











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Women infected with the human immunodeficiency virus (HIV) face several personal, family and social challenges, especially during the pregnancy and puerperal period, in which biological, emotional and psychological changes take place. As a way to face the challenges they experience, and in an attempt to maintain their social and family relationships, women hide their diagnosis from people 1. This situation could lead to difficulties in maintaining the care for their own health and for the newborn.
Thus, coping strategies are needed in order to enable the person to constantly adapt to their health situation. Among them, the strengthening of social support through the use of support networks, as well as the availability of care and information, can result in positive repercussions for health and reduce the psychosocial impact caused by the disease. Such coping mechanism helps in the construction of new paths, especially in the face of a chronic condition 2.
In view of the above, continuous treatment is important and, to that end, necessary to minimize obstacles related to social stigma, discrimination and prejudice 1,3, which can be faced with the help of sources of social support, thus reducing the negative effects of stressful events. The support from family and friends is considered a health protection factor, as it encourages self-care and helps women to feel more stimulated to continue their lives with a chronic condition 4.
The concept of social support can be defined as the "information that leads the individual to believe that they are cared for, loved, esteemed and that they belong to a social network with mutual duties" (5, p. 300). Therefore, social support lies within the personal dimension and is composed of members of a social network with common rights and duties 4.
The social support framework presents the predominance of two categories: i) instrumental or operational support and ii) emotional or self-esteem support. The former relates to financial backing and support in solving daily problems. The latter relates to emotional social support, which involves listening and attention or companionship, which contributes to the person's feeling of being loved and cared for 6.
Social support is an essential aspect to motivate women when they are faced with the disease and social issues, and it is considered a predictor for adherence to the anti-retroviral treatment. Although such predictor did not reach sufficient levels of significance in the logistic regression, the bivariate analyses showed that people who perceived greater availability of social support were more satisfied and presented greater adherence to the anti-retroviral treatment compared to those who perceived lesser social support from family members and friends 7.
One study looked at the association between the perception of social support and emotional and physical symptoms related to psychiatric conditions among women. The results showed that women less satisfied with social support were mothers and were about seven times more likely to present a set of symptoms, the most cited being tiredness and sadness, which can characterize suspicion of mental disorder. This research also showed that the main sources of social support were their spouses and children 4. In addition, health professionals were the least mentioned sources of support, although they are the ones that should incorporate in their assistance the type of listening that surpasses clinical aspects, including emotional and family issues, considering that there are situations in which the social support from family members with whom the women live is scarce. The above with the purpose of enabling health approaches with an integral perspective 8-10.
It is important to assess the perceived social support based on the comparison between the gestational and the puerperal periods. In the gestational period, there are recommendations for follow-up in health services in a systematized manner during prenatal care, during pregnancy and the need for adherence to HIV prophylaxis. During this period, women receive increased social support 11. There are also recommendations for follow-up in the puerperal period. However, health services do not provide adequate structure in the scope of social support and attention for women, weakening the care provided to the woman 12, which indicates the fragility of the support network.
In this sense, a review study showed the fragility of the support network indicators in several health situations, although a gap in knowledge production persists for the puerperium period 13. It is evident that the social aspect of labor and delivery is a necessity for women. Despite this, the support from relatives and health professionals is directed towards the child exposed to HIV 12.
In view of the above, this research aims to assess whether the social support perceived by pregnant women is different from that perceived by puerperal women, all living with HIV.
Method
This was a cross-sectional study conducted at the University Hospital of Santa Maria (HUSM), in Santa Maria, Brazil, from April to November 2014. The inclusion criteria were defined as women who used reference services for the care of HIV patients at HUSM during their pregnancy and puerperal periods. The exclusion criteria were incarcerated women or women who preferred private services as their regular source of health care.
The study population was based on a list of pregnant women notified with HIV, provided by the HUSM Epidemiological Surveillance Service, considering pregnancies from 2012 to 2014. This list consisted of 109 possible participants, representing the entire population to be investigated in that study period. Therefore, no sample calculation was performed. All the women in this list were invited when they were in the waiting room for outpatient appointments or in the maternity ward, although 29 women from the list did not attend appointments at the health service during the period of data collection. Another strategy was telephone contact to schedule data collection, in which there were two refusals, totaling 31 losses, resulting in a final study population of 78 participants.
The data collection was developed by a graduate student and four research assistants who were undergraduate students with scientific initiation scholarships and trained to conduct the data collection phase. The instruments were applied in person, in reserved places in the research setting. For data collection, an instrument that contemplated a survey built by the authors with socio-demographic, economic and clinical-obstetric variables was applied.
In order to assess the perception and satisfaction of the social support received, the Social Support Scale for People Living with HIV/AIDS was used. This instrument derived from the Canadian scale called "Social Support Inventory for People who are HIV Positive or Have AIDS," which was adapted, translated into Portuguese, and validated by Seidl and Tróccoli 14. The scale aims to assess perceived availability and satisfaction with instrumental and emotional social support, and was used in this study considering its appropriateness for analyzing social support in contexts of health and disease, regardless of the pathology.
The evaluation consisted of two dimensions and 24 items. The first dimension was related to emotional support (12 items) and the second dimension to instrumental support (12 items). Responses were rated on a five-point Likert scale (1 = never; 2 = rarely; 3 = sometimes; 4 = often; 5 = always) for support availability and support satisfaction (1 for very dissatisfied up to 5 for very satisfied). The variation (1 to 5 points) indicates that the higher the score, the better the perception of the social support received 15. The perceived social support was considered as the dependent variable, while the independent variables were the following demographic, economic and social characteristics: age, education, income, self-declared skin color, marital status, employment, tobacco/drug use, alcohol consumption, and clinical and obstetric characteristics such as previous history of abortion, type of delivery, prematurity, participation in prenatal care, means of HIV transmission, discovery of diagnosis, partner's serological status, use of antiretro-viral therapy (ART), and use of lactation inhibitor.
The hypothesis of this study was based on the theoretical assumption that social support is influenced by independent variables. Based on the assessment of the normality of variables using the Shapiro-Wilk test, descriptive statistics were performed in order to present baseline characteristics and the T test of independent samples. Fisher's exact test was used to assess the distribution of the independent variables versus the dependent variable. Linear logistic regression was used to obtain estimates of Odds Ratios (ORS) and their respective confidence.
The present research was approved by the Research Ethics Committee of the Universidade Federal de Santa Maria under opinion No. 533,126. Besides, the international ethical requirements of the Declaration of Helsinki were met. All participants signed the informed consent form with explanations about the research and guaranteed individual privacy.
Results
The average age of the participants was 43.21 years old (SD = 10-47 years old), median of 10 years of schooling (minimum of 3 years; maximum of 12 years), and median monthly income of BRL 925 (minimum of BRL 134; maximum of BRL 3,000). With respect to the self-declared skin color, 47.4 % (n = 37) identified themselves as white, 25.6 % (n = 20) as black, 20.5 % (n = 16) as brown, 5.1 % (n = 4) as yellow, and 13 % (n = 1) as indigenous. Out of the 78 participants, 64.1 % (n = 50) were in puerperium at the time of data collection (Table 1).
Table 1 Socio-demographic characteristics of the study population
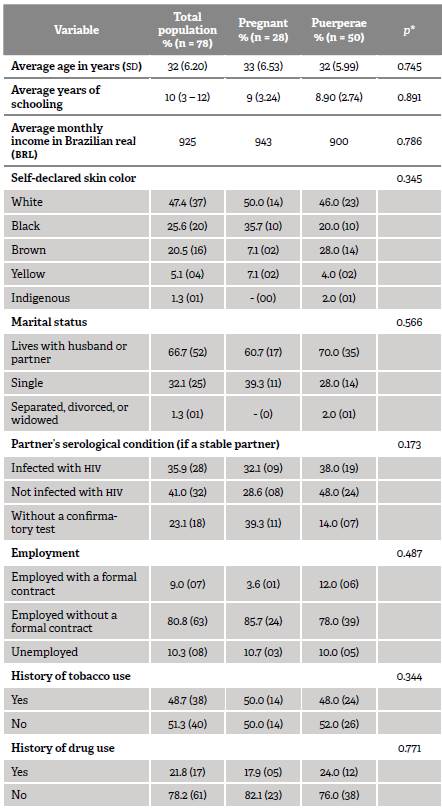
* Fisher's exact test.
Source: authors with research data.
Prematurity (less than 37 weeks of pregnancy) represented 26 % (n = 13) of the variables related to the puerperal period. Regarding the type of delivery, 30 % (n = 15) were vaginal deliveries, 36 % (n = 18) elective cesarean sections, and 34 % (n = 17) emergency cesarean sections. A total of 88 % (n = 44) used ART as the prophylactic measure for vertical transmission (VT) during delivery and 100 % (n = 50) used a lactation inhibitor in the postpartum period. The clinical and obstetric data of pregnant and puerperal women is presented in Table 2.
Table 2 Clinical and obstetric data of the study population
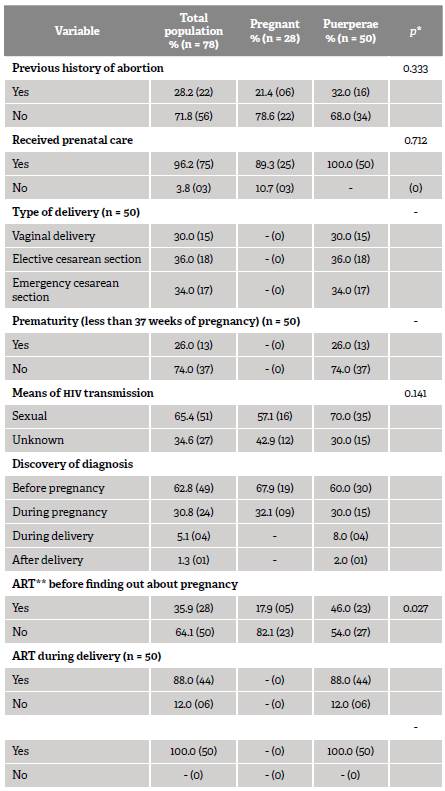
* Fisher's exact test. **Anti-retroviral therapy (ART)
Source: authors with research data.
The population of pregnant and puerperal women presented an arithmetic average of social support of 3.79 points (SD = 0.79). The arithmetic average for the scale dimensions was 3.86 points (SD = 0.86) for emotional social support and 3.73 points (SD = 0.90) for instrumental social support. The assessment of the distribution of social support among pregnant and puerperal women showed a significant difference in total social support and instrumental social support, demonstrating that the group of pregnant women had higher rates of social support compared with the group of puerperal women (Table 3).
Table 3 Distribution of social support among the study participants
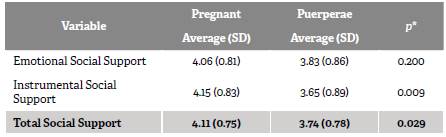
*T-test of independent samples.
Source: authors with research data.
The variables with a significant result among pregnant and puerperal women with HIV show that alcohol consumption and the use of ART before finding out about the pregnancy was higher in puerperal women. This group also reported dissatisfaction with the support received for daily activities, which is perceived in the lack of support from their friends in both emotional and instrumental social supports, especially when compared with the period of pregnancy (Table 4).
Table 4 Independent variables with significant results among pregnant and puerperal women with HIV
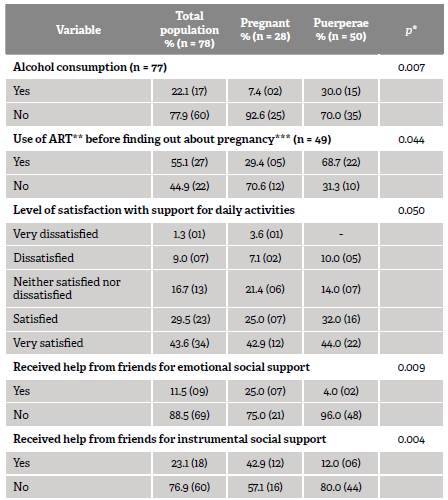
* Fisher's exact test. **Anti-retroviral Therapy (ART)
***Only among those with HIV diagnosis before pregnancy.
Source: authors with research data.
On the other hand, the linear logistic regression evidenced that pregnant women were 8.8 times more likely to receive social support (OR: 8.80, CI: 1.01-16.76) and 6.0 times (OR: 6.00, CI: 1.53-10.48) more likely to receive social instrumental support when compared to puerperal women.
Discussion
The characterization of the participants goes in line with the data presented in the Epidemiological Bulletin of HIV/AIDS from 2000 to 2019, which reported a predominance of notified cases of self-declared brown (48 %), white, (33.4 %), and black pregnant women (13.7 %) in 2018 16. Regarding education, most pregnant women had completed from 5th to 8th grade of school education, representing 28.9 % of the reported cases, a characteristic that can interfere in outpatient follow-up due to the difficulty in understanding and interpreting the guidelines provided by health professionals. Additionally, there is evidence that a lower level of education is associated with an increase in HIV seropositivity rates 16-18.
Most participants were employed, although without a formal contract, with a monthly income between one and two minimum wages. Such conditions make women vulnerable to their socioeconomic situation, which may be precarious, and are related to difficulties in accessing health care services, implying an inappropriate prenatal care that leads to unreliable assistance for VT prophylaxis 19.
Some pregnant and puerperal women had a previous or current history of tobacco and drug use, an issue that should be investigated in prenatal and puerperal appointments as these factors interfere with certain clinical situations, such as premature birth and fetal malformation. These women are more susceptible to situations of vulnerability, especially in the social context, in the gestational experience and in the relationship between mother and child. The use of psychoactive substances is multi-factorial and may be related to socio-cultural and psychosocial aspects, as well as to weak affective relationships 17,20. Thus, it is important to know the network of relationships of pregnant and puerperal women with a view towards interventions focused on reducing the damage caused by injecting drugs, considering that this issue doubles the risk of HIV VT, which makes the risk of miscarriages six times higher 21.
In this study, 28.2 % of participant women had a previous history of abortion. The prevalence of spontaneous miscarriage of 6.1 % and perinatal mortality rate of 4.0 % are associated with other risk factors such as drug use, multiple pregnancies, lack of prenatal care, and absence of anti-retroviral drugs during labor 21.
The sexual means of transmission was prevalent among the participants, as well as the discovery of HIV infection before pregnancy. However, there is a relevant number of diagnoses during prenatal care. The early knowledge of the diagnosis implies the possibility of an early health monitoring, ART and the start of actions that are essential for VT prophylaxis. In other Brazilian states, such as those in the northeastern region, 49.5 % of the diagnoses were in prenatal care and 29.8 % in the pre-pregnancy period 22.
The majority of the participants reported that they had not been on ART prior to the discovery of pregnancy; they used ART only during pregnancy and at the time of delivery. These findings indicate that the discovery of the diagnosis in the pre-pregnancy period does not guarantee the use of ART. Such failures in the follow-up may compromise the goal of eradicating new cases of HIV infection by VT 23. These weaknesses can be overcome through the monitoring of this population in a network care model, promoting a dialog among professionals in order to plan actions that enable the execution of a protocol for VT prophylaxis.
Another issue corroborated with a previous study was the cases of prematurity, which indicates another possibility of an inappropriate prenatal care. A study that searched for factors associated with perinatal mortality evidenced a compromised quality of care for pregnant women and increased risks of VT 21.
The present study compared the perception of social support by stratifying the population into pregnant and puerperal women. Consequently, it was evident that pregnant women report higher scores for total and instrumental social support than puerperal women. Puerperal women are 8.8 times more likely to have low total social support and 6.0 times more likely to have less instrumental support compared to the group of pregnant women. Hence, offering socioeconomic support and solving daily problems are strategies to promote the continuity of treatment, since the precariousness or absence of such types of support interferes with adherence to VT prophylaxis. In this context, it is worthy to note that health professionals are essential in the expansion and maintenance of the primary support network, as they are able to provide subsidies from the information and knowledge shared 24.
A research study conducted with caregivers of children exposed to HIV, mostly their mothers (in puerperium), showed that they expressed the perception of support and absence of support from health professionals. They believed that the service would be able to provide them with instrumental support, such as artificial milk formula and medication, at no charge 25.
In order to analyze which variables could indicate differences in total and instrumental social support between the groups, they were correlated to the socio-demographic characteristics. The analysis showed that alcohol consumption was prevalent among puerperal women. Such behavior is particularly concerning, as it may interfere with the clinical condition of these women due to the organic modifications that take place during puerperium, when the body is returning to its pre-pregnancy state, and it may also adversely affect health with a reduction in the body's defensive cells. Additionally, there are emotional and psychological changes added to the prospect of having an Hiv-positive child and the fear for the social discrimination that the infant may suffer 26.
This study showed that women with restricted social support presented an increase in symptoms of exhaustion, sadness and anxiety, which should be taken into consideration because, sometimes, emotional complaints tend to be neglected in behalf of other health demands 4. It is worth mentioning that HIV exposed children depend on the care, most often from their mothers, for the continuity of VT prophylaxis. This may be affected when the woman is under the effect of an abusive use of alcohol and other drugs or psychological distress, and it indicates the need for support in order to maintain the bond with the child and the care for her own and her child's health.
The pioneering nature of this study can be evidenced by the assessment of social support in pregnant women living with HIV and its difference from that perceived by puerperal women also living with HIV. Therefore, it was not possible to compare this phenomenon with other studies in the literature that used research instruments similar to those presented in this research.
Another important association was the fact that puerperal women had a lower level of satisfaction with the support perceived in their daily activities compared to pregnant women. This indicates the need to bring the sources of instrumental and emotional support together with the purpose of strengthening the relationships between this group of women and their social network, including health professionals, who are sometimes their only source of support 27. These professionals are essential, considering that pregnant women who received appropriate emotional support and prenatal care were more likely (1.52 %) to have an undetectable viral load in the last trimester of pregnancy 28.
Conclusions
Puerperal women living with HIV are dissatisfied with the social support they perceive, especially in the instrumental dimension that involves the clinical practice of health professionals. Thus, health care for puerperal women should be qualified through an active listening that contemplates the social dimension through the mapping of the social support network of women living with HIV.
The knowledge of this network will enable its involvement in the daily care of the baby and the puerperal woman.
In addition, new research studies with different approaches -such as the qualitative- should be conducted. These could consider the understanding of women living with HIV about their needs regarding their social support network. Our study contributes to the planning of actions to deal with this disease, since changes in the clinical practice of professionals may positively affect adherence to prophylactic measures in order to prevent vertical transmission and increase the maintenance of healthy habits.
The limitations of this study consisted of a convenience sample with a heterogeneous distribution of participants between groups. This is justified by the difficulty in accessing the studied population. On this regard, several strategies were carried out during data collection in order to minimize bias. It is important to mention the lack of studies linked to the social support framework with these populations. Similar assessments that could serve as a subsidy for improving the health care provided to these women are required.

