











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Chronic non-communicable diseases (CNCDS) account for 63% of the causes of death worldwide and pose a threat to global public health. Their complexity and increasing costs represent a great burden to the health system, societies and national economies 1. For example, according to a study conducted by researchers from the Brazilian Society of Cardiology 2, more than 17 million of the deaths caused by CNCDS were due to cardiovascular disease (CVD), whose global prevalence is estimated at 22% among people over 18 years, while in the Americas has an estimated prevalence of 14 to 40% in people over 35 3.
In Brazil, there are significant differences as to the prevalence of systemic arterial hypertension (SAH) between men and women, with the former being more affected by this disease (men: 26.7%; women: 19.9%) 4. SAH is an important health problem due to its pathological characteristics and for representing a risk factor for other diseases such as renal failure 3. Recently, SAH has been considered one of the comorbidities most frequently related to the evolution to severe and fatal forms of COVID-19 5.
Within the Brazilian National Policy for Integral Health Care of People Deprived of Liberty in the Prison System 6, monitoring and controlling blood pressure are essential actions for incarcerated population health care. Under the current pandemic moment of COVID-19, such actions should be reinforced, since individuals suffering SAH have contagious rates up to eight times higher than those of other population groups 7.
Added to the above, it is known that the prison population is growing in all continents. For instance, in America, the total number of inmates has increased by 40% since 2000, in a territory affected by insalubrity, overcrowding, permanent confinement, lack of government investment, and increased violence, which favor the development and worsening of SAH 8. In this line, it has been corroborated that imprisonment is associated with increased and uncontrolled blood pressure levels, mainly affecting diastolic pressure 9.
The risk of developing SAH is associated with several modifiable factors (alcoholism, tobacco use, obesity, sedentary lifestyle, eating habits [highlighting fat intake], and stress) and non-modifiable factors (genetics, sex, skin color, and age) 10. Therefore, blood pressure control and its consequences for individuals and society can be modulated by human behavior, beyond its constitutional/biological dimension. This information is relevant to promote health behaviors and prevent and treat this type of health issues in confined spaces. However, despite the magnitude of the morbidity and mortality and the costs related with SAH at incarceration, studies on the factors associated to this condition in inmates are incipient. In view of this situation, this research was aimed at identifying the association between risk factors for SAH and blood pressure levels of prisoners under a closed regime.
Materials and methods
This is a cross-sectional study carried out between February and September 2019 with inmates serving their sentences under a closed regime in a prison complex located in the southern region of Brazil. The complex is a national reference for re-socialization.
The inclusion criteria were being in a closed regime for at least 12 months and having preserved cognitive functions. Inmates in wards, inpatients outside the complex, and highly dangerous inmates were excluded from the sample.
Sample calculation process considered the number of inmates in the year prior to data collection (n = 627), reporting a confidence level of 95% and a 5% sampling error rate. Based on the test analyses, a total of 240 men were required to carry out this study. A pilot study was conducted with 20 inmates, who subsequently took part in the analysis.
The selection of participants was random, and they were approached in the health unit of the prison complex while waiting or finishing their health care sessions. During the approach, inmates were informed about the research procedures and its objectives in the health care rooms of this unit, without the presence of penitentiary professionals. Those who showed interest in participating voluntarily were selected and signed the free and informed consent form.
It is worth noting that data collection occurred in a private room provided by the management of the complex, and that we thoroughly observed the ethical issues involving participants considered as vulnerable in research with human beings. Security measures were guaranteed by the institution and all the established internal protocols were followed at all times, which included participants to be wearing handcuffs and the presence of security agents outside the room.
A semi-structured data collection instrument designed by the researchers was used. This instrument asked for sociodemographic and health-related data (age, education, marital status, skin color, age group, time in prison, tobacco use, alcohol abuse, medication use, fat consumption, coffee consumption, physical exercise practice, and family record of SAH) as well as information about the period of imprisonment. In the item "medication," participants were asked whether they took any medications (prescribed by a medical professional) for the control of blood pressure and blood glucose, without further examining medical records or another type of confirmation.
Some procedures were performed to classify blood pressure (BP), abdominal circumference, heart rate, risk factors and body mass index (BMI), calculated by means of height and weight and categorized according to the World Health Organization (WHO) 11. The instruments for data collection included a stethoscope, a sphygmomanometer (with appropriate cuff for measurement of arm circumference in adults), measuring tape (to measure abdominal circumference and height), a calculator, a Segma® digital scale in tempered glass, and an oximeter.
To measure BP, participants were required to remain seated for at least 15 minutes, empty their bladder, refrain from drinking coffee, eating food or smoking up to 30 minutes before the measurement, and to refrain from exercising 60 to 90 minutes before the measurement session. Participants were weighed barefoot and positioned in the center of the scale. To verify height, they stood barefoot with the body in contact with a wall where a tape measure was fixed.
The measurement of abdominal circumference was verified according to WHO guidelines, from the height of the last rib and the apex of the iliac crest, a body area in which there is usually a concentration of visceral fat. Values up to 94 cm for men were considered as a healthy measurement of the abdominal circumference 12.
The data collection instrument and the research protocol were based on the VII Brazilian Guideline on Hypertension, which was in force at the time of conducting the research (2019) 13. Such document served as reference for the classification of blood pressure. Therefore, it became unfeasible to perform a data analysis based on the new guideline published in 2020.
This study did not intend to diagnose SAH in prisoners, since diagnosis is a medical competence based on at least two BP measurements held in the health service and measurements elsewhere, through ambulatory blood pressure monitoring (ABPM) 13. The study identified, in a single measurement, participants BP level. In cases of BP ≥ 140 mmHg in systole or ≥ 90 mmHg in diastole, a statistical correlation was established between elected cardiovascular risk factors.
Participants with normal BP were instructed to have their BP measured annually, while prehypertensive participants (those with 121-139 mmHg in systole and 81-89 mmHg in diastole) were told to do so every six months. In both cases, participants were advised to observe health behaviors and risk factors for SAH in their daily lives.
The data collected were tabulated in a database validated by double typing in order to identify filling errors. Data were then analyzed using the software Statistical Package for the Social Sciences (SPSS), version 20.0. Descriptive statistics were used for numerical variables, with measures of central tendency and proportions for categorical variables. In addition, various statistical tests were adopted for sample analysis: Mann-Whitney's test (non-parametric) to verify differences; Pearson's chi-squared test to study associations between independent variables; Odds Ratio (OR) for association between variables; Tolerance and Variance Inflation Factor (VIF) to test multi-collinearity.
After the first analysis round, the variables identified as significant (p < 0.20) were submitted to the unconditional forward stepwise (likelihood ratio) method for multivariate analysis. A significance level of p < 0.05 and Nagelkerke's R2 values were established for all inferential statistical tests. The Hosmer-Lemeshow test was used to evaluate the quality of fit. Finally, the Kolmogorov-Smirnov test was used to verify the normality of data.
The study was approved by the Ethics Committee for Research with Human Beings at Universidade Federal da Fronteira Sul, under the number CAAE 07049518.2.1001.5564. The ethical precepts of Resolution 466/12 by the National Health Council were also respected.
Results
A total of 240 inmates participated in the study. Participants had a mean of 37.17 years (SD 11.5 years), most of them had attended school for five to eight years (39.2%), were single (48.8%), had been in prison for less than four years (67.9%), and were brown (42.9%) and white (41.3%). Most participants were normotensive at the time of data collection (66.3%) (Table 1).
Table 1 Sociodemographic and clinical characteristics and inmates' length of confinement. Chapeco, Santa Catarina, Brazil, 2020
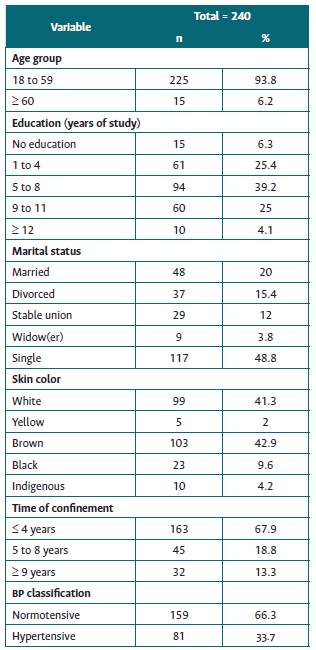
Source: authors.
In the initial analysis, the cardiovascular risk factors associated with BP were smoking, medication use, physical exercise, and family history of SAH (p < 0.20). Physical exercise was negatively associated with the development of SAH (p = 0.034) (Table 2), while previous or current tobacco use was not statistically correlated with SAH (p = 0.081). Similarly, problematic alcohol consumption was not a significant factor for hypertension (p = 0.555). Finally, the regular use of medication for controlling SAH and diabetes mellitus (DM) was not associated with hypertension (p = 0.09) (Table 2). This item was asked to the participants and not verified through clinical records.
Table 2 Univariate analysis of cardiovascular risk factors among inmates. Chapecó, Santa Catarina, Brazil, 2020
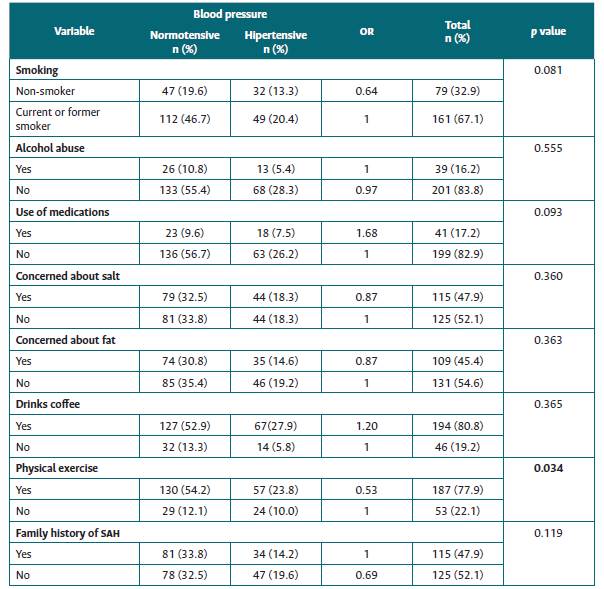
Source: authors.
Regarding careful food intake and possible lack of control of BP, the concern with salt and fat consumption showed no association with hypertension (p = 0.360 for concern with salt consumption and p = 0.363 with fat consumption). No correlation was identified between coffee drinking and SAH (p = 0.365) (Table 2).
Table 3 shows the analysis for cardiovascular risk associated with the following variables: age group, marital status and length of confinement; anthropometric characteristics (BMI and waist circumference); heart rate; and the presence of four or more modifiable and non-modifiable risk factors among participating inmates, all associated with BP. In this regard, BMI and waist circumference were positively associated with cardiovascular risk and SAH (p = 0.000). In this analysis, BMI, waist circumference and HR were associated (p < 0.20). The variables age, marital status, and length of confinement showed no statistical correlation with cardiovascular risk in this population. Besides, the number of participants with and without (known) family history of SAH was homogeneous (47.9 and 52.1 %, respectively), and this non-modifiable variable was not correlated with cardiovascular risk (p = 0.119) (Table 3).
Table 3 Univariate analysis of cardiovascular risk factors among inmates. Chapecó, Santa Catarina, Brazil, 2020
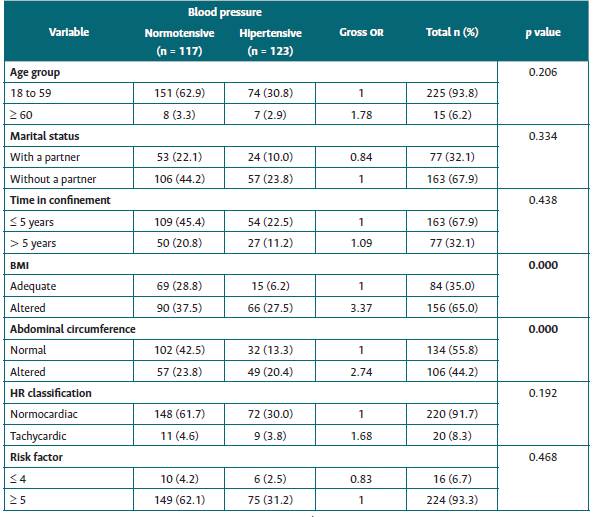
Source: authors.
The results of the multivariate analysis are presented in Table 4. Statistical significance was revealed for BMI when controlled for all other variables in the model, i.e., the chance of developing SAH was 2.33 times higher for inmates with altered BMI. There was no statistical significance for the other study variables.
Table 4 Final logistic regression of modifiable and non-modifiable factors associated with the occurrence of the outcome (cardiovascular risk) among inmates.
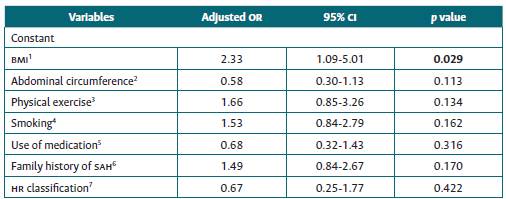
Note: 1: adjusted by the constant; 2: adjusted by BMI; 3: adjusted by BMI and waist circumference; 4: adjusted by BMI, waist circumference and exercise; 5: adjusted by BMI, waist circumference, exercise and smoking; 6: adjusted by BMI, waist circumference, exercise, smoking, and medication use; 7: adjusted by all the previous variables.
Source: authors.
Discussion
Participants' BP level is comparable to that of the general population, a similar finding to that of a research study carried out in a penitentiary in Rio de Janeiro (35%) 14. This means that confinement in a prison environment is not a factor that influences BP levels. Risk factors for cardiovascular diseases conventionally associated with SAH were correlated, with a prevalence of modifiable risk factors. This result implies that institutional health programs may affect BP among this population.
The inmates that participated in this study were mostly normotensive at the time of data collection, similar findings to a study carried out in the state of Ceará in Brazil 15. Although incarceration is not a predictive factor for BP changes, research studies in the United States have found that men in detention have reported changes in BP more frequently than men at large 8. From a macroscopic perspective, incarceration is known to increase an individual's socioeconomic disadvantage, which predisposes him or her to cardiovascular risk 16.
Sedentary lifestyle favors the onset of cardiovascular disease in inmates. In a Canadian study, it was shown that regular physical exercise in this group is important, creating changes in their BMI and abdominal circumference. In that research, 57.8% of participants performed high and low intensity physical activity at least 30 minutes per day, which corresponds to 210 minutes per week, meeting WHO recommendations 17. These data indicate that regular physical exercise reduces risk factors related to SAH. In the Canadian reality, physical exercise is an institutional action, which differs from the present study, where this practice occurs by individual motivation. In the US scenario, in a 12-month research with 103 inmates, weight gain increased as physical activity decreased, making individuals a risk group for SAH 18.
Although BMI does not differentiate body compositions and is therefore questioned by some authors 19) as a predictor of weight status, it is still the most widely used classification to stratify weight, given its effectiveness in clinical use to predict cardiovascular risk. This study evidenced that the BMI of prisoners is a risk factor associated with SAH. In this regard, it is worth noting that US researchers investigated juvenile detainees for 12 months and found that their BMI increased by 3.4 kg/m2 after incarceration. The percentage of youths with healthy weight decreased from 69 to 42%, and the percentage of overweight youths increased from 33 to 52.5% 20.
With regard to the variable waist circumference, this has been identified as an important risk factor for SAH. In a research conducted with 754 prisoners in a Canadian penitentiary, it was shown that waist circumference can be reduced through regular physical activity, a proper diet and regular sleep patterns 17. Weight gain/change in BMI, frequent among prisoners, is related to cardiovascular aggravations and predicts health problems such as DM, obesity and cardiovascular diseases 21.
A recent Brazilian review article indicates hypertension and overweight/obesity as cardiovascular risk factors for the incarcerated population. That is why there is a concern, especially in the US, in unveiling cardiovascular risks in this vulnerable public; not to mention the costs and therapeutic challenges of this complex network of problems for public health. In the study, abdominal circumference above the indicated parameter was correlated to hypertension and deficit in physical activity practice 22.
The modifiable risk factors, especially BMI, waist circumference and regular exercise, showed an association with the onset of hypertension. As these are modifiable risk factors, it is assumed that there are failures in health care in these spaces of deprivation of liberty 23. Given this, it is necessary to address the problem by the perception that, in the confined space, these men depend on institutional interventions for the control, prevention, and treatment of SAH and, ultimately, of cardiovascular aggravations.
In the prison environment, individuals are deprived of their autonomy to manage health behaviors due to a routine that imposes sedentarism, and consequently bad lifestyle habits. Since cardiovascular diseases are an important cause of death among prisoners and early detection and treatment are ensured to them by the State, the management of cardiovascular risk factors should be promoted 16,24. Studies of different designs are fundamental to mobilize prison and governmental institutions, as well as to subsidize institutional and intersectoral actions in this direction 25.
This research was conducted by nurses and nursing students and sheds some light on the responsibility of this professional category and interdisciplinary teams for the prevention, early identification and management of cardiovascular risk and hypertension in inmates. It highlights the need for the development of institutional programs linked to the Brazilian Unified Health System in order to promote self-care, since the risk factors identified here are modifiable by information (health education) and health behavior.
Starting from the premise that men are culturally resistant to self-care, it is understood that they need to be mobilized into transforming their attitude towards health 22. It is emphasized the responsibility of health professionals in the process of intelligent modification of prison routines and prisoners' decisions about their lifestyle, considering, of course, the real restrictions imposed by these institutions.
The limitations of this study include its cross-sectional design (a single BP measurement) and the fact that participants' medical records were not accessed, which limited a comprehensive assessment of their BP patterns, SAH diagnosis, and possible treatments.
Conclusions
This study found that risk factors for the development of SAH are present in the prison environment to a similar degree as in the general population. Among the risk factors significantly associated with increased blood pressure levels was the reduced practice of physical exercise, as well as altered BMI and waist circumference. It is worth noting that BMI was the variable of greatest statistical significance, since, when altered, it increased 2.33 times the chance of prisoners developing SAH.
Still, it should be noted that inmates do not have complete autonomy to define their eating patterns and the practice of physical exercise. Therefore, knowing the cardiovascular risk factors among this population brings particular challenges for governments, penitentiary system leaders, and the professionals who serve them, all this amidst an intersectoral and interdisciplinary context.

