











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The use of zidovudine (AZT) during pregnancy, labor, and childbirth for exposed newborns, in addition to the suspension of breastfeeding associated with the provision of infant formula, are prophylactic interventions for vertical transmission (VT) of the human immunodeficiency virus (HIV) that integrate the protocol recommended by the Brazilian Ministry of Health. When these recommendations are followed, the mother-to-child perinatal transmission reaches rates of 1% to 2% 1,2.
In addition to these measures, a study called PACTG 1043 proved greater efficacy in the treatment of exposed neonates with the introduction of nevirapine (NVP) to the chemoprophylaxis scheme of vertical transmission of HIV during the first 48 hours of life. Its indication occurs due to the mother's viral load or the non-use of antiretroviral therapy (ART) during pregnancy 3. Furthermore, the Brazilian protocol recommends the use of sulfamethoxazole-trimethoprim (SMZ-TMP) for children of 4 to 6 weeks born to mothers living with HIV/AiDS, also indicating the need for differentiated health care. At hospital discharge, the infant should have the first consultation scheduled at a specialized service within the next 15 to 30 days, with regular follow-up until the diagnosis is defined, and also comply with the specific immunization schedule until the diagnosis is confirmed 4.
However, despite governmental efforts and the effectiveness of existing prophylaxis measures, the elimination of HIV VT remains a challenge for health policies in Brazil. The country has not yet achieved the Pan American Health Organization (PAHO) and World Health Organization (WHO) goal of reducing VT of the virus to less than two cases for every 100 infected mothers 3.
At this juncture, for not having self-management capacity, the child depends on their family caregivers, especially regarding treatment adherence, supply of prescribed medications, and clinical follow-up 5. The social and close family support is decisive for the health of the child exposed to HIV, disclosure of the diagnosis, and even for the realization of the care itself, considering that the therapeutic success can be influenced by psychosocial factors 6.
Given this scenario, Nursing has a significant role in the health/disease process of newborns exposed to HIV and the monitoring of care for the control of VT performed by family caregivers. Therefore, professionals must interact with the family caregiver to investigate their ability to provide care, especially during the child's first year of life, with a view to better equip them to adhere to prophylactic recommendations for non-seroconversion and to clarify any doubts. Despite the expressive global pediatric HIV-positive population, studies on care involving this age group and the sociodemographic factors related to the prevention of VT are still scarce 7.
In view of the above, we aimed to establish the degree of pharmacological and clinical compliance of family caregivers of children exposed to HIV and the sociodemographic factors associated with the execution of this care.
Materials and methods
This is a quantitative and cross-sectional research developed in the specialized service for comprehensive care of pregnant women and pediatric patients with HIV/AIDS at a reference hospital located in Pernambuco, Brazil. The study involved the participation of the main family caregivers of children exposed to HIV by VT, aged zero to 12 months, who attended outpatient clinics.
The total population registered and being followed-up in the unit was 67 people. For this study, we adopted a confidence level of 95%, a prevalence of 50% chance of the outcome occurring in the study population, and a sampling error of 10%. By applying the corrected formula for the population found in this study, we obtained a total of 40 participants.
The inclusion criteria for the participants were being the main family caregiver -regardless of gender- of children born at the risk of HIV VT, with up to one year of life, in outpatient follow-up for treatment of HIV/ AIDS, and being present at the chosen service during the period of data collection. Exclusion criteria were being a guardian or professional of a support home or shelter where the child resides, whose parents were unknown, deceased or deprived of family power.
Data were collected by individualized interviews in a private environment. Family caregivers were invited to participate in the study when they attended health services. A structured form was used to capture family caregivers' socioeconomic characteristics, infants' clinical and epidemiological characteristics, and the family support in the face of the HIV-positive situation.
Next, we applied the Scale of Assessment of the Ability to Care for Children Exposed to HIV (EACCC-HIV), developed and validated in Brazil 8. The EACCC-HIV represents a reliable instrument capable of assessing the ability to care for children exposed to HIV, from birth to 12 months of age, through 52 questions divided into five dimensions: i) ability to administer AZT syrup for children up to 42 days of age; ii) ability to prepare and administer formula milk for children up to 1 year; iii) ability to prepare and administer complementary feeding for children over 4 months; iv) ability to administer prophylaxis with SMZ-TMP, for children over 42 days up to 1 year; v) ability to ensure adherence to clinical follow-up and vaccination.
Each dimension can be separately evaluated by measuring the level of skill of the family caregiver in the development of each item. The measurement scale is Likert type, with five intervals of answers that relate to the frequency of childcare activities, ranging from one (never) to five (always). To reach the proposed objective, dimensions i, iv and v were used.
The answers were classified into three levels (low, moderate, and high capacity to care), according to the score obtained. In dimensions I and IV, the level of ability to provide care is considered low with scores 4 to 9, moderate from 10 to 15, and high from 16 to 20. In dimension v, with scores from 5 to 9, the ability to care is considered low, from 10 to 19 is considered moderate, and from 20 to 25 is considered high.
Data were double entered into an Excel spreadsheet and, after validation, exported to the Statistical Package for the Social Sciences (SPSS) software, version 20.0. Data analysis applied descriptive statistics to characterize the sample by means of absolute frequency, relative frequency, and 95% confidence intervals (95% ci) for categorical variables, and by means and standard deviation (SD) for quantitative variables. In the bivariate analysis, the chi-square and Fisher's exact tests were used in order to verify the association between socio-demographic characteristics and the care ability expressed by the scores, adopting a 95% significance level and a p-value <0.05. Dimensions I, IV and V of the scale were considered as the dependent variables, while the independent variables were degree of kinship, age of the family caregiver, marital status, education, employment status, financial benefit, family income, number of residents in the household, family support, and infant's age.
The study followed the standards for investigations involving human beings, and was approved by the Research Ethics Committee of the Center for Health Sciences at Universidade Federal de Pernambuco, Brazil, with the presentation certificate for ethical appreciation number 20270513.4.0000.5208. All participants were previously informed about the objectives of the study and signed the informed consent form.
Results
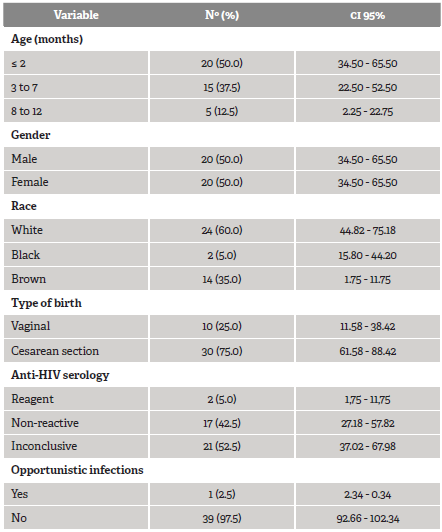
Among the 40 family caregivers of children exposed to HIV through VT, there was a prevalence of mothers (90%), young adults between 19 and 29 years old (55%), with a mean age of 29 years (29 + 8.5), white (45%), living with a partner (65%), between 8 and 11 years of schooling (52.5%), and family income of up to one minimum wage (57.5%), equivalent to USD 188.94. Half of the participants received financial benefit from a Brazilian government social program (50%). Most had family support (90%), either material/ instrumental (52.6%) or emotional (47.4%). Of the profile of children exposed to HIV, half were less than or equal to 2 months old (Table 1), with a mean of 3.5 (+3.13) months.
As for the EACCC-HIV, in the three dimensions analyzed, it could be verified that family caregivers show a high capacity to provide care for children exposed to HIV. When analyzing dimension, I, which concerns the capacity to administer AZT syrup, 35 individuals (87.5%) reported high capacity for this type of care. Regarding dimension IV, 40% were classified with high capacity to administer prophylaxis with SMX-TMP. In dimension v, 20% had moderate difficulty in adhering to the child's clinical and vaccination follow-up (Table 2).
Table 2 Results of dimensions I, IV and V of the assessment scale regarding the ability to care for children exposed to HIV
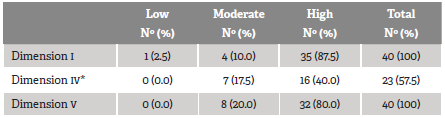
* In this dimension only children older than 42 days were evaluated (n = 23).
Source: own elaboration.
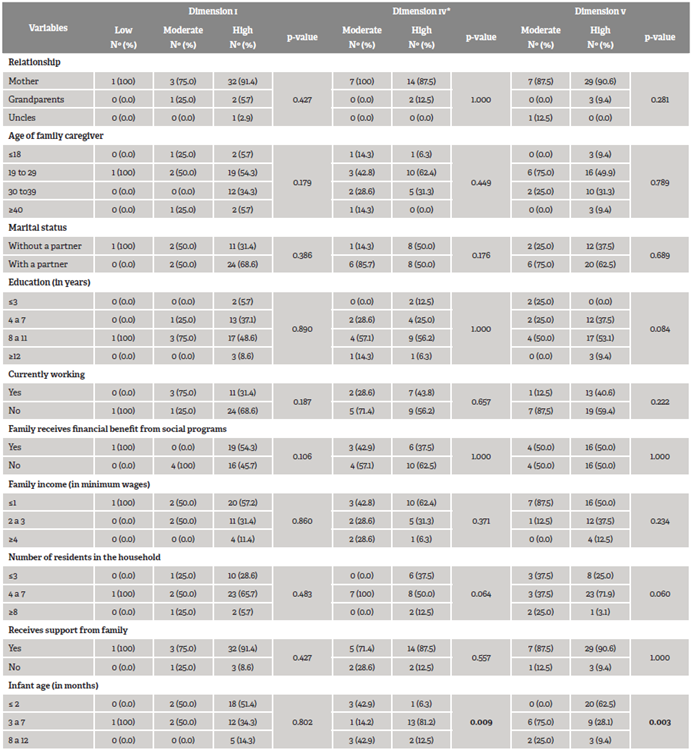
Table 3 shows that there was a statistically significant difference between the ability to administer SMZ-TMP prophylaxis and to ensure clinical/vaccinal follow-up with the age of the child exposed to HIV, with p = 0.009 and p = 0.003, respectively. The three domains investigated reported a higher prevalence of participants with high capacity for childcare among young mothers, aged 19 to 29, who lived with their partner, education attainment equivalent to high school, residing in a household with four to seven people, who did not work, and who received family support.
Discussion
The characterization of family caregivers of children born exposed to HIV in this study showed a predominance of mothers, especially between 19 and 29 years, a finding that corroborates the national dynamics, since the largest portion of women living with HIV in Brazil are young adults, of reproductive age and reduced insertion in the school environment 1. However, this differs from a cohort study conducted with 487 mothers of children exposed to HIV in India, in which infants born to mothers 30 years or older had seven times higher risk of VT infection than those born to mothers under 20 9.
A quarter of the children were found to be born via vaginal childbirth. Recent studies show clinically significant effect of cesarean section as one of the measures to reduce the VT of HIV, however, it is known that this childbirth route is not the most appropriate in all situations 9,10. The Brazilian recommendations are that the procedure should be performed starting in the 38th week of pregnancy, before the beginning of labor, when membranes are still intact, in women with unknown viral load or greater than 1,000 copies/ mL, after 34 weeks of gestation. The vaginal route may be indicated in pregnant women taking ARTS and with sustained HIV-CV suppression or in pregnant women with HIV-CV less than 1000 copies/mL but detectable, if there is no obstetric indication for cesarean section for another reason 2. However, in practice, it seems difficult to guarantee the safe performance of vaginal deliveries 1.
Although the serology of children born exposed to HIV is mostly inconclusive, in this study, the low proportion of opportunistic infections is one of the findings that may reflect the quality in the fulfillment of the guidelines recommended by the Brazilian Ministry of Health, since, due to exposure to the virus, opportunistic diseases such as pneumonia can manifest quickly and with high lethality in exposed children 11. Given this, the benefits of antiretroviral prophylaxis for HIV combined with social factors that contribute to the understanding about the recommendations for the child are unquestionable, considering their non-seroconversion 5.
The high capacity for care found in the three dimensions evaluated, related to the administration of drug chemoprophylaxis, clinical follow-up, and adherence to the vaccination schedule of children exposed to HIV, converge with similar studies that applied the EACCC-HIV in specialized HIV services. These works were developed in northeastern Brazil, with the participation of 62 HIV-positive mothers with children born exposed to the virus 12, and the southern region of the country, with 86 participants 13. Internationally, the limitation of research studies using the scale makes it difficult to compare the findings with similar studies. It is pointed out the need to elaborate research works focused on the translation, cultural adaptation, and validation of the scale in other countries, with the purpose of invigorating health education initiatives in specialized services aimed at this pediatric population exposed to HIV.
However, the factors contributing to pharmacological and clinical compliance of family caregivers of HIV-exposed children are well elucidated in the literature. A cohort study conducted in a small African country in communities with high HIV prevalence found that VT prevention programs that ensure lifetime access to ART for all HIV-positive women, timely testing of exposed children, disclosure of the mother's serology test result, and initiation of drug prophylaxis administration in children are protective factors for child survival. In this study, it is noteworthy that women who disclosed their HIV serology possibly got more support to be adherent to their treatment and that of their infants 14.
A national research developed in South Africa to evaluate the effectiveness of the HIV VT prevention program with 2,811 mother-infant binomials suggested that adolescent and young mothers, the non-disclosure of HIV status to family and friends, unawareness of CD4 test results, late initiation of maternal ART (after childbirth), and giving birth outside the health care facility increased the risk of maternal and infant treatment abandonment, which were also risk factors for non-adherence to therapy by family caregivers. In addition, the mother's knowledge about the national program for VT prevention and the knowledge of the partner's serologic status can improve the adherence to preventive drug care for the child exposed 15.
Children who do not adhere to the treatment protocol and clinical follow-up have a higher prevalence of seroconversion, as identified in a longitudinal study conducted in Equatorial Guinea with children born to HIV-positive mothers. In addition, maintaining breastfeeding is an important risk factor for infection transmission. The prenatal control at early gestational age and maternal ART, initiated in a timely manner, significantly reduced perinatal transmission of HIV, showing that the positivity of children was highly dependent on the adherence of family caregivers 16.
Such aspects are an important target to establish what strategies should be used to strengthen the pharmacological and clinical adherence in exposed children and to identify the critical points in the assistance to family caregivers. Health education actions and dialogue directed to this public are essential for the elimination of HIV VT.
The routine monitoring of the growth and development process of these children becomes fundamental, since those infected could cope with restrictions in weight gain and susceptibility to opportunistic infections during their first months of life 4,17. In the dimension about the capacity of the family caregiver for adherence to clinical and vaccine monitoring, although the assessment indicated high capacity, it is considered that the identification of the group of 20% of the participants who developed moderate capacity in this dimension deserves attention, in the sense that health education actions should be prioritized.
Weight growth impairment is a frequent finding in children with HIV. This initial manifestation can be considered a marker of progression to the disease and a risk factor for infant mortality 14. An analytical ecological study with data from children under 14 years living in Porto Alegre, Rio Grande do Sul (Brazil), showed that access to pediatric care protocols, the clinical follow-up of the exposed child, among other preventive measures, had a direct impact on child survival and mortality by AIDS in childhood 11.
The variable infant's age was significantly associated with the family caregiver's ability to administer the SMZ-TMP prophylaxis and to ensure clinical and vaccination follow-up. A higher prevalence was observed in the family caregiver's ability to offer the chemoprophylaxis with SMZ-TMP to children aged 3 to 7 months. This medication should be instituted between 4 and 6 weeks to 12 months of age for primary prophylaxis of Pneumocystis jiroveci pneumonia 4.
These data reflect that, in children under 2 months, the ability to administer prophylaxis with SMZ-TMP needs to be improved by family caregivers. Perhaps, this is due to the demand for early puerperal care and maternal adaptation, which hinders the administration of prophylaxis, since most mothers are the ones who care for their infants. Among infants aged 3 to 12 months, the capacity for clinical and vaccine surveillance of the child was moderate, suggesting that the advancing months of life of the child and maternal (re)insertion into the labor market may make it difficult to monitor the child exposed to HIV.
Although no statistically significant association was found with the other variables, a higher prevalence of family caregivers with high capacity for medication administration and clinical follow-up for the child was observed among young mothers who lived with their partner, had a better education, lived in a household with relative population density, did not work, and received family support. These are aspects that may interfere favorably in the support to this caregiver and child.
Family support is a determining factor in coping with infection. Eswatini's Ministry of Health initiated a pilot model of family-centered HIV care. Caregivers and health workers interviewed in a survey about the benefits of this model reported that it strengthened family bonding, encouraged family members to disclose their HIV status, and generated mutual support in taking antiretroviral drugs and fewer days in the clinic, shorter waiting times, and that they received better counseling services compared to standard care services 18.
Family support can influence the therapy, thus contributing positively to adherence. Besides, the partner is recognized as one of the main sources of social support in the HIV scenario. In this sense, a cross-sectional study with 179 infected participants, and on ART, found that living with a partner is a protective factor for social support, compared to the reality of single, separated, or widowed individuals, since the chance of protection was almost nine times higher in the first group 19.
The better level of education, measured in years of study, among the participants with high capacity for childcare proved to be an important factor that can interfere directly in the family caregiver's better understanding of the needs of a child exposed to HIV. The low instructional level reflects in limited maternal access to VT instructional preventive measures, as shown in a retrospective documentary study conducted in medical records of 110 mothers with HIV and their children 20.
Other studies corroborate this finding. When analyzing the socioeconomic profile of mothers with HIV in a cohort in South Africa, researchers found a higher prevalence of women with schooling level equivalent only to primary education, an aspect that impacts adherence to ART and may result in HIV transmission from mother to child, resulting in cases of AIDS in children 15.
A study carried out by applying the EACCC-HIV scale with mothers of children exposed to the virus and assisted in reference hospitals showed a statistical association between maternal education and the ability to ensure adherence to clinical follow-up and vaccination of the child exposed to HIV. Among mothers with less than 5 years of schooling, cooperation and clinical-vaccinal compliance ranged from moderate to high, while among those with 6 to 9 years of schooling this capacity remained high 12.
The family support network in homes with relative housing density predominated in the group with high capacity for care, in all three dimensions of the study. This finding validates the results obtained in a cross-sectional study developed in a specialized HIV service using the ability-to-care assessment scale for children exposed to HIV, which showed a relationship between high ability to administer AZT and the presence of three to five people living in the household 13. Divergent results were obtained in cross-sectional studies, in which mothers who had many children and the high number of people in the same household were risk factors for non-adherence to ART and neglect of other care required for children exposed to HIV 21,22.
Reducing HIV VT to 2% or less was set as a global goal in 2017 by PAHO/WHO 23. In addition, it composes the sustainable development goals of ending the AIDS epidemic by 2030 24. Brazil has adhered to these goals, and the eradication of HIV cases in children is one of the priorities of the Department of Chronic Conditions Diseases and Sexually Transmitted Infections of the Ministry of Health (Brazil) for 2019 and 2020 2.
In this context, nursing, together with the health team, is responsible for the best confrontation of the difficulties concerning mother-child HIV infection. Nursing professionals are active in all phases of the measures recommended for the prevention of VT, since preconception, prenatal period, childbirth, and up to the puerperium. Therefore, nurses must be inserted in the secondary support network through the development of innovative educational interventions that provide these women with autonomy over their health 25.
Additionally, the professionals inserted in the specialized health services should identify family caregivers with low capacity to administer antiretroviral chemoprophylaxis and to adhere to the clinical follow-up of the exposed child and act accordingly in order to improve this situation. New studies should be carried out to deepen into the risk factors associated with the adherence to the preventive measures of HIV VT at home, verifying their effects on the newborn's health, as well as to assess the quality of life of family caregivers, since they are the main responsible actors for drug administration and potential non-seroconversion of exposed children.
The limitations of this study include a sample restricted to people seen in a single health service, which hinders the ability to generalize the data, although it is a reference for this type of care and age group. In addition, the results point to associations, but do not allow establishing cause and effect relationships.
Conclusion
Most family caregivers of children born exposed to HIV followed and carried out the current recommendations for HIV VT prophylaxis offered by the health service in Brazil, as established by the high score in relation to the evaluation of the ability to administer antiretroviral chemoprophylaxis and adherence to clinical and vaccination follow-up of exposed children.
Among the sociodemographic factors, infants' age was associated with the execution of these prophylactic cares. The prevalence of better outcomes regarding caregiving capacity was observed among family caregivers with higher education attainment and who received a family support network. Nursing assessments during child health follow-up in specialized services must also consider these non-clinical factors, through the development of an expanded care plan and longitudinal interventions aimed at monitoring family caregivers' ability to provide medication and clinical follow-up for children. The incorporation of these strategies in the praxis of professionals contributes to improve pharmacological and clinical adherence in children exposed to HIV and to enhance the quality of health care, thus providing favorable prognoses.

