











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
In the critical pandemic period we are experiencing, triggered by the Coronavirus Disease 2019 (COVID-19), health professionals have been playing a relevant role. The virus has caused one of the most severe public health problems and the most comprehensive social crisis in the last decades 1. An event of this nature poses challenges to health professionals. Their safety and well-being are significant, not only to guarantee care continuity but, above all, to control contagion due to the role they play in public health education.
Psychological and social changes that affect every-one -especially health professionals- must also be taken into account. Many of these specialists have already lost their lives since the pandemic began 2,3. They are health professionals highly likely to become ill due to the exposure they are subject to, but also due to the unavailability and inappropriate use of Personal Protective Equipment (PPE) and lack of adequate training to face the emergence of extremely infectious disease outbreaks 4-6. Their staffs are under constant pressure, so they begin to develop signs and symptoms related to increased exposure, which is most notorious among nurses 1,5,7. The professionals are vital to the organization and management of health interventions, often as the first and last individuals the patients see 1.
The effects of virus exposure go far beyond debility, morbidity, and mortality 8-10. Since social distancing is the most effective measure of disease control, it can further increase the mental health impact on individuals 9,11. For health professionals, in addition to the increased work hours, lack of personnel and material, it leads to isolation from their families, affecting them physically and emotionally. Therefore, the first signs of change, such as anxiety, depression, denial, insomnia, and anger appear, affecting their clinical decision, judgment, attention, and disease understanding, also having an impact on long-term well-being 8,10,12.
For families, the difficulties of surviving are evident, such as keeping the balance between work, homeschooling with the children, the online work many parents started, the financial concern with income loss, increased chores, among other problems such as gender differences, and domes-tic violence 13.
Despite the possibility of spreading the virus to their relatives, for health professionals, a family is still a form of comfort and a possible return to normality, constituting one supporting element 10. Thus, along with the problems found and described by all families, there is a general concern with infecting the relatives; consequently, some-times, these professionals choose to live away from them for an indefinite period. The previous aspects potentially change the family dynamics and how their members are interconnected 9,10, as reported. Inharmonic families experience more conflicts, disagreements, loss of affection and approval among their members 14. The reality is that all families are experiencing this phenomenon for the first time so far, in a non-normative crisis imposed throughout the world 15.
We highlight the concepts of cohesion, adaptabil ity and family functionality as aspects that can show these changes. The Family Functionality Evaluation uses Family Adaptability, Partnership, Growth, Affection, and Resolve (APGAR) to evaluate each member's satisfaction with the support their family provides 16.
Cohesion is defined as the emotional bond that family members feel for each other, and adapt-ability refers to the family's ability to change its structure, roles in relationships, and rules to respond to situations or development stages 17. Family Adaptability and Cohesion Evaluation Scale II (FACES II) evaluates these concepts separately on scales and then combines the classification to obtain the family type based on these two factors. High values of cohesion and adaptability indicate balanced families, and lower values reveal extreme families 17.
According to Olson (2000) 17, there are particularities to consider about families classified at the extremes: in families named rigid, roles and little flexibility in the rules, imposed by one of its members who controls the family dynamics, are rigid; in chaotic families, members may switch roles, as these are not well-defined; in structured families, there is an adaptation to family roles and rules, which reflects a democratic leadership, with evident participation of children, according to their age 17. More recently, it has become clear that families with extreme behaviors in one of the two dimensions function less satisfactorily (high dependency, member separation, rigidity in the application of discipline rules in response to new situations) than families balanced concerning cohesion and adaptability 19. In either case, the family dynamics of change and transition through the different classifications improve its functioning process 17.
Accordingly, it makes sense to be concerned with these professionals and the support they receive from their families and give to them. Family roles and the dynamics already assumed by the fami ly are aspects that inevitably change 15, which means family support should play an even supe rior role for these professionals. Thus, given the pandemic period and the function of nurses during this process, our study objective is to eval uate nurse family adaptability, cohesion, and functionality during the state of emergency.
Materials and methods
It was an exploratory, quantitative, descriptive, and cross-sectional study. We aimed at accessing the population through snowball sampling, in a non-probabilistic way, and for convenience, with the following inclusion criteria: being a nurse in any situation and professional location, being over 18 years old, and consenting to participate in the study voluntarily.
Instruments for data collection were organized and sent by Google® forms and diffused by email and social networks, such as Facebook®, WhatsApp®, and Instagram®. The questionnaire starts with the informed consent, necessarily validated before proceeding with the remaining part (Decision of the Ethics Committee 2020/12 of Santa Maria Health School). The form required individuals to answer each question before moving on to the next one. Uncompleted questionnaires were excluded.
For the study we used a sociodemographic questionnaire (gender, age, marital status, education), which also includes, in the end, an assessment of the importance some items have for nurses in this pandemic and social isolation period; a questionnaire to characterize the family, housing and fami ly cohabitation during the pandemic, including Duvall's Family Life Cycle Stages, Family Adapt ability and Cohesion Evaluation Scale (FACES II) 17, and questions related to Adaptation, Partnership, Growth, Affection and Resolve (APGAR) 16 that measure the family function.
The Family Adaptability and Cohesion Evaluation Scale (FACES II) evaluates family cohesion and adaptability 17. FACES II is an instrument with 30 items, which uses a Likert-type scale from 1 (seldom) to 5 (almost always), measuring the individual's perceptions of adaptability, family cohesion and the general family function. It has 16 questions measuring cohesion and 14, adapt-ability. Cohesion results in a classification into four levels: disengaged (extremely low cohesion); separated (low/moderate cohesion); connected (moderate/high cohesion), and enmeshed (extremely high cohesion). Adaptability is based on an assessment process, leading to four levels: rigid (extremely low adaptability); structured (low/ moderate adaptability); flexible (moderate/high), and chaotic (extremely high adaptability) 17. The Family Adaptability and Cohesion Evaluation Scale (FACES II) has dimensions and punctuation: cohesion can be classified as disengaged, separated, connected and enmeshed; adaptability can be classified as rigid, structured, flexible and chaotic. With the scale, it is possible to classify each of the families, considering each of the parameters that, combined, result in the categorization of families into four types: extreme, mid-range, balanced and very balanced 17.
The APGAR evaluates family function on a scale from 0 to 10: a score of 7-10 indicates "highly functional family"; a score of 4-6 corresponds to a "moderately dysfunctional family"; and a score of 0-3 refers to "severely dysfunctional family" 16. On one hand, intermediate scores on the cohesion and adaptability scales indicate more balanced family systems. On the other hand, families with extreme scores are less functional 14,17,18.
Data analysis was performed using the IBM SPSS® Statistics V27 software. Since the sample does not have a normal distribution, non-parametric tests were used for inferential analysis (Mann-Whitney U or Kruskal-Wallis), considering statistical significance for p values < 0.05.
Results
In Table 1, there is a summary of the main results. There were 125 responses for the questionnaire, principally in Portuguese north (78.4 %) and central region (10.4 %). The majority is female (80.0 %). The average age is 41.01 (Standard Deviation [SD]) = 12.4), minimum 21 years old and maximum 72 years old. Most nurses are married (52.8 %), 72.8 % have a bachelor's degree, and 8.0 % are already retired. Only a part is currently telework ing (4.8 %). A majority considers living in a “house or apartment, which, without being luxurious, is spacious and comfortable” (57.6 %); the most common household has three members (33.6 %), and 6.4 % have a one-person family. Most classify themselves as a "married couple with children" (54.4 %), and the most predominant life cycle stage corresponds to families with children (20.8 % to “families with school-age children: oldest child: 6 to 13 years old” and 19.2 % to “families with young adults: first child leaving - last child leaving”).
Table 1 Sample characterization, mean values of family APGAR, cohesion and adaptability (N = 125)
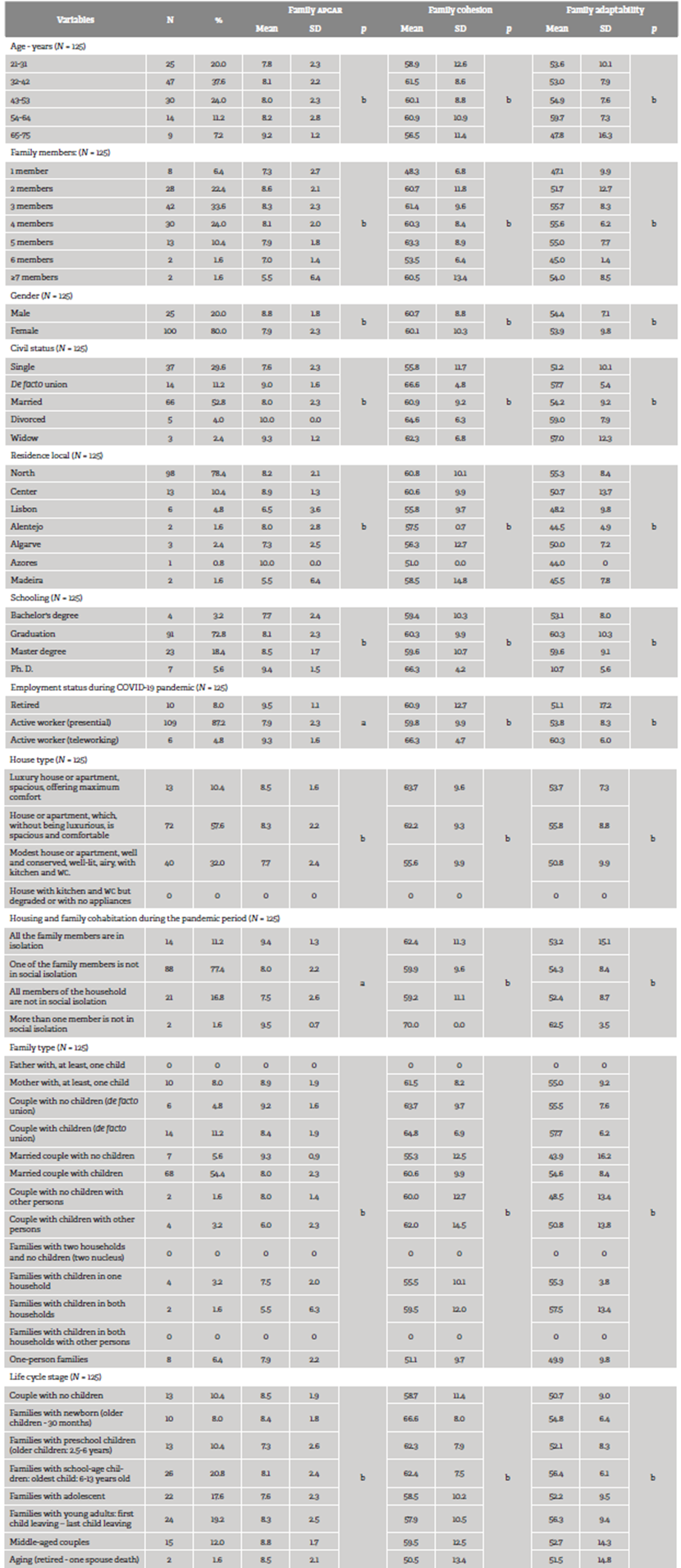
Note. a. p < 0.05; b. p ≥ 0.05.
Source: research database.
The family APGAR presents higher mean scores in the following cases: men (Mean= 8.8; SD= 1.8); older nurses, aged 65-75 years (Mean= 9.2; SD= 1.2); divorced (Mean= 10.0; SD= 0.0); living in the Azores (Mean= 10.0; SD= 0.0); retired (Mean= 9.5; SD= 1.1); and individ uals currently teleworking (Mean= 9.3; SD= 1.6) and with a statistically significant difference in relation to nurses working on-site. Nurses with better housing conditions, families without children, and families with "middle-aged couples" present higher mean APGAR scores (Mean= 8.8; SD= 1.7). There are two to five household members, the APGAR rises, being lower in families with one member or with more than six members. Furthermore, the higher the level of education, the higher the APGAR.
Regarding the household situations during isolation, the APGAR (Mean= 9.5; SD= 0.7), cohesion (Mean= 70.0; SD= 0.0), and adaptability (Mean= 62.5; SD= 3.5) are better in those in which more than one member is not socially isolated. Concerning the APGAR, there is a statistically significant difference.
To family cohesion, the figures presenting the best mean values: men (Mean= 60.7; SD= 8.8); interme diate age groups 32-42 (Mean= 61.5; SD= 8.6), and 54-64 (Mean= 60.9; SD= 10.9); nurses in a de facto union and divorced (Mean= 66.6; SD= 4.8); living in the north (Mean= 60.8; SD= 9.9); those who have more education; those who are teleworking or in a similar situation (Mean= 66.3; SD= 4.7); families living in better conditions; households with more members; families in a de facto union, with children (Mean= 64.8; SD= 6.9); families with newborns (Mean= 66.6; SD= 8.0).
Regarding family adaptability, the following ones present better mean values: men (Mean= 54.4; SD= 7.1); nurses between 54 and 64 years old (Mean= 59.7; SD= 7.3); divorced (Mean= 59.0; SD= 7.9); living in the north (Mean= 55.3; SD= 8.4); with a bachelor's degree (Mean= 60.3; SD= 10.3); currently working (telework or similar) (Mean= 60.3; SD= 6.0); those who live at a house or apartment which is not luxurious (Mean= 55.8; SD= 8.8); families with more than three members (Mean= 55.7; SD= 8.3); families in a de facto union, with children (Mean= 57.7; SD= 6.2). It is also worth mentioning the total mean values concerning cohesion, 60.2 (SD= 10.0), and adaptabil ity, 53.9 (SD= 9.3).
Respecting the family APGAR, and as shown in Table 2, a majority observes their family as "highly func-tional" (80.0 %), and only a percentage esteemed their family as "severely dysfunctional" (4.0 %).
Table 2 APGAR family dimension
| Dimensions | N | % |
|---|---|---|
| Families severely dysfunctional | 5 | 4.0 |
| Families with moderate dysfunction | 20 | 16.0 |
| Highly functional families | 100 | 80.0 |
Note. APGAR: Adaptability, Partnership, Growth, Affection, Resolve.
Source: research database.
Regarding the score obtained on the FACES II scale (Table 3), in the family cohesion dimension, most nurses called their family "connected" (45.6 %). In the family adaptability dimension, a majority (52.8 %) considered their family to be "chaotic". And about type of family, most are categorized as "very balanced" (39.2 %) and "balanced" (35.2 %) families, with the "extreme" type associated to only 4.8 %.
Table 3 Families scores in FACES II factor dimensions
| Factor | Factor dimensions | N | % |
|---|---|---|---|
| Family cohesion | Disengaged | 25 | 20.0 |
| Separated | 25 | 20.0 | |
| Connected | 57 | 45.6 | |
| Enmeshed | 18 | 14.4 | |
| Family adaptability | Rigid | 7 | 5.6 |
| Structured | 15 | 12.0 | |
| Flexible | 37 | 29.6 | |
| Chaotic | 66 | 52.8 | |
| Type of family | Extreme | 6 | 4.8 |
| Mid-Range | 26 | 20.8 | |
| Balanced | 44 | 35.2 | |
| Very balanced | 49 | 39.2 |
Note. FACES II: Family Adaptability and Cohesion Evaluation Scale II.
Source: research database.
With regard to the items, nurses rank crucial during this pandemic and isolation period, the options and results are: "health" (8.6 %); "protection" (8.5 %); "affection" (8.2 %); and less important, "money" (6.8 %).
Discussion
There are no Portuguese studies on nurses' fami lies in this specific situation. High pressure at work has shown to be a factor that can aggravate the conflict between employment and family, affect job and life satisfaction and even cause damage to the professionals' physical and mental health, influencing their performance and ability to make decisions in the workplace, as studies from other countries have confirmed 3,9,10,14,20.
From the analysis of 125 nurse families, a mean value for cohesion and adaptability is slightly higher than that of another study on Chinese nurses working in hospitals (20). However, the comparison must be careful, given the cultural differences.
In the present study, 65.6 % of the families rank in the intermediate levels of cohesion (separated and connected), which are considered more functional. The most extreme levels (disengaged and enmeshed) are likely to cause more damage to their members, and we cannot ignore that 20.0 % are disengaged. Although most families are classified as functional, 20.0 % for non-functional families is worrying.
Nurses who experience more demands in their workplace and who are required to spend their emotional and physical resources tend to have more conflicts in their households 20. A function al family is related to the ability of a family to with-stand stress periods, preserving the system identity and the respect for the individual differences of its members. In addition, we cannot forget Olson's theory 17, which underlines family dynamics as transitory through dimensions, so it is possible a situation in which many of the nurse families experience these dimensions due to the stress triggered by isolation. It does not mean they are necessarily dysfunctional but coping with a different stage and possibly benefiting the household.
Most families have children, and 6.4 % are single-person families. These family types are relevant because they are considered at-risk and under major pressure 1, a situation evidenced in this study through low APGAR scores and cohesion values.
Families living in better housing conditions also present better APGAR, cohesion and adaptability results. Naturally, housing is crucial factor since, with all family members at home together and still working or with school activities, there is a need for more spaces: if they do not exist, sharing is necessary, which puts the members under pressure, establishing more visible differences. In this way, family roles and spaces change and become messy, with a greater need to share domestic tasks and, in turn, increase them. Relevant economic issues can raise, stressing the family much more 13.
Most families consist of three members. This condition scored positive in APGAR, with remarkable cohe sion and adaptability values. Similarly ranked more mature families, without children or with adult children. In other studies, better adaptability values were found in families with two children 20.
Older nurses (65-75 years) score better in APGAR. However, they are not associated with more accurate cohesion and adaptability values. Adaptability is meaningful, and we know the adaptation ability to changes decreases with age 21, thus demonstrating, even more, the relevance of fami ly in determining the mental and physical health status of this age group 22.
Adaptability is also lower in nurses with a higher education level, who may belong, as well, to the oldest and worst adaptable group, given the limitations that can characterize this age group 21. In another study, in China 20, the linear regression also showed worse adaptability in nurses with a postgraduation or a higher education level. Contradictorily, these same nurses present the best APGAR score and family cohesion values. In this case, the relationships may already be well-established and lasting, putting aside the possibilities of other bonds and emotional and affective instability.
Divorced people also have better adaptability. We believe it is related to the life cycle stage, which forced them to overcome a particular adaptative situation (divorce), so now they feel more capable of adapting to new circumstances, relativizing other difficulties.
Nurses who are currently teleworking or in a similar situation prove better APGAR, cohesion and adapt-ability, so those who continue working presential gave lower values, despite all the difficulties fami lies face when they are at home in this situation 13, which clearly places nurses and their families at a higher risk level compared to other individuals.
Despite this reality, it is interesting to note that, in the family APGAR, most families are classified as highly functional. We should also highlight that nurses consider health, protection, and affectivity as the most important aspects at this stage, placing money at the last level, despite the manifest discontent and successive claims heard recently in this regard.
It seems to be a close relationship between better cohesion and good adaptability values, similarly to other studies 14. At the same time, the importance of the family role in the well-being of these profes sionals is confirmed through telephone conversations or image sharing (photos and videos) 23-25.
The institutional role is also mentioned 9, as there is evidence of the relationship between good leadership (by superiors) and the maintenance of nurses' good family cohesion and adaptability (by nurses who are led) 3,20,25. Indeed, the behaviors and adaptation strategies adopted by these professionals vary between individual protection measures and the value of family support. The way the pandemic develops makes us more aware of the family role in health professionals as a way of "thinking" about the family 12,15.
Thus, using a convenience sample, the possibility of data generalization is limited. Most respons es correspond to the north and central region of Portugal since researchers do live there as do the participants, who are mostly their contacts. The questionnaire was aimed at nurses anywhere regardless of their employment status, and we have answers from nurses belonging to different contexts, retired or teleworking, which we decided to validate and include due to the variable difference they present. Moreover, the influence of nurs es' work in care providing and quality of liffe during the lockdown concerning family cohesion and adaptability was evidenced. Likewise, as the questionnaire is self-conducted, it may cause some bias.
Conclusion
In the study, we found that 80.0 % of the families consider themselves functional, but 20.0 % are linked with moderate or severe dysfunction, and it should be handled properly. Likewise, and regarding the FACES II score, most nurses are in intermediate (and more functional) classifications, and we should highlight families in extreme situations (4.8 % classified as extreme and 39.2 % as very balanced), which are the ones with the highest risk of stress signs.
Indeed, age is a predictor of worse adaptability and cohesion values. When all family members are not isolated, emerges a stress factor for a fami ly represented with lower APGAR scores since the increased demand for these professionals entails less support for themselves and their families.
From the study, we were able to identify the following factors, which can improve APGAR, cohesion and adaptability: better housing conditions; families with three or more members; mature families; with children or adult children; with telework.
We propose a future study exploring the factors that affect nurses' family cohesion and adapt-ability given the variable workplace during the pandemic. This aspect influences the family context enormously, allowing the creation of targeted and specific personal and institutional conditions to face with this and other situations. We also propose a more customized approach and a retrospective study as soon as more professionals are available.

