











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Background
Daily calcium intake below the necessary daily requirements has been linked to low vitamin D (Vit-D) and the appearance of osteoarticular diseases, osteoporosis, and fractures, among others 1-3.
Calcium and Vit-D influence metabolic and immunologic processes and their deficiency has also been linked to the occurrence of connective tissue diseases such as systemic lupus erythematosus and rheumatoid arthritis 4-6. There are two fundamental pillars in achieving adequate skeletal health: calcium levels and the preponderant role of Vit-D 7-10, although some researchers have recently discussed their role in therapeutics, specifically, their osteoprotective action 11-13.
Hypovitaminosis D appears in the context of a multifactorial model caused by changes in lifestyle, eating habits, sleep patterns, and other conditions produced by stress. This combination of factors may end up in connective tissue pathology, with syndromic features, predominantly affecting young or post-menopausal women 14.
The environmental conditions related to the geographical location are determinants that establish social and cultural patterns: apparel type and walking to work directly influence the degree of sunlight exposure, a necessary physiological component for Vit-D production. Interaction between these variables and those derived from lifestyle, eating habits, age, and sex transform into a risk formula that impacts the incidence or prevalence of Vit-D deficiency 15,16.
This diagnosis is common in Asian countries where 96 % of infants, 91 % of schoolgirls, 78 % of health professionals, and 84 % of pregnant women suffer from this condition; in Europe, between 2-30 % of the adult population and 75 % of older people showed Vit-D deficiency, most often in men 16. In North America, the NHANES HI study identified a relationship between calcium intake and Vit-D deficiency, and low levels were found in 23 % of men, 56 % of women between 20-70 years old, and 97 % of older people 17.
In Latin America, even if there is weak evidence, the perspective is consistent. In Mexico, Chile, and Brazil, the incidence of Vit-D deficiency in the general population ranges between 42-67 %. In Colombia, there are studies only in post-menopausal women and patients with renal and metabolic diseases, reporting frequencies of 55 % and 92 %, respectively 18,19. There are no studies in the general population in Colombia, a country located in the tropics with a variety of climate zones and sociocultural patterns that may predispose inhabitants to the occurrence and prevalence of this condition.
Therefore, this study aims to determine the prevalence of Vit-D deficiency in a specific group of people in Bogotá, its relationship to dietary calcium intake, and the influence of sociodemographic factors and sunlight exposure.
Materials and methods
Design and place of study
A prospective descriptive study was conducted in the School of Medicine at the Fundación Universitaria Juan N. Corpas (FUJNC) in Bogota, Colombia, which also has a University Hospital (Juan N. Corpas Hospital) that together with other entities forms the Corpas Social Group (CSG). It has around 3,084 people, including students, faculty, staff, clinical, and services personnel; most of them study and work during daylight, except those who provide security services. The study was approved by the FUJNC Ethics and Research Committees (Code of Ethics Committee approval).
Selection of participants and collection of information
Consecutively, in November 2016, participants were selected randomly; with the benchmark of hypovitaminosis D in 76.9 % of post- menopausal women, we calculated a sample of 66 participants to achieve 95 % CI, with 10 % amplitude and a 5 % margin of error 19.
Two surveys were designed to collect data; the first one contained sociodemographic, anthropometric variables, and exclusion criteria; the second one, items to estimate daily dietary calcium intake and body sunlight exposure.
Individuals between 18-70 years old were included, who belonged to the CSG during the established study period, signed informed consents, and kept the required fast for sampling. Exclusion criteria were people with a Body Mass Index (BMI) < 16 or > 35, consumption of mineral or vitamin supplements, a Charlson Index > 2, surgical history (endocrine or gastrointestinal) that affects calcium absorption or Vit-D action; autoimmune or rheumatic diseases, osteoporosis, osteomalacia, stage C or D heart failure, dysthyroidism venous thromboembolism; treatment with loop diuretics, corticosteroids, antiplatelet or anticoagulant agents; lack of monitoring, and problems when filling questionnaires.
Surveys were administered by fifth-year medicine students previously trained and supervised by three researchers (AAT, LMP, LGP). The information related to calcium intake was collected with open questions asking to describe the food eaten the day before the interview.
A week before and during the collection phase, CSG staff and patients attending the outpatient unit were informed of research and the need for fasting from 8 to 12 hours to ensure their inclusion, in case of being selected at random.
Information related to age, sex, weight, height, occupation, working hours, socioeconomic status (SES), and monthly income was collected; the calcium intake data was converted into mg/day using the Food Frequency Questionnaire/Recall Method instrument, validated for the Colombian population 20,21. Immediately after filling out the instruments, between 07:00 and 09:00 hours, the blood sample was frozen at -20 ° C and processed at < 12 hours to measure serum calcium (mg/dL) and collected Vit-D (ng/mL), both of them through the chemiluminescent immunoas-say technique (Biolmagen).
The second survey was carried out by phone on the third and fifth day after the first evaluation to calculate the average daily calcium intake during a week.
The hours of sunlight exposure were determined by calculating the weekly average in three evaluations at different times; we asked about the daily use of clothing to determine the number of sun-exposed body parts: 0 (none), 1 (only one area exposed: face, back, upper or lower area) and > 1 (more than one area exposed: face, back, upper or lower area).
Outcome measures
Individuals were classified as having adequate, insufficient, or deficient levels of Vit-D to determine the prevalence of hypovitaminosis 22.
The average daily dietary calcium intake was compared to that suggested for the Colombian population 23,24.
Also, the relationship between Vit-D concentration, sociodemographic, anthropometric, and physiological variables, and sunlight exposure was evaluated.
Statistical analysis
Minitab-V17 software was used to present and analyze the results. Data were expressed as means, medians, and proportions (95 % CI); normality was determined with the Shapiro Wilks test. Continuous data comparisons for two independent groups were performed using the U Mann-Whitney test or Kruskal Wallis for three or more independent groups. Categorical data were compared with the chi-square test (x2); p < 0.05 (two-tailed) was established as significant.
Following a univariate analysis, which identified variables related to Vit-D concentration (p < 0.2), a multiple regression model that evaluated the most favorable interaction was run to predict Vit-D concentration. The model was applied without the intercept, steps forward, and included variables with p < 0.05.
Results
During the study, 106 potential participants were evaluated, six were excluded for not meeting the inclusion criteria, two for not monitoring their food consumption, and one due to a technical failure while processing laboratory samples (Figure 1).
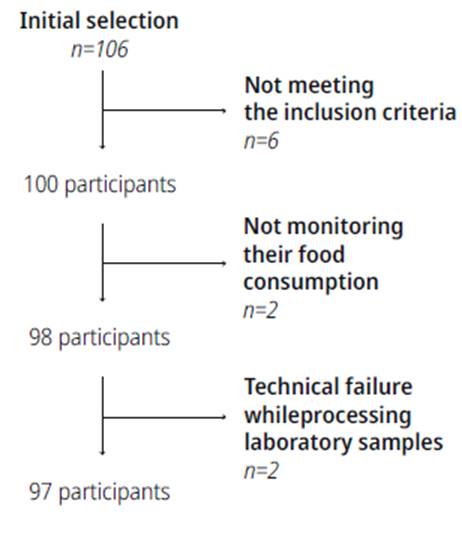
Ninety-seven subjects were included, most of them with a median age of 23, 60.8 % were women, 36 % belonged to middle SES, 83 % worked in the health field, and 47.7 % had a monthly income between 1-2 statutory minimum wages (Table 1).
Table 1 Sociodemographic Features of Participants
| Baseline features | n: 97 |
|---|---|
| Age, median (Q1-Q3) | 23 (22-31) |
| Sex, n (%) | |
| Female | 59 (60.8) |
| Male | 38 (39.2) |
| SES, n (%)a | |
| Low | 33 (34.0) |
| Medium | 35 (36.1) |
| High | 29 (29.9) |
| Occupation, n (%) | |
| Health care | 80 (83.3) |
| Sales and services | 13 (13.5) |
| Finance and administration | 3 (3.1) |
| Monthly income, n (%) | |
| ≤ 1 SMMLV | 7 (7.2) |
| > 1-2 SMMLV | 46 (47.4) |
| > 2-4 SMMLV | 20 (20.6) |
| > 4 SMMLV | 24 (24.7) |
Q1: p25; Q3: p75; SES: Socioeconomic status, low 1-2, medium 3-4, high 5-6; SMMLV: Statutory monthly minimum wage in force; a: No significant differences were found between participants by SES.
Source: Own elaboration.
Anthropometric and physiological characteristics
Two of the three anthropometric variables and all physiological variables showed skewed distributions; the results were analyzed according to the SES, given the influence of this condition the studied variables. No differences in weight, bmi, intake, or serum levels of calcium and Vit-D were found when comparing ses subgroups. Subjects belonging to low ses showed shorter height (mean ± sd) compared to the other two subgroups, but no influence on bmi (p= 0.001) (Table 2). Further analysis between levels of monthly income or physiological and anthropometric variables was performed, and no relationship was found (Table 3).
Table 2 Anthropometric and Physiological Features of Participants
| Features | High SES | Medium SES | Low SES | Total | p-Value |
|---|---|---|---|---|---|
| Weight (kg)a | 65 (59.5-77.5) | 62 (53-75) | 61 (55.3-67) | 62 (55.2-70.5) | 0.152 |
| Height (cm)b | 168.5 ± 7.3 | 168.1 ± 8.9 | 161.2 ± 8.7 | 165.9 ± 8.9 | 0.001 |
| BMI (kg/m2)a | 24 (21.5-25.8) | 22.2 (20.7-24.2) | 23.1 (21.3-25.1) | 22.8 (21.2-25.2) | 0.244 |
| Calcium intake (daily mean)a | 345.7 (281.8-515) | 441.3 (304-597.3) | 362 (282.8-457.5) | 393.7 (291.8-525) | 0.154 |
| Serum calcium (mg/dL)a | 9.7 (9.5-9.9) | 9.8 (9.5-9.9) | 9.7 (9.4-9.9) | 9.7 (9.4-9.9) | 0.847 |
| Vitamin D (ng/mL)b | 23.6 ± 4.3 | 23.9 ± 4.9 | 23.5 ± 5.8 | 23.7 ± 5.02 | 0.947 |
SES: Socioeconomic status; a: median (p25-p75); b: mean ± so; BMI: Body mass index. The median differences were established using a Kruskall-Wallis test and ANOVA.
Source: Own elaboration.
Table 3 Relationship between Vit-D Concentration and Sociodemographic, Anthropometric, Physiological, and Sunlight Exposure Characteristics.
| Characteristics | p-Value |
|---|---|
| Sex | 0.196ª |
| Age (years) | 0.417 |
| Occupation | 0.821 |
| SES | 0.947 |
| Monthly income (smmlv) | 0.170ª |
| Weight (kg) | 0.915 |
| Height (cm) | 0.454 |
| BMI (kg/m2) | 0.436 |
| Calcium intake (mg/day) | 0.068ª |
| Serum calcium (mg/dL) | 0.022ª |
| Sunlight exposure (hours) | 0.615 |
| Sun-exposed body parts | 0.194ª |
a: Characteristics with p-value < 0.2 will be evaluated using an interaction model.
Source: Own elaboration.
The daily calcium intake (mg/day) in each of the SES and overall was lower than the recommended for the Colombian adult population (800 mg/day) (Wilcoxon test, p < 0.001); median (p25-p75) intake in men and women was 348.2 mg/day (285.4536.7) and 408.3 mg/day (296-520.3), respectively, both being lower than that recommended for our population (Table 2).
Frequency of hypovitaminosis D
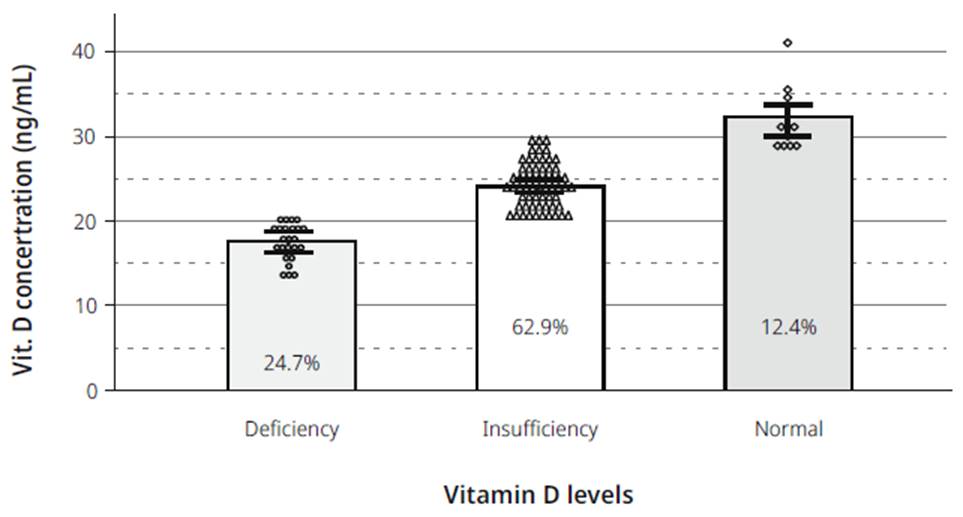
Some degree of hypovitaminosis D was identified in 87 % of individuals: 24.7 % were classified as deficient (95 % CI, 15.6- 33.8 %), 62.9 % as insufficient (95 % CI, 52.8-73 %), and 12.4 % as sufficient (95 % CI, 5.3 %-19.4 %). The average Vit-D concentration (ng/mL) (95 % CI) was 17.6 (16.8-18.4) in the deficient group, 24.3 (23.7 to 24.7) in the insufficient group, and 32.7 (30.6 to 34.8) in the sufficient group (Figures 2 and 3).
Source: Own elaboration.
Figure 2 Vit-D concentration and Hypovitaminosis D prevalence. Vit. D: Vitamin D; Deficient: [Vit-D] < 20 ng/mL; Insufficient: [Vit-D] 21-29 ng/mL; Normal: [Vit-D] ≥ 30 ng/dL.

Factors related to Vit-D concentration
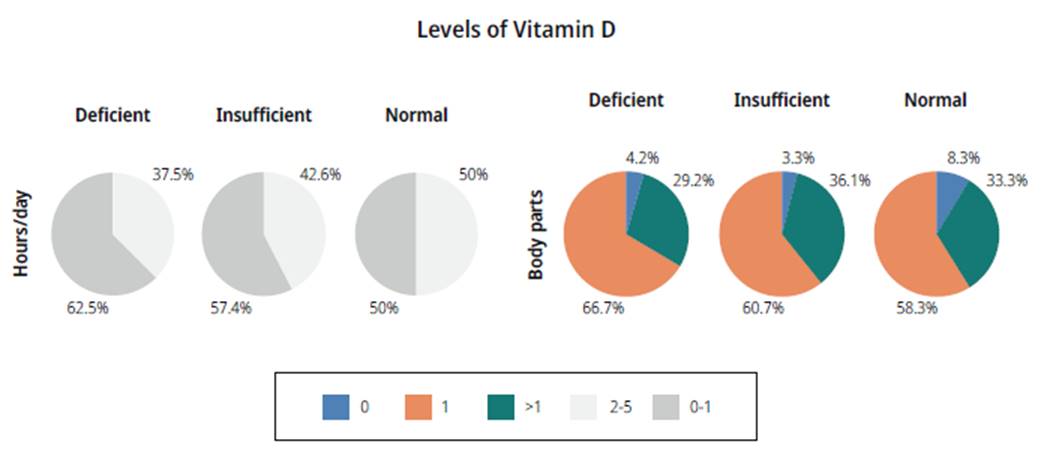
About half of the individuals (50/97; 51.6 %) reported daily sunlight exposure ranging between 2-5 hours; the others had one hour (44/97; 45.4 %) or no hours during the day (3/97; 3.1 %). Most of the people exposed one complete body part only (57/97; 58.8 %), followed by those who exposed more than one part (36/97; 37.1 %). A trend related to the hours of daily sunlight exposure, the number of body parts exposed, and the levels of Vit-D was identified, showing no statistical relationship between variables (Figure 4).
Source: Own elaboration.
Figure 4 Daily sunlight exposure and serum Vit-D. Sunlight exposure: 0-1 hours, 2-5 hours; Sun-exposed body parts (hours/day): 0, 1, > 1 parts.
The univariate analysis showed that the variables with a < 0.2 statistical relationship were sex, monthly income level, calcium intake, serum calcium, and the number of daily sun-exposed body parts.
Interaction between calcium intake and the number of daily sun-exposed body parts was identified with differences when stratifying between men and women (p < 0.05); men had a higher concentration of Vit-D, preferably when consuming higher levels of dietary calcium (Figure 5).

Source: Own elaboration.
Figure 5 Vit-D concentration related to calcium intake, sunlight exposure, and sex. SEBP: Sun exposed body parts; R2 Men, 0-1 SEBP: 96.2 %; R2 Men, > 1 SEBP: 98 %; R2 Women, 0-1 SEBP: 94.2 %; R2 Women, > 1 SEBP: 94.1 %.
Dietary calcium intake was divided into quartiles: < 291.8 mg/day (p25), > 291.8-393.7 mg/day (p50), > 393.7-525 mg/day (p75), and > 525 mg/ day. Table 4 details the equations of the regression model.
Table 4 Prediction of Vit-D Concentration Related to Calcium Intake Level, Sunlight Exposure, and Sex
| Factor | Equation |
|---|---|
| Man | |
| Sunlight exposure | |
| 0-1 | 20.0 * calcium intake level - 3.461 * calcium intake level2 |
| >1 | 21.75 * calcium intake level - 3.739 * calcium intake level2 |
| Woman | |
| Sunlight exposure | |
| 0-1 | 18.39 * calcium intake level - 3.372 * calcium intake level2 |
| >1 | 20.92 * calcium intake level - 3.716 * calcium intake level2 |
Sunlight exposure: Sun-exposed body parts; Calcium intake level: Level 1 (≤ p25), level 2 (> p25-p50), level 3 (> p50-p75), level 4 (> p75). The regression model was adjusted to a quadratic function.
Source: Own elaboration.
Discussion
This research determined the prevalence of hypo-vitaminosis D among healthy individuals in a specific group of participants; it also contrasted the regular dietary calcium intake with the minimum required for adults and identified possible factors related to Vit-D concentration.
The place of selection of participants allowed identifying individuals with different SES and classify them randomly; this relationship was found in nutritional studies involving biochemical variables 25. In CSG institutions, the activity of their members is related to the provision of health care services, and due to their educational background, they would be expected to apply their knowledge of daily nutritional requirements to their self-care.
Finally, it is noteworthy that, among the participants, no individuals belonged to indigenous communities and other special groups with specific nutritional habits that could influence biological markers.
In general, dietary calcium intake was two times lower than the established for Colombian adults, according to the National Statistics Department; some of the most frequently consumed foods in Bogota are bread, cereals, milk, cheese, and eggs, all of them between 17-212 mg of calcium per 100 grams 26. The research was conducted in a Latin population, two of them in Bogotá, which included only women and students of a public university, respectively, and they were consistent with low dietary calcium intake (27, x, y 19-21). Research with women included staff not related to the health field and the condition of patients, without excluding those with conditions limiting calcium intake, absorption, or metabolism. In the study with university students, more than 90 % had breakfast and homemade food, but lunch, an important source of calcium-rich foods, was bought at restaurants, without specifying the type of food eaten at the time.
It was identified that at least eight of ten participants had some level of hypovitaminosis D. A systematic literature review that included 243 publications involving the Latin population determined a deficiency in < 1 %. Mexico, the only country with nationally representative samples, showed a prevalence of inadequacy between 8-24 % 28. The cut-off points of hypovitaminosis D categories were different than the ones defined for this research, and the population groups included people < 18 or > 40 years old, factors related to the diagnosis and classification of hypovitaminosis D.
The interaction between sex, level of calcium, and degree of sunlight exposure was a non-linear triad predictor of Vit-D concentration. Physiologically, these variables influence the homeostasis process of Vit-D 23-28; besides, each of these factors has been associated, individually or combined, with Vit-D concentration using prediction models 29-32. It is clear that most of the models were uni- or bivariate except for the Sohl model, which included between 10 and 13 predictors and, unlike our research, did not take into account the usual calcium intake or sun-exposed body parts 33.
This research did not measure Vit-D intake within the usual diet nor the consumption of antacids or laxatives, factors directly related to serum levels or absorption of Vit-D. One of the strengths of the design is the consecutive and random selection of participants, which took into account the SES and allowed including equitably subjects belonging to low, medium, and high socioeconomic levels 34.
Recent studies have not been convincing when trying to associate the calcium content in the diet or calcium supplements with cardiovascular complications 35-41. Moreover, discoveries about the pleiotropic effect of Vit-D in the body, as a result of multiple receptors in different tissues, transformed the conception of this vitamin, from a simple nutritional supplement to a biomolecule with hormonal properties, in which appropriate serum levels are a reflection of homeostasis in humans 42-50.
This new information increases the relevance of population studies like ours because, when rigorously assessing the calcium intake in a population and its relationship to the levels of Vit-D, they reveal a health problem that may impact various human diseases, including those affecting the osteoarticular system.
Given the results obtained, a high prevalence of Vit-D deficiency among the general Colombian adult population is confirmed, and it is also related to low daily dietary calcium, demographic factors, and sunlight exposure.

