English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Risky health behaviors such as smoking, drinking and obesity, are considered a major source of morbidity and mortality associated with cardiovascular diseases, cancer, diabetes, and liver diseases. Additionally, having unsafe sexual behavior could be a source of sexually transmitted diseases (STD), which in turn, could be the cause of severe illnesses, infertility, long-term disability, and even death for millions of people. The World Health Organization (WHO, 2014a) estimated that in 2012 about 6% of deaths worldwide were attributable to alcohol consumption, 11% to tobacco use, and 5.7% to insufficient physical activity. Furthermore, according to the WHO (2012) in 2008 there were about 500 million new cases of four STDs in adults between the ages of 15 and 49.
Colombia is not the exception on this matter. The Pan American Health Organization (2012) emphasizes that for individuals between 18 and 69 years old, 7.6% of the population was considered at risk of alcohol dependency, while the prevalence of current smokers was 12.8%. Also, the prevalence rate of HIV for adults aged 15 to 49 was 0.5% in 2013 (UNAIDS, 2014).
Education has played an important role in preventing risky health behaviors. In general, the theoretical literature has found that there are three main channels through which education affects health, and consequently risky health behaviors. The first two channels date back to Grossman (1972) who studied the demand for health, considering health as a form of human capital. In the productive efficiency channel, education directly affects the health production function, considering that more educated people obtain more health output given a certain amount of inputs. In the allocative efficiency channel, education affects the input mix in the health production function, since more educated people choose a different input mix than less educated people in order to produce more output. The third channel, put forward by Fuchs (1980), establishes that education and health are likely to be affected by the same set of unobserved variables.
Specifically, in the case of risky health behaviors, there has been a growing interest in studying empirically the role of education, dating back to Ross and Wu (1995) who evaluate the relationship between education and health in the United States, taking into account health lifestyles. The majority of these studies have been carried out for developed countries; they have found that there is a negative relationship between schooling and the prevalence of smoking, heavy drinking and obesity. For example, Cutler and Lleras-Muney (2010) evaluate the relationship between education and risky health behaviors by means of the education gradient for the United States and the United Kingdom. Buckles, Hagemann, Malamud, Morril and Wozniak (2016) study the effect of education on smoking, heavy drinking and obesity, and Cawley and Ruhm (2011) analyze the relations between education and smoking, alcohol consumption, physical activity, diet, and the use of illicit drugs, also for the United States.
The association between education and health behaviors has also been studied for several European countries. For example, Brunello, Fort, Schneeweis and Winter-Ebmer (2015) study the effect of education on smoking, drinking, exercising and the body mass index, considering short and long-run mediating effects for 13 European countries. Renner (2011) examines the possible channels through which education affects smoking tobacco, alcohol abuse, and overeating for eleven countries of the European Union. In general, these authors find that education reduces the probability of having some risky behaviors. For specific countries, Etilé and Jones (2011) analyze the relationship between schooling and smoking in France; Jürges, Reinhold and Salm (2011) investigate the effect of schooling on smoking and obesity in West Germany. For Australia, Webbink, Martin and Visscher (2010) analyze the effect of education on the probability of being overweight.
For developing countries, studies have mainly focused on the effects of education on sexual behavior. For example, the effect of schooling on the use and knowledge of contraception for women has been studied by Andalón, Williams and Grossman (2014) for Mexico, by Dinçer, Kaushal and Grossman (2014) for Turkey, and by Mocan and Cannonier (2012) for Sierra Leone. In addition, Agüero and Bha-radwaj (2014) find that education has a positive effect on having more knowledge about HIV and a negative effect on the number of sexual partners for women in Zimbabwe. Also, de Walque (2006) finds that education is an important predictor of sexual behaviors in Burkina Faso, Cameroon, Ghana, Kenya, and Tanzania. In the case of Colombia, Varela et al. (2011) estimate the prevalence of risky sexual behaviors and analyze their relationship with socio-demographic characteristics in adult population from all regions of the country; Campo-Arias, Ceballo and Herazo (2010) study the prevalence and factors related with risky behaviors for reproductive and sexual health for high school students in the city of Santa Marta, and Brook, Brook, Pahl and Montoya (2002) identify the relationships between drug use, risky sexual behaviors and early pregnancy in Colombian teenagers.
The aim of this paper is to study the relationship between education and risky health behaviors in Colombia. The study of this relationship is important given that the burden of premature deaths and diseases caused by these behaviors is heavily concentrated in low and middle-income countries, causing not only distress for those involved, but also high economic costs for health services.
This paper constitutes, to the best of our knowledge, one of the few applications using data from an emerging economy that considers not only risky sexual behavior, but also other risky behaviors such as alcohol abuse, smoking tobacco and obesity, which have mainly been studied in developed countries. This study also contributes to the literature by providing evidence on the relationship between education and other covariates and health behaviors by area of residence (i.e., rural vs. urban). This analysis is important due to the significant differences observed in years of schooling between urban and rural areas, which has not received a great deal of attention in the literature. Furthermore, we take into account differences in gender, since traditional gender roles may influence the effects of education on risky health behaviors.
In general, our results are consistent with the empirical literature. In particular, we found that there is a negative and significant effect of education on the probability of smoking and a positive effect on the probability of heavy drinking and having unsafe sexual behavior, underlining the importance of social and cultural factors. In addition, knowledge variables about the negative effect of these behaviors on health reduce the probability of smoking, heavy drinking and obesity.
This paper is divided into four sections, besides this introduction. The second presents the empirical strategy used in the estimations. Section three provides information about the data used in the analysis. Section four presents and discusses the results. The last section concludes.
EMPIRICAL STRATEGY
In order to analyze the effect of education on an individual's risky health behaviors, we follow the empirical strategy proposed by Cutler and Lleras-Muney (2010). Specifically, we first estimate the basic equation, including education and a set of basic controls, that is:

where H i is the risky health behavior of individual i (i.e., current smoker, heavy drinking, obesity, and unsafe sexual behavior); E i is the education of individual i, measured as the years of schooling; X i is a set of basic controls, such as age, gender and ethnic group; and εi is the error term which is assumed to be normally distributed.
From this estimation we obtain the education gradient, given by the education coefficient (α 1 ), which measures the effect of schooling on the risky health behavior.
The second step consists of re-estimating equation (1) by adding a set of income and socio-economic variables in order to identify if the effect of education is mediated by these type of variables. That is,

where Y i . is a set of socio-economic explanatory variables (e.g., income, marital status, geographical location of the individual, social security regime, labor participation, and overcrowding). From this estimation we can obtain the education gradient (α 1 ) once this set of explanatory variables is added to the basic equation. This procedure allows us to calculate the percentage of change in the education coefficient from the addition of these variables.
Next, we re-estimate equation (1) adding a set of knowledge variables. These variables could play a mediating role in explaining the relationship between education and risky health behaviors. It is important to consider that people with different education backgrounds can obtain information about health behaviors from several sources and can understand it in different ways. That is,

where Zi is a set of knowledge variables about health risks (e.g., if an individual knows that smoking increases the chance of developing cancer, that smoking is harmful for unborn children and pregnant women, that alcohol is harmful for health, if individuals know that exercise is good for health, if individuals have heard about condoms).
Finally, in the same equation we estimate the effect of years of schooling and all the covariates considered above on each risky health behavior, according to the following equation:

Since the risky health behavior variables of individual i (H i .) are binary, the estimations are carried out using logit models.
DATA SOURCE AND VARIABLES
The data used in this paper come from the Colombian National Health Survey (NHS) carried out by the Ministerio de la Protección Social de Colombia (2007). The survey has national coverage and provides information on the assessment of general health and the main problems faced by the population from all regions in the country. The survey gathers socio-economic information for all individuals in the household, including education, employment, perceived morbidity, demand and utilization of health services, chronic conditions and risk factors, and physical activity. Also, it includes questions on assault and assault injuries, sexually transmitted diseases, perception and knowledge about HIV/AIDS, and psychoactive substances.
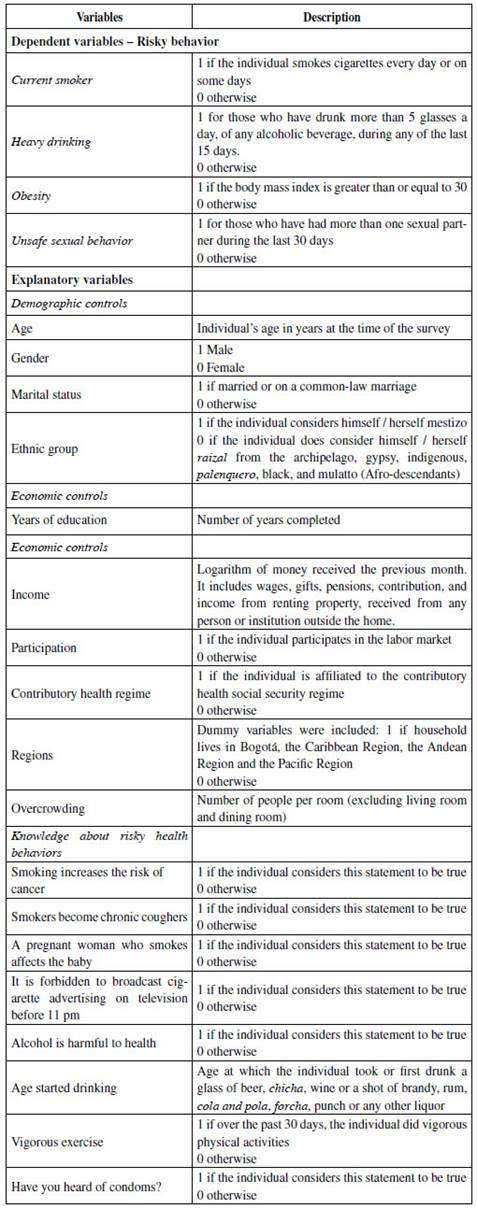
Our empirical analysis is carried out for individuals who are 18 years and older. The resulting sample will depend on the number of individuals who answered the relevant questions about risky health behaviors. Specifically, we consider four risky health behaviors, namely: current smoker, heavy drinking, being obese and unsafe sexual behavior. These variables were defined as dummy variables, based on the information provided by the NHS, where a current smoker takes the value of 1 if the individual smokes cigarettes every day or some days of the week, and 0 otherwise; heavy drinking takes the value of 1 for those who have drunk more than 5 glasses of any alcoholic beverage a day during any of the last 15 days, and 0 otherwise; being obese takes the value of 1 if the individual's body-mass index is greater than or equal to 30, and 0 otherwise; and unsafe sexual behavior takes the value of 1 for those who have had more than one sexual partner during the last 30 days, and 0 otherwise.1
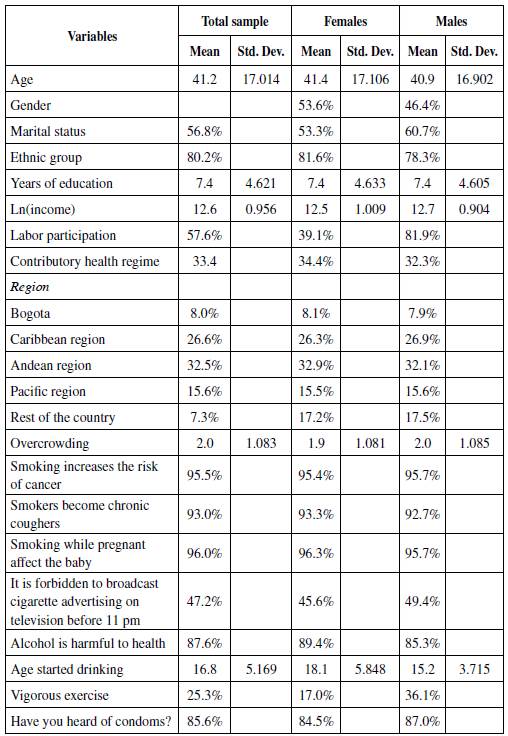
To characterize an individual's risky health behaviors, our analysis evaluates the role played by socio-economic variables and some indicators about the knowledge on these risky behaviors, as mentioned in the previous section. These variables were divided into three groups, besides education. First, we have a group of control variables (Xi), including age, gender and ethnic group; second, the socio-economic variables (Yi) include household total income (in logs), overcrowding, and a set of dummy variables indicating marital status, the geographical location of the individual, labor participation, and whether the individual belongs to the contributory or subsidized social security regime. Third, a set of knowledge variables about health risks was considered (Z i ). In the case of smoking, dummy variables were added, indicating whether individuals consider the following statements to be true: smoking increases the risk of cancer, smokers become chronic coughers, smoking while pregnant affects the unborn child, and it is forbidden to broadcast cigarette advertising on television before 11 pm.
For heavy drinking, a dummy variable was included, indicating if the individual considers that drinking alcohol is detrimental for his/her health; also the age at which the individual started drinking or first drank was considered, since early initiation of alcohol consumption could be associated with increased risk for alcohol dependence at later ages (WHO, 2014b). In the case of being obese a dummy variable for the individual performing vigorous exercise was included, which not only is an indicator of knowledge about the importance of physical activity, but also suggests actual practice. Lastly, for unsafe sexual behavior, a dummy variable about his/her knowledge on condoms was considered.2 Tables A1 and A2 in Appendix A present the definition and the descriptive statistics of the variables included in the analysis.
RESULTS
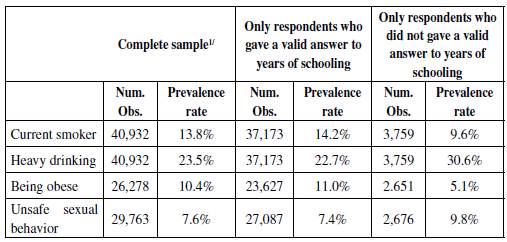
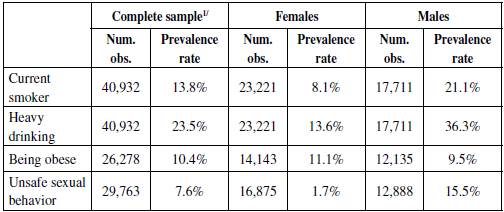
First, we present the prevalence rates and the predicted probabilities of the effect of years of schooling on each risky health behavior, after controlling for age and gender. Table 1 shows prevalence rates by gender of risky health behaviors of the population under consideration. In all cases except obesity, male prevalence rates are higher than those for females.3 For example, in the case of males, the prevalence of current smoking is 21.1%, while for females this rate is 8.1%. For heavy drinking, the difference between males and females reaches more than 22 percentage points, whereas the prevalence of having more than one sexual partner during the last 30 days is almost 14 percentage points higher for males.4
Table 1 Risky Health Behaviors Prevalence Rates (Percentage)
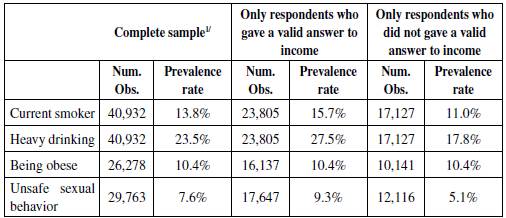
1/ The resulting samples for being obese and unsafe sexual behavior are smaller than for the other two behaviors. In the first case, some individuals did not know either their height or weight which is required to calculate the BMI; in the case of unsafe sexual behavior, the relevant questions came from a different survey module.
Source: Authors' calculations based on NHS (Ministerio de la Protección Social de Colombia, 2007).
The relationship between education and risky health behaviors is illustrated in Figure 1 by means of the predicted probabilities of the effect of years of schooling on current smoker, heavy drinking, being obese, and unsafe sexual behavior, controlling for age and gender. The effect of years of education on these behaviors is mixed. In general, there is a negative relationship between years of education and smoking; a positive relation with heavy drinking, and no particular pattern in the cases of being obese and unsafe sexual behavior. In particular, each additional year of education reduces the probability of being a current smoker from 23% for individuals without education, to 12% for those individuals with 18 or more years of schooling. Conversely, the probability of drinking heavily increases with each additional year of schooling, up to 10 years, where this probability is 35%; beyond this level of education, the probability remains around this percentage. In the case of being obese, this probability remains around 12% independently of each additional year of education. Similarly, the probability of having more than one sexual partner during the last month does not present significant changes with each additional year of education, remaining at about 15%.
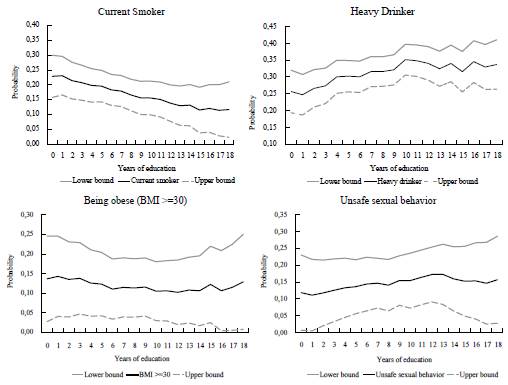
Note: Predicted probability from Logit regressions on education, controlling for age and gender. 95% confidence intervals. Source: Authors' calculations.
Figure 1 Effect of Education On Risky Health Behaviors: Predicted Probabilities
Next, for each risky health behavior, we present the education gradient and the percentage change in the schooling coefficient from the addition of each set of explanatory variables (namely, socio-economic (equation 2) and knowledge variables (equation 3)). In a second exercise, we characterize each risky health behavior based on the estimation of equation (4). The analysis is carried out for the complete sample and also by gender and area of residence, where the latter splits the sample depending on whether the individual lives in an urban or rural area.
Education Gradient
Table 2 presents the effect of socio-economic and knowledge variables on the education gradient for the four risky health behaviors under consideration.5 First, we estimate the basic equation (1) for the complete sample. The results indicate that the probability of smoking reduces with each additional year of education. On the contrary, the probability of heavy drinking increases with education, since alcohol appears to be a normal good (Cutler & Lleras-Muney, 2012). Similarly, the probability of having unsafe sexual behavior increases with education. Meanwhile, education does not affect the probability of being obese; hence, in this case, it is not possible to calculate the education gradient.
The results suggest that education has helped reduce the incidence of smoking in Colombia, but not that of alcohol consumption, which can be linked to cultural and social factors and/or to the failure to recognize the damage that alcohol abuse causes to an individual's health, as has been done in the case of cigarette smoking. Nowadays, cigarette smoking generates social rejection, since it is forbidden to smoke in public places, while it has not been the same with alcohol consumption, which historically has been a social activity and whose "... consumption and behavior have been subject to self-imposed social controls" (The Social Issues Research Centre, 1998, p. 6). Moreover, despite that, individuals recognize that alcohol consumption is harmful, they tend to disregard the impact of alcohol consumption in everyday life; namely, the development of chronic diseases, mental disorders, alcohol dependence, as well as the injuries caused by traffic accidents and violence. The positive effect of education on having more than one sexual partner may be linked to cultural and social factors. More educated people may not only have a greater knowledge on risky sexual behaviors, but also on how to avoid their negative effect on health. According to de Walque (2006) and Cutler and Lleras-Muney (2012), education increases the use of protection, but at the same time, it predicts more infidelity and less abstinence. It is worth mentioning, that the results differ by gender. In particular, education increases the probability of having risky sexual behaviors in men, whereas in women the opposite occurs. These results could be explained by traditional gender attitudes still rooted in countries like Colombia, such as machismo. For example, women are judged more harshly for having casual sex (England & Bearak, 2014).
Table 2 Effect of Socioeconomic and Knowledge Variables On Education Gradients (OLS estimates)
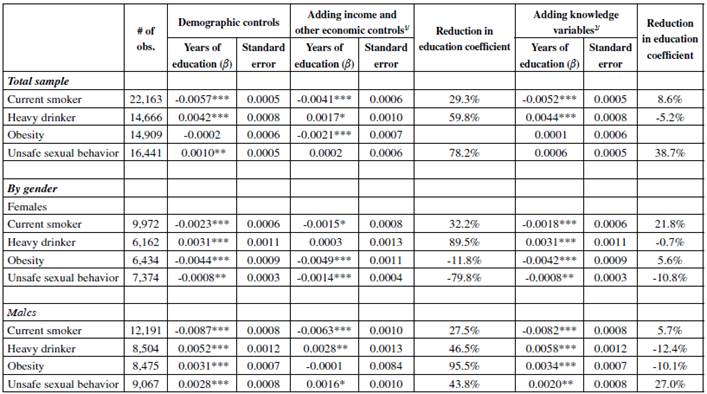
*** p < 0.01, ** p < 0.05, * p < 0.1
1/ The variables included are: income, marital status, contributory health regime, the region where the individual lives (Bogotá, Andean region, Pacific region, Caribbean region), labor force participation, and o vercrowding. See Appendix A for a description of the variables.
2/ Dummy variables were included to account for the knowledge of individuals about health risks.
3/ Percentage change in the education coefficient of the basic re gression.
4/ The reduction in the education coefficient is not calculated when this coefficient is not statistically significant in the basic equation.
Source: Authors’ calculations.
The direction of the effects by gender are very similar to those obtained by using the complete sample in the case of current smoking and heavy drinking (Table 2). We found contrasting results for males and females regarding the impact of each additional year of education on the probability of being obese and having more than one sexual partner during the last 30 days. For females, these effects are negative, whereas for males they are positive, highlighting the importance of education to reduce the incidence of these behaviors in women.
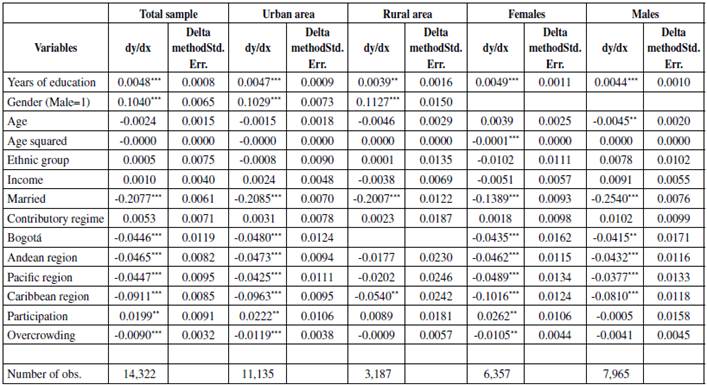
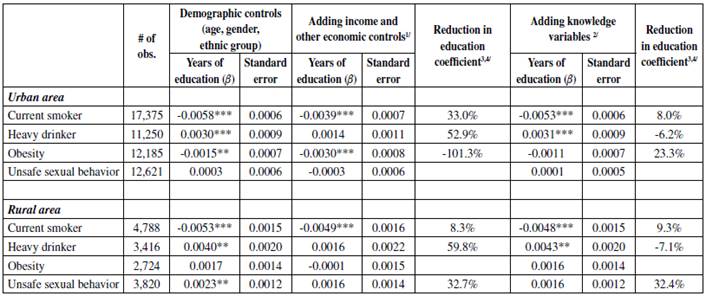
In addition, it is important to take into account the area of residence, given the significant differences observed in years of schooling between the urban and rural areas. In particular, in our sample, the average years of education in urban areas is 8 years, while in rural areas it is 5 years. The main differences are observed in obesity and unsafe sexual behavior. While for individuals in urban areas education negatively affects the probability of being obese, whereas education is not significant in rural areas. In the case of unsafe sexual behavior, in urban areas education does not affect the probability of having more than one sexual partner during the last 30 days, whereas in rural areas its effect is positive (Table 3).6
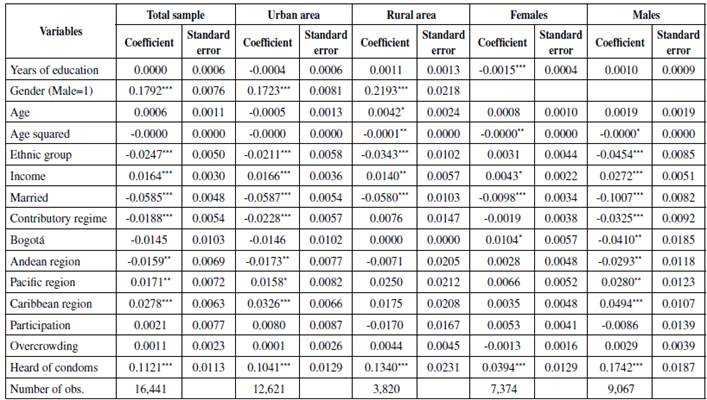
Table 3. Effect of Socioeconomic and Knowledge Variables On Education Gradients by Area of Residence (OLS estimates)
*** p < 0.01, ** p < 0.05, * p < 0.1
1/ The variables included are: income, marital status, contributory health regime, the region where the individual lives (Bogotá, Andean region, Pacific region, Caribbean region), labor force participation, and o vercrowding. See Appendix A for a description of the variables.
2/ Dummy variables were included to account for the knowledge of individuals about health risks.
3/ Percentage change in the education coefficient of the basic re gression.
4/ The reduction in the education coefficient is not calculated when this coefficient is not statistically significant in the basic equation.
Source: Authors’ calculations.
Next, income and other socio-economic variables were added to the basic equation (equation 2). The results show that these variables account for some of the education effect (Table 2). For instance, the coefficient on years of education in the current smoking equation falls by 29%. In addition, in the heavy drinking equation, this coefficient falls by 60%, which is much higher than the result obtained by Cutler and Lleras-Muney (2010) for the United States (13%), indicating that, in Colombia, more than half of the effect of education on the probability of heavy drinking is mediated by income and other socio-economic variables. The education coefficient on the equation for unsafe sexual behavior falls by 78%, indicating that almost two-thirds of the effect that education has on the probability of having more than one sexual partner during the last month is mediated by income and other socio-economic variables. The high reduction in the education gradient for heavy drinking and risky sexual behavior highlights the importance of socioeconomic variables.
For females, in the case of current smoking, results are similar to those obtained for the complete sample (Table 2). The differences arise in the case of heavy drinking, where the coefficient of education does not differ from zero when adding these variables, which could be due to a correlation between income and education. In the case of obesity and unsafe sexual behavior, including socioeconomic variables in the basic equation increases the education gradient by 12% and 80%, respectively, indicating an opposite effect to that of education. For males, the reduction in the education gradient for smoking, heavy drinking and unsafe sexual behavior is similar to the one found for the complete sample. Meanwhile, the inclusion of socio-economic variables in the equation for obesity makes the education coefficient insignificant.
By area of residence, the mediating effect of the socio-economic variables is higher in the case of individuals living in urban areas (Table 3). The presence of socioeconomic variables in the heavy drinking equation renders the education variable insignificant, in both urban and rural areas. In urban areas, the education gradient increases after socio-economic variables are added, emphasizing the role of these variables on the probability of being obese. In rural areas, these variables reduce the positive effect education has on the probability of having more than one sexual partner during the last 30 days.
Lastly, knowledge variables were added to the basic equation (Table 2). In the case of smoking, the survey asks about their knowledge on the risk of cancer, chronic cough, the effect on unborn children, and advertising. Results indicate that adding these four variables reduces the coefficient on years of education in the current smoking equation by 9%, indicating that the probability of smoking is mediated by knowledge variables. In the case of heavy drinking, the survey includes information on the age at which the individual started drinking or first drank, which may have an impact on alcohol dependence. Also, the survey asks about the awareness of individuals on the harmful effects of alcohol consumption. Conversely to the case of smoking, including these variables increases the coefficient on education by 5%, indicating that these knowledge variables have the opposite effect of education on the probability of heavy drinking, contributing to reduce its incidence. In the case of unsafe sexual behavior, the survey asks about the individual's know-ledge on the use of condoms; the inclusion of this variable reduces the coefficient on education by 39%. As mentioned, in this behavior, unlike the others, know-ledge variables could increase the likelihood of engaging in unsafe sexual behaviors, such as having more than one sexual partner. In particular, knowledge and use of condoms could prevent negative health effects.
For women, the effect of education on the probability of current smoking and obesity is mediated by knowledge variables, since the coefficients reduce by 22% and 6%, respectively (Table 2). On the contrary, the inclusion of these variables in the heavy drinking and unsafe sexual behavior equations does add a little to the explanation of the education effect. For males, in the case of smoking, the education gradient reduces by 6%. For obesity and heavy drinking, adding knowledge variables increases the education gradient, offsetting the positive effect of education on the probability of being obese and heavy drinking.
In both rural and urban areas, the inclusion of knowledge variables offset the positive effect of education on the probability of heavy drinking, highlighting the importance of the age at which the individual started drinking or first drank and of the knowledge about the detrimental effect of heavy alcohol consumption on one's health (Table 3). Regarding obesity, the education gradient reduces by 23% in urban areas, indicating the importance of exercising to reduce the probability of being obese.7 For unsafe sexual behavior, in rural areas, the education gradient reduces by 32%, indicating that knowledge about condoms increases the probability of this risky behavior.
The Effect of Education and Other Covariates
We also estimate the effects of the socio-economic and knowledge variables on each risky health behavior (equation (4)) using logit models for the complete sample, by area of residence and by gender.8
Smoking
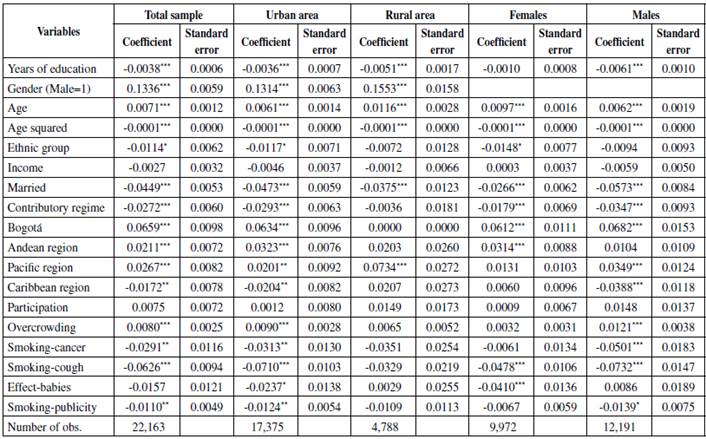
When considering socio-economic and knowledge variables altogether, education remains negative and significant, except in the case of women (Table 4). The probability of current smoking is higher for men than for women in both urban and rural areas. This probability increases with age until about 53 years old, when it starts to decrease. In rural areas, this probability begins to decline later in life (60 years old); this could be partly explained by the lack of effect of the knowledge variables, highlighting the importance of education to reduce the incidence of this risky behavior.
Table 4 The Impact of Education and Other Co variates On the Probability of Current Smoking: Logit Estimation
*** p < 0.01, ** p < 0.05, * p < 0.1
Source: Authors’ calculations.
Being married reduces the probability of current smoking in all cases; this result could be influenced by the negative effect secondhand smoke exposure has on the partner's health, which could affect an individual's decisions about smoking (see for example, United States Department of Health and Human Services, 2006). Also, being affiliated to the contributory health regime reduces this probability in all cases, except for individuals who live in rural areas where it is more common to be affiliated to the subsidized regime, which, by the time the survey was carried out, had a basket of services that was different to that of the contributory regime. Interesting differences are observed among regions of the country. In the full sample, inhabitants of the Caribbean region are less likely to be current smokers than individuals living in the rest of the country. The same behavior is observed when the analysis is performed for individuals in urban areas and for men. For women, only those living in the Andean region and the capital of the country (Bogotá) have a higher probability of smoking that those living in the rest of the country.
Regarding knowledge variables, they negatively affect the probability of current smoking, indicating that campaigns and studies on the negative effects of smoking have raised awareness about how harmful smoking is. In the case of women, campaigns on the harmful effects of smoking during pregnancy seem to have been quite effective, reducing this probability significantly (e.g., Cornelius & Day, 2000). Moreover, the WHO (2013) highlights the importance of campaigns against smoking. However, when estimations are carried out by area of residence and gender, it is observed that for women living in rural areas, these knowledge variables do not have a significant effect on reducing the probability of smoking.9 Lastly, it is worth mentioning that individual income does not significantly affect the probability of current smoking. Since it is a bad habit, its consumption might not be tied to income.
Heavy Drinking
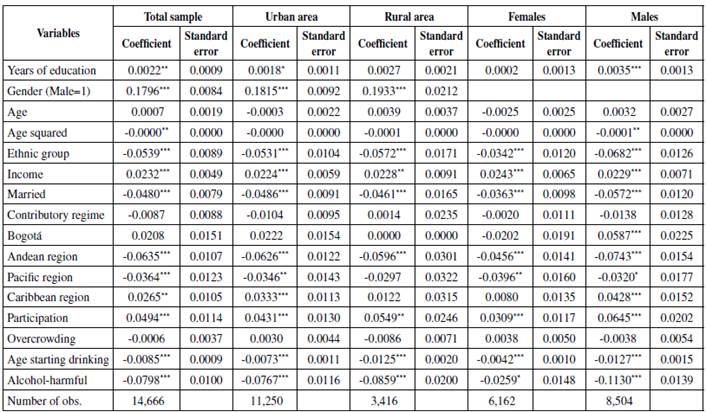
Results do not show significant differences when the estimations are carried out by gender and area of residence. Education has a positive and significant effect on the probability of heavy drinking for the complete sample, for individuals living in urban areas, and for males (Table 5).
Table 5 The Impact of Education and Other Co variates On the Probability of Heavy Drinking: Logit Estimation
*** p < 0.01, ** p < 0.05, * p < 0.1
Source: Authors’ calculations.
Similarly to smoking, men are more likely to be heavy drinkers than women, due mainly to cultural factors (see The Social Issues Research Centre, 1998). Contrary to the case of current smoking, income and labor force participation have a positive and significant effect on the probability of heavy drinking.10 Similarly, for developed countries, the WHO (2014b) mentions that there are more drinkers in higher socio-economic groups; moreover, this report also suggests that in lower socio-economic groups people are more susceptible to the consequences of alcohol abuse. Results also indicate that ethnicity is an important factor in determining the probability of heavy drinking, which is consistent with other studies that find differences in alcohol consumption between ethnic groups within countries.
The probability of heavy drinking is lower for married individuals. Alcohol consumption can have both health and social consequences, not only for the drinker, but also for other individuals (such as family members or friends). Hence, the possible negative consequences of heavy drinking on others may reduce the probability of drinking for individuals living with a partner. In addition, individuals living in the Caribbean region have a higher likelihood of heavy drinking than those in the rest of the country, when the estimations are carried out for the complete sample, for individuals living in urban areas, and for males.
The age at which an individual started drinking has a negative and significant effect on the probability of heavy drinking. That is, the younger the individual started drinking, the higher the probability of becoming a heavy drinker. Regarding this, the WHO (2014b) states that: "... early initiation of alcohol use (before 14 years of age) is a predictor of impaired health status because it is associated with an increased risk for alcohol dependence and abuse at later ages..., alcohol-related motor vehicle crashes..., and other unintentional injuries (p. 7)." In turn, despite the fact that education increases the probability of heavy drinking, knowing about the harmful effects of alcohol reduces this probability.
Obesity
The analysis of this health behavior is important given that it is a major risk factor for some chronic diseases, including diabetes, cardiovascular diseases, and hypertension. According to the WHO (2014b), worldwide incidence of obesity almost doubled between 1980 and 2014, when 15% of women and 11% of men were considered obese. Moreover, the prevalence of obesity is not restricted to developed countries. Its incidence has been increasing in low and middle income countries, particularly in urban areas (WHO, 2015).
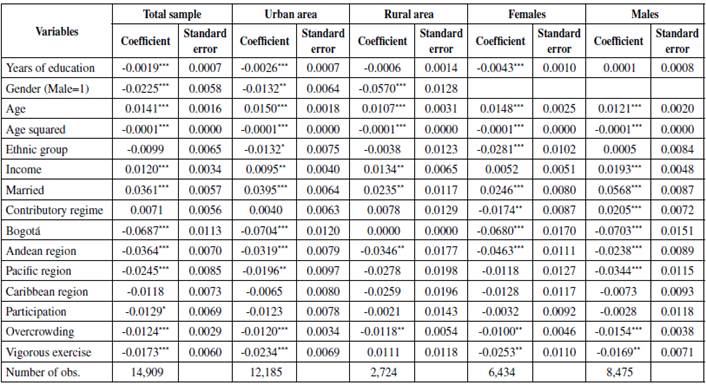
Regarding the effect of education, each additional year reduces the probability of becoming obese for the complete sample, in urban areas and for women (Table 6), while for rural areas and men it is not statistically significant. The likelihood of becoming obese is higher for women than for men. This probability increases with age until about 51 years old for the complete sample, which could be related to muscle loss due to aging. However, differences are observed by gender. For women, the probability of being obese starts to decrease at 58 years old, whereas for men it starts to decline at 49 years old. In addition, results differ by ethnic group; this coefficient is only significant for women.
Table 6 The Impact of Education and Other Co variates On the Probability of Being Obese: Logit Estimation
*** p < 0.01, ** p < 0.05, * p < 0.1
Source: Authors’ calculations.
The probability of being obese also increases with income in the case of men.11 This probability is higher for married individuals than for singles, widows/widowers, or divorced people. Conversely, this likelihood is lower for individuals living in overcrowded conditions and for those living in Bogotá and the Andean Region, which could be related with differences in lifestyles. Lastly, vigorous exercise reduces the probability of becoming obese. This result is consistent with the findings of the WHO (2010) which point out that physical activity is a key determinant of weight control.
Risky Sexual Behavior
Risky sexual behaviors could increase the incidence of sexually transmitted diseases (including HIV), cervical cancer, and unwanted pregnancies. Interestingly, only in the case of women, every additional year of education reduces the probability of engaging in risky sexual behavior (Table 7). Consequently, education is an important tool to enhance female sexual and reproductive health, which could also result in lower maternal and neonatal mortality and morbidity rates.
Table 7 The Impact of Education and Other Co variates On the Probability of Having Risk y Sexual Behavior: Logit Estimation
*** p < 0.01, ** p < 0.05, * p < 0.1
Source: Authors’ calculations.
The probability of having more than one sexual partner during the last month is higher for men than for women and lower for married individuals.12 There are also differences by ethnic group and region of residence. For example, residents in the Caribbean and Pacific regions have a higher likelihood of risky sexual behavior, especially in the case of urban areas and males. Furthermore, income has a positive and significant effect on this risky behavior, whereas for those living in urban areas and males, being affiliated to the contributory health social security regime has a negative effect on the probability of this risky behavior. This last result could be associated with more effective campaigns aimed at reducing the incidence of disease and unwanted pregnancies. As mentioned, the knowledge about condoms increases the probability of this risky behavior, once again highlighting the importance of cultural factors.
FINAL REMARKS
This paper analyses the relationship between education and four risky health behaviors, namely smoking, heavy drinking, obesity, and unsafe sexual behavior for Colombia. To this end, we assess the effect of socio-economic variables and some indicators about the knowledge on these risky behaviors by means of the education gradients. We also provide evidence on the effects education and other covariates have on these health behaviors by gender and area of residence.
The results of the education gradient indicate that years of schooling negatively and significantly affect the probability of smoking. Conversely, the probabilities of heavy drinking and having unsafe sexual behavior increase with education; meanwhile, there is no significant effect of education on the probability of being obese. These findings suggest that in Colombia, education has helped reduce the incidence of smoking, but not that of alcohol consumption, which could be explained by cultural and social factors and/or by the failure to acknowledge the harmful effect alcohol abuse has on health. The positive effect of education on unsafe sexual behavior may also be related to cultural and social factors. People who are more educated may have, not only more knowledge on risky sexual behaviors, but also on how to avoid its negative influence on one's health.
Income and other socio-economic variables account for some of the education effect. In particular, there is a large reduction in the education gradient for heavy drinking and risky sexual behavior, highlighting the importance of socioeconomic variables in Colombia. Moreover, when knowledge variables are included, the results indicate that the coefficients of education in the smoking and unsafe sexual behavior equations fall. Conversely, the inclusion of knowledge variables in the heavy drinking equation increases the coefficient on education, indicating that these variables contribute to reduce its incidence.
In a second exercise, we characterize each risky health behavior using logit models, taking into account socio-economic and knowledge variables altogether. The results show that being married reduces the probability of current smoking, heavy drinking and having unsafe sexual behavior, due to the negative consequences that these behaviors could have on family members. In general, the probability of engaging in these risky behaviors increases with age, up to a certain age, when it starts to decline. Knowledge variables reduce the probability of smoking, heavy drinking and obesity, indicating that campaigns and research on the negative effects of these behaviors raised awareness about how harmful they are.
The evidence presented in this paper highlights the importance of education and knowledge about the negative effects of these risky behaviors on one's health. Since there are significant differences in education by area of residence, it is important for public policy to increase the years of schooling in rural areas. Regarding knowledge, in the case of smoking, campaigns have proven to be successful in reducing the incidence of this risky behavior, especially in the case of women, since campaigns on the harmful effects of smoking during pregnancy seem to have been quite effective. In the case of heavy drinking, results indicate that although its incidence could be highly linked to social and cultural factors, knowledge about its harmful effects contributes to reduce the probability of drinking heavily. Moreover, physical activity should be promoted, since it is a key determinant of weight control and it helps to curb the risk of some chronic diseases. In this sense, Law 1355 of 2009 was enacted in order to adopt measures to control, prevent, and treat obesity and non-communicable chronic diseases associated with it as a public health priority.
Public policy should continue implementing policies aimed at reducing the prevalence of risky health behaviors since they are a major source of mortality and morbidity associated with chronic and sexually transmitted diseases, as well as an important source of demand for health services.
Finally, it is important to mention that in this paper we evaluate neither the joint effect of all behaviors nor the effect that one risky behavior may have on another one. For example, we do not take into account if smoking may increase the probability of drinking alcohol, or vice versa. In addition, due to the lack of suitable data, it was not possible to gather information on other forms of unsafe sexual behaviors in order to further our understanding of their relationship with education.