs to be developed with patients of health services, constitutes the motto of this investigation.
The educational program outlined in the present research proposes a dialogic relationship between health professionals and people with DM, seeking to integrate the demands for better diabetes care. This research aimed to evaluate the effect of an intervention program on capacity and action for the self-care of people with DM.
Methods
It is an interventional study through the implementation of a Diabetes Education Program (PED by its initials in Portuguese), evaluated at the beginning and after the follow-up of people with diabetes during the period from May 2008 to May 2009, for 12 months in a health institution in the city of São Paulo. The study project was submitted for the approval of the Research Ethics Committee of the Universidade Federal de São Paulo and obtained approval (CEP n° 0652/08). The ethical precepts for conducting research with beings were incorporated to carry out researches with human beings; they agreed to voluntarily participate in the program, signing the Free and Informed Consent Term.
The study sample consisted of a non-probabilistic choice, as individuals sought the program by spontaneous demand, that is, they wanted to participate in an education program for the control of DM.
In the first phase of the project, participants were selected, and 500 people with diabetes were identified, of whom 400 were not part of any educational program. The selection of this population occurred in an open event for 200 people who were supposed to sign up by phone. The criterion for choosing this sample was the order of registration, but there were only 80 people enrolled. The registered people were invited to participate in an event composed of four moments: initial screening, breakfast, educational lectures and a moment of explanation about the details of the PED. The steps that make up the CONSORT 7, assessed for eligibility, allocation, follow-up and analysis were adopted as guideline for the report of this research of educational intervention in diabetes, with emphasis on the self-care of the population.
They were informed that there would be a selection of participants according to the inclusion criteria: being over 18 years of age, having DM type 2, being associated with the agreement for more than one year, and being accompanied by a general practitioner or endocrinologist responsible for treatment. Exclusion criteria were: previously diagnosed diseases that could affect cognition, and chemical dependence.
After explaining and recruiting the participants to the PED, 50 people were considered eligible to be part of the study population. All eligible people were allocated for educational intervention. Of these, 41 proposed to participate in the follow-up of this investigation and some referred lack of interest. At the end of the 12 weeks, the program followed 23 participants.
The data collection design consisted of screening of filling out a questionnaire with general data of the participants and previous exams, measurement of fasting capillary blood glucose and blood pressure. All participants received an educational folder. After this stage, there were three lectures given by the interdisciplinary team of the program on healthy habits of life and DM with the following topics: diabetes and self-care, "eat or not eat, that's the question!!!" and physical activity.
The following variables in the study were analyzed: social (gender, age, race, education, occupation, place of birth and marital status), lifestyle (smoking and drinking habits), clinical (preexisting conditions, blood pressure, clinical assessment/lab exams including values of glycosylated hemoglobin (HbAiC), microalbuminuria, total cholesterol and fractions, triglycerides, medium glycaemia/ glycemic variability, body mass index (BMI), fat percentage, abdominal circumference (AC), blood pressure (BP), and physical activity).
In addition to the variables mentioned above, the following scales were applied (8): Scale for Assessing the Actions of Self-Care of the Person with Diabetes (ECAD), and Scale for Assessing the Actions of Self-Care of the Person with Diabetes (EAAD), both validated for Portuguese language with the Cronbach's alpha = 0.8513 and 0.8016, respectively. Each scale includes 30 items with values attributed to a Likert-type scale ranging from 1 to 5 points. The answers have a minimum of 30 and a maximum of 150 points. The higher scores, the better the capability and action for self-care of the person with diabetes 9-10. The ECAD aims to assess the knowledge of the diabetic individuals about their disease and self-care, and the EAAD focuses inassessing whether the diabetic individuals are able to put the knowledge into practice in the daily life. To compare the scales before and after the educational intervention, it was used the statistical test Cronbach's alpha to assess the variability. It was adopted the confidence interval of 95% (p < 0.05).
The design of the educational intervention was developed in a clinical setting for structured health services to provide care to participants and their families, with podiatric clinic for specific attention and amphitheatres to conduct group dynamics and lectures. The activities developed in the PED were based on the seven behaviors: activity, feeding, monitoring, medication, problem solving, healthy coping and risk reduction in Diabetes Education 11, and adapted to individual needs.
The 12-month PED propitiated at least two activities per month for each participant, alternated with the nursing team, nutritionist, podiatric and physical educator. Group dynamics, lectures, and physical activity were adopted. Participants received a descriptive educational manual to follow the content addressed during the activities and contacted the team.
In this first occasion, assessment scales for the capability and actions for self-care were used with the intention to know the individual needs, as well as the comparative learning analysis at the beginning and the end of the program.
A software helped to determine the glycemic profile and to verify the average glycemia of this first monitoring, as well as all the others conducted during the program period.
In the multiprofessional team consultations, we addressed the following themes: self-monitoring, diabetes concepts, healthy, fractioned and adequate diet to maintain a good glycemic control, acute and chronic complications, definition of the glycosylated hemoglobin and mean weekly glycemic profile, dental assessment, physical activity to conduct a plan of action adequate to each participant, and foot care. The patients periodically went to a specialized podiatric, and besides cutting nails, she provided guidance about feet care.
The PED ended with a review game of the addressed themes, with the re-assessment of the capability and action scales for self-care, and a questionnaire to evaluate the program.
The procedures of data analysis were performed from data collection of evaluation and evolution records, food reminders and scales applied. The data of the participants were stored in database with double typing and evaluation of expertise in the program Excel (Microsoft Office Excel 2007), enumerating the continuous and qualitative variables.
Results
The program started with 41 people and only 23 remained until the end of the study. The reasons for the discontinuation were: absence of the company, difficulties to participate in consultations due to work, personal issues, other serious health problems, participation in another quality of life program, distance from home and only two people (4.3%) mentioned to have addressed issues to follow the recommendations.
Table 1 shows the socio-demographic variables in absolute and relative frequencies, with the respective means and medians. For the age of 57.7 and 57 years, respectively, it is observed that most of the studied population were males, younger than 60 years, with completed superior education, retired, white and Brazilians.
Table 1 Socio-demographic characteristics of people with DM, participating in the PED, São Paulo, Brazil, 2010
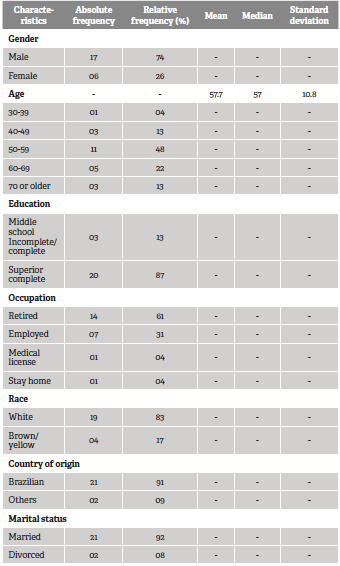
Source: primary data from PED.
Regarding the clinical characteristics, 16 (70%) participants were diagnosed in less than ten years; regarding comorbidities, 15 (65%) participants were hypertensive, five (21%) had some heart disease, 12 (52%) had other diseases, and four (17%) were smokers.
When analyzing people before and after the educational process, it was observed, regarding the metabolic control, the glycosylated hemoglobin and glycemic variability values statistically significant between the beginning and the end of the program (Table 2).
Table 2 Mean values and their respective standard deviations related to the glycemic control of people with DM, integrating the PED. São Paulo, Brazil, 2010
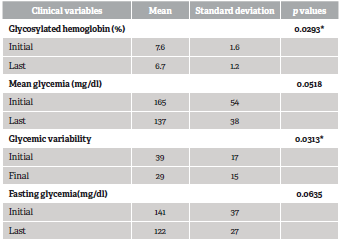
Source: primary data from PED.
Regarding the clinical variables, the laboratory parameters used did not show differences statistically significant when comparing before and after one year of accompaniment. Regarding the kidney function control assessed by the microalbuminuria, parameters indicating regular rates were found.
When analyzing the blood pressure results, we observed that the diastolic blood pressure variation was significant (p = 0.0077) between the observation periods. Regarding the physical activity, we verified that 12 people (53%) initially practiced some activity, and at the end this number increased to 19 (83%).
The anthropometric variables (BMI and AC) did not reveal differences, but when the percentage of participants regarding the BMI was analyzed, we observed a substantial migration of classes. This canbe seenin Graph 1.
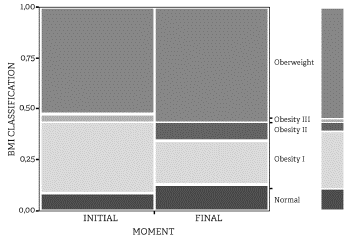
Source: primary data from PED.
Graph 1 BMI classification of people with DM, integrating the PED. São Paulo, SP, Brazil, 2009
It was found that both scales obtained positive results from the PED. When analyzing the questionnaires in detail, we verified improvement in the ECAD scores for 53% of the people when comparing the before and after moments. Note that on the scale measuring action for self-care, this improvement was 73%.
The data point a difference between initial and final capability and action (p = 0.0002; mean = 108.6 for actions and 125.6 for capability; p = 0.0389; mean = 133.3 for actions and 140.7 for capability, respectively). Comparing the initial and final values between capability and action, we verified a difference of 17 points (11%) at the beginning and 7.4 points (5%) at the end, demonstrating an isolated improvement in capability and action, that is, a score increase of 6% of the execution of what the individual can perform (Table 3).
Table 3 Scores of self-care capabilities and actions of people with DM, integrating the PED. São Paulo, SP, Brazil, 2010
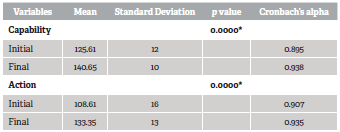
Source: primary data from PED.
About the time since the diabetes diagnosis, it was verified that when the cut-point was of 10 years, it was not observed any difference in capability/ action. But when the variable was categorized for five years, action scores presented significant differences, that is, verified a larger increase (1.7 points) for actions than for the capabilities for self-care at the final phase of the program (p = 0.0146).
Discussion
The reduced number of individuals that signed up to participate in the PED and the considerable loss of participants during the investigation resulted in a challenge to understand the interest and availability of diabetic people to take part in educational programs. Other studies with long-term accompaniment found that 63% to 85% of participants finished the programs, highlighting healthy elderly without depression when compared to those who did not finish them 11-15.
It was possible to detect loss of participants in this study related to gender, education, personal cost to participate in the educational program, difficulties in adhering to proposed recommendations for the disease control, preference for individual accompaniment with a physician of their choice. Therefore, although problematic, the participation in the educational program does not guarantee the user's participation 2,16.
Men majorly composed the investigated population, aged between 50 and 59 years, white, college educated, retired, married and Brazilian. It was observed that in our study, gender does not corroborate other similar studies that obtained a larger number of women in their samples. The type of occupation performed by this group in the telephony field can explain this fact, and it is observed that data related to age is corroborated by other analyzed studies, due to the populational aging and higher morbidity of DM type 2 in this age group 1,14,17.
Different from other studies, the participation of people who graduated from college was something noteworthy because it allowed us to know the reality of an educational program directed to the people that uses private health system.
In fact, there is a lack of studies in this field. The role that education plays in the determinants of the health-disease process is evident. In Brazil, the prevalence of DM is higher in the group that completed middle school and lower in the group that is more educated. In this case, it is not possible to verify the impact of this variable, as we did not have a control group. Studies conducted in populations with lower education levels also present similar results. It can be assumed that health education is a practice that collaborates with the control of chronic diseases, regardless of socialclass 3,14.
DM is frequently associated with comorbidities that are important risk factors for high rates of mortality caused by it. Hypertension was the most frequent (65%), as seen in the literature, that is, about 40% of people who are diagnosed with DM are already hypertensive. In our study, the improvement in the diastolic blood pressure of the group was significant, and the final mean of 130 x 76 mmHg confirms the American Diabetes Association (ADA) and Brazilian Diabetes Society (SBD by its initials in Portuguese) recommendations 1,18,19. These findings are not common in different studies, and this should be pointed out by the work of multidisciplinary actions 17,20.
At each meeting, participants showed their glycemic profile, which was discussed with the team. With this, the targets for the glycemic control were reached, the self-monitoring was incorporated and it was observed an adequacy of the clinical prescriptions for 70% of the investigated individuals. Here, it resides a fundamental step for diabetes education described by the action of the global nursing, precursor of the concepts of self-management, self-monitoring, and self-control of the disease. The comprehension of these action sallows to stimulate the adoption of positive behaviors, as well as the recognition of signals and symptoms of the disease, therapeutic update, and better adherence to the clinical treatment 1,11.
Following national and international indicators from ADA and SBD, the glycosylated hemoglobin values for diabetic people are 7%, corresponding to a GM of 154mg/dl 1,19. In the present study, we foundan initial A1C mean of 7.6%, therefore, above the proposed goal (p = 0.0293). Considering the result of an international study, the UKPDS showed a 25% reduction of deaths associated to DM2 for each reduction of one percentage point of the glycosylated hemoglobin 20. The reduction of values for the glycosylated hemoglobin in people participating in educational programs was seen in other studies 21. This could and should constitute an excellent assessment measure of educational programs and still, a neglected indicator in some local levels, in public, as well as in private 1,17,18.
The values of the estimated mean glycemia (EMG) initially measured were of 165 mg/dL, and there was a reduction to 137 mg/dL at the end of the program. These values were compatible with the established world's parameters 1,19. But these results deserve more observations. The guidelines of the SBD highlight through classical studies with an evidence level A, the relationship of the EMG, an important predictor of macrovascular complications, in comparison to HbA1C and the glycemic variability, an isolated risk factor for diabetes complications, regardless of the high values of EMG 1. In the present study, the glycemic variability values obtained represent an evident clinical improvement (p = 0.0313).
Other analyzed clinical exams, such as the fasting glycemia, triglycerides, total and HDL cholesterols, did not show significant differences, probably due to the sample size, associated co-factors, medications used and the time of participant's observation. The LDL fraction presented initial and final average values recommended by the literature that refers to such findings 17,22.
The evaluation of group education programs on DM developed by a multidisciplinary team, with a duration of 6 months or more, indicates that these programs tend to be more effective than individual or routine interventions. The discussions lead to improved knowledge about the disease, clinical aspects, healthy behaviors and lifestyles, and also surpass the biological dimensions, with economic and psychosocial issues 15,17.
Randomized clinical trials and meta-analyses showed that in patients with DM2, structured physical exercise for at least 12 weeks is associated with the average reduction of HbA1C in 0.77% when compared to a control group, and the higher reductions are associated with exercises executed for longer than 150 minutes per week (0.89%), in comparison to short duration exercises (035°%)19,23. Thus, the adherence of PED participants to physical activity collaborated to the results of our study.
Regarding body composition, there was a non-significant decrease in the abdominal circumference mean and maintenance of the BMI mean. However, when analyzing the levels of BMI classification, we observed an interclass transition of participants. The Academy of Nutrition and Dietetics indicates that the benefit of educational interventions in people with type 2 diabetes is controversial, with or without improving HbA1C values in one year of intervention 24. The weight loss of people with DM2 during dietary intervention varies from 1.9 kg to 4.8 kg in one year, although it does not reflect on HbA1C, lipids or blood pressure 25.
The PED acted on two dimensions: the first englobes the necessary knowledge to conduct care related to diabetes control and its complications. The second refers to the action, the active posture of each person that allows change of attitude and the incorporation of new life habits 26,27. A study conducted in Palestine with 405 individuals presented a paradoxical result, in which patients with good knowledge in diabetes had a higher tendency to non-adherence to the treatment, deserving investigation of associated factors 28.
The results showed the increase of knowledge and an implementation of actions for self-care. Some themes that were known became actions practiced at the end of the PED. However, it is noteworthy that these capabilities are not directly related to behavioral changes.
A systematic study of the scientific literature, carried out in Portugal, suggests that dynamic and interactive educational interventions centered on the person, the individualities and the senses of the diagnosis of DM are relevant to the impacts on the participants' health gains. The definition of professionals as reference in the team and the participants of the programs as protagonists of the education process, allows better self-knowledge, care of themselves, and management of health and life conditions 2. Among the successful interventions to promote the health of people with diabetes for self-care and reduction of chronic complications there are innovative methods, such as telephone follow-up by nurses, person-centered interventions mediated by educators in diabetes, which target specific approaches and practices with this population 2.
The problem solving education allows the person to practice the autonomy to transform behavior or not. The professional should know how to recognize and to respect the diabetic person's right to be the protagonist of their care plan, which can include or not the non-adherence to proposed recommendations 29-32, the adoption of pedagogical resources using principles of participatory education, emancipating and co-responsible for stimulating the adoption of self-care 6,10,34. This aspect reinforces the need and the challenge of keeping updates, exchanges of experiences and knowledge among team members in the area of diabetes education 31,32.
A study conducted in India with 307 individuals, mean age 55.6 years and mean time of DM of 10.7 years pointed that 9.4% of the affected individuals had good knowledge about the disease, while 71.3% had a moderate knowledge and 19.2% had insufficient knowledge. Age, education and time of diagnosis were not identified for the presence of DM knowledge 33. Regarding education, one aspect that relates to reflection is the lack of studies with populations that completed higher education levels.
A study conducted at two health facilities in the Philippines with people with diabetes participating in educational groups on the perspective of "Diabetes self-management education", corroborated the effectiveness of education actions by improving glycemic control, measures of waist circumference, knowledge, attitudes, adherence to drug therapy and physical exercise, as well as improving the perception of complications by DM 34. In this study, reductions in HbAic were observed in 60.4% of participants and a significant increase in knowledge (p < 0.001), positive attitude (p = 0.013), perception of glycemic control capacity (p = 0.004) and medication adherence (p = 0.001) 34.
The association between capability scores and the action for self-care to control DM in people who have had the disease for ten years was not different. However, this difference was observed in individuals with five years of diagnosis, a fact that can indicate the need to adopt education actions since diagnosis. Certainly, this aspect needs more evidence.
The most important limitation of this research was the small final number of participants in the study, with almost half of participants dropping out during the educational program. In spite of prejudicing the statistical analysis, and results of efficacy and effectiveness, the study warns that an educational program for this chronic disease should consider the social, economic and geographic vulnerabilities in the proposition of presential activities.
Regarding the scale used, it is known that they do not include all the actions necessary for the control of diabetes and the prevention of acute and chronic complications, which may have hindered the analysis of some aspects related to the subjectivity of diabetes education and which require another research methodology.
Conclusions
The "Program for Diabetes Education" allowed the improvement of glycated hemoglobin values, glycemic variation, and diastolic blood pressure variation of the study participants.
The use of assessment scales for self-care capabilities and actions of people with diabetes pointed to the program effectiveness, allowing us to differentiate capacity of action as an essential factor for the assessment of diabetes education.
Educational actions should be developed according to the target group to achieve the goals desired by those involved in this process. The importance of participative methodologies of health education to guarantee the protagonism and autonomy of the subjects with diabetes regarding the management of their treatment and the strategies faced for the self-care are highlighted.
Based on the present study, self-management education in diabetes is highlighted as an essential strategy for the management of the disease, since the improvement of the clinical variables accompanies the increase in capacity and action for self-care.
This study also confirmed the importance of developing instruments capable of evaluating the impact of education programs on the adherence of people with diabetes to their treatment, and improving their clinical outcomes, as well as guiding professionals in the development of strategies for improvement of diabetes care.


