











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
SINCE THE case of Phineas Gage (Harlow, 1868), studies of humans with focal brain damage have produced a unique and fundamental insight into the cognitive functions that are served by the prefrontal cortex (PFC) (Schneider & Koenigs, 2017). The PFC is vital for human social cognitive and moral judgment processing (Forbes & Grafman, 2010). It is comprised of several regions that are associated with reward, motivation, and cognition (Haber, 2016).
The entirety of PFC, including its prefrontal region, is "action cortex" in the broadest terms. It is cortex devoted to action of one kind or another, whether skeletal movement, ocular movement, the expression of emotion, speech, or visceral control; it can even be the kind of internal, mental, action that we call reasoning (Fuster & Geffen, 2008). The PFC can be parsed into dorsolateral (dlPFC), ventrolateral (VIPFC), dorsomedial (dmPFC), ventromedial (vmPFC), and orbitofrontal (OFC) regions (Forbes & Grafman, 2010).
The dlPFC is a hub for executive control processes and it is one of the regions involved during emotion regulation. It plays a critical role in response preparation, goal maintenance, and goal-directed cognition. Though we typically think of the dlPFC as an affect modulating region, it is also involved in the top-down generation of affective states (e.g., experiencing affect via mental simulation) (Helion, Krueger, & Ochsner, 2019; Palma & Horta, 2016).
The VIPFC is one of the primary regions involved in cognitive control and during emotion regulation. It is instrumental in implementing goal-directed behavior and guiding retrieval of relevant information from memory and in the "top-down" generation of emotion. It also plays a key role in response inhibition. The VIPFC has functional connections to the anterior insula, medial PFC, and dorsal regions of the lateral PFC (Morawetz et al., 2016; Silvers et al., 2017), underscoring its role in response selection based on the detection of internal states and influencing goal-directed cognition (Helion et al., 2019).
The dmPFC is a region that acts as a conduit between cognitive control areas and affect-triggering regions that play a role in both generating and regulating emotion (Helion et al., 2019). The vmPFC seems to be critically involved in coding the affective value of stimuli within the current situational and temporal context (Braunstein et al., 2017).
The OFC is considered together with the amygdala, as a hub of multi-modal association of information from other brain regions, whose action results in the choice of behaviors, emotions, and an autonomic response. It is responsible for representing the value of the stimulus-reinforcement association in terms of its value as a reward or punishment, as well as reversing the association when the context changes (Palma & Horta, 2016).
In the words of Forbes & Grafman (2010) regions as the OFC, the vmPFC, and the dlPFC are likely critical for evaluating current motivational and emotional states, situational cues, and for integrating this information within the context of current goal states and past experience. Through interactions among these regions, possibly at both implicit and explicit levels, humans can build immediate impressions of others, infer what others are thinking, and plan actions that are likely to facilitate a successful interaction with others, all within the context of social norms.
The region of interest in this case study is vmPFC. Injuries in vmPFC arise from several etiologies: acquired brain injury (ABI), as meningiomas, infections, subarachnoid hemorrhage (particularly from ruptured aneurysms in the anterior communicating artery), ischaemic stroke, and traumatic brain injury (TBI) (Schneider et al, 2017). Injuries in this brain region lead to cognitive and emotional deficits that interfere with the individual's ability to return to daily life (Mcdonald, 2013, p.231). In 1978, impaired ability for social perception was described as a key feature of changes observed after injury (Lezak, 1978).
One of the most recurrent lesions of the prefrontal cortex in Colombia is associated with stroke. According to the Ministerio de Salud y Protección Social - Colciencias (2015), the incidence of stroke is higher in older adults and in people with vascular risk factors. Cerebral ischemia represents 80% of strokes worldwide and almost 50% of neurological admissions at the local level (Muñoz-Collazos, 2010).
May et al. (2017) confirmed associations between emotion recognition and behavioral alterations resulting from any form of prefrontal cortex injury, providing partial evidence for models that propose emotion recognition as one of the prerequisites for proper social functioning. Underlying the literature is a central paradigm in social functioning that is affected when brain injury occurs: Social Cognition (sc), which in the specific words of Lieberman (2007) is defined as the ability to understand other people. sc allows us to predict the behavior of others, share experiences, and communicate effectively. As the human species depends on cooperation and competition to survive, it is argued that sc is an evolutionary imperative, converging in a high-level and independent development of non-social information processing skills (Adolphs, 2003 cited by Mcdonald, 2013). Consequently, a brain injury in vmPFC has an important impact on prosocial behavior causing cognitive, functional, affective, and relational alterations in the person who suffers it.
Method
Participants
Patient: 58-year-old male diagnosed with right lobe vmPFC due to cerebral infarction from anterior cerebral vein thrombosis. Evolution of less than five (5) years, without previous cognitive impairment or neurological history other than stroke. First episode of stroke, no neuropsychiatric history, drug or alcohol addiction. Patient attended at Fundación Liga Colombiana contra la Epilepsia (LICCE) Capítulo Valle del Cauca; health institution specialized in the diagnosis and management of neurological conditions. Controls: 10 healthy participants, with no history of neurological, cerebrovascular, hypertensive or neuropsychiatric disease, were selected and recruited from the University of the Valley Health Institute database. The sample was matched by age, gender, laterality, and schooling level.
Instruments
Neuropsychological Assessment. Institute of Cognitive Neurology (INECOJ Frontal Screening (IFS) (Zapata et al., 2019; Torralva et al., 2009): We evaluated Executive Functions (EF) by administering the INECO Frontal Screening (IFS) test. It assesses eight different domains of EF and has been used to evaluate frontal performance in injured patients. The IFS evaluates frontal lobe function as an index of the following sub-tasks: Motor programming, conflict instructions, verbal inhibition control, abstraction, backward digit interval, spatial working memory, and Go/No Go.
Addenbrooke's Cognitive Examination-Revised. ACER-COI: Version adapted and validated in Colombia by Ospina (2015) is a multi-domain test that evaluates key aspects of cognition, easy to administer and of short duration (between 15 and 20 minutes). The test initially incorporated the Mini-Mental State Examination (MMSE) and assessed 5 domains: orientation (10), attention (8), memory (35), verbal fluency (14), language (28), and visuospatial (5) with a total score of 100 (Ospina, 2015, p. 9).
Raven's Matrices. CPM "Coloured Progressive Matrices" - (Raven et al., 1988): A measure of relationship education ability, one of the main components of general intelligence and the 'g' factor.
The Trail Making Test A-B (TMT). (Reitan, 1958): TMT has been described as a visomotor tracking task with different processing demands for each part (Lezak, 1995). Part A requires the participant to draw a line as quickly as possible by joining consecutive numbers (1-25) arranged pseudo-randomly on an 8 X 11.5 inch page. In Part B, the participant draws a line that alternates between consecutive numbers and letters that are also pseudo randomly arranged on a page (1A-2B-3C...) (Stuss et al, 2001, p. 232).
Digits & Symbols (WAIS-III). This is a subtest of the Wechsler Adult Intelligence Scale in version III. The scores on this subtest contribute to IQ and index scores. The person being tested copies the symbols that are paired with numbers. Using a key, the individual draws each symbol under its corresponding number. The individual's score is determined by the number of symbols he or she correctly drew within the 120-second time limit (Wechsler, 1997 p. 88).
Affective Screening.Beck's Depression Inventory (BDI-II) (Beck et al., 1996): This is a self-report instrument composed of 21 items whose purpose is to measure the severity of depression in adults and adolescents aged 13 and older. Each item is evaluated according to a four-point scale, from 0 to 3. If an examinee made multiple choices for an item, the alternative with the highest value is used. The maximum total score is 63.
State Trait Anxiety Inventory (STAI). (Spielberger et al., 1970). According to Beckler (2010) the State Trait Anxiety Inventory (STAI) has been widely used in research and clinical practice. It comprises separate self-report scales to measure state and trait anxiety.
Mind Theory Assessment. Faux Pas Test (FPT) (Stone, Baron-Cohen, and Knight, 1998): It was originally developed in children and has been modified for use in dementia research. It measures the ability to understand what a person says and/or unintentionally produces a negative emotion in a third party and to attribute to the second party a lack of knowledge about certain information concerning the third party. The FPT assesses the emotional and cognitive inference aspects of TOM. Participants read or listen to social interactions between two or three characters and identify instances where the speaker has said or done something inappropriate (faux pas).
Reading Mind in the Eyes Test. (RMET) (Baron-Cohen, Jolliffe, Mortimore, & Robertson, 1997): Assesses participants' ability to derive basic and complex mental states after seeing a clipped image of the eye region. This test assesses the emotional inference aspect of TOM. The task consists of36 images of the eye region of a face. Participants are asked to choose which of the four words best describes what the person in each picture thinks or feels as well as what the sex of the person in the picture is.
Empathy Assessment. Interpersonal Reactivity Index (IRI) (Davis, 1983): Assesses multidimensional empathy. The IRI is a self-report questionnaire that contains four 7-item scales (two cognitive scales and two affective scales). The two cognitive scales are: (I) perspective taking (PT), that measures the reported tendency to spontaneously adopt the psychological point of view of others; (II) fantasy scale (FS), that measures the tendency to imaginatively transpose oneself into fictional situations (Shamay-Tsoory, 2009, p. 620). The two affective scales are the empathic concern (EC) and the personal distress scale (PD). The EC scale takes advantage of respondents' feelings of warmth, compassion, and concern for others. The PD scale assesses the self-oriented feelings of anxiety and discomfort that result from tense interpersonal environments (Shamay-Tsoory, 2009, p.620).
Procedure
A population of 68 subjects referred from the LICCE database with diagnoses derived from neurovascular diseases was analyzed. The call for the control group was made by invitation through a telephone call, and the volunteers were chosen in a targeted manner ensuring compliance with the defined inclusion criteria.
Both patient and controls were evaluated in a single session. The patient in the LICCE facilities and the controls in the Neuropsychology Laboratory of the Universidad del Valle. Detailed information of the study was explained and presented. They then read the informed consent, indicated their understanding and accepted the terms of the research. They were given the opportunity to ask questions, then signed the consent form as stipulated by the Declaration of Helsinki and finally proceeded with the application of the neuropsychological and sc assessment protocol that was approved by the local ethics committee of the University.
Data analysis:
A modified version of the Student т-test was used to compare patient performance with a control sample. "This methodology allows the assessment of significance by comparing multiple individual's test scores with norms derived from small samples. This modified test is more robust for non-normal distributions, presents low values of type I error, and has already been reported in recent single case studies. (Couto, Sedeno et al. 2012, p.5).
Due single cases are reported, p< .05 values of a tail were considered statistically significant in all comparisons (not taking into account trends as a significant difference). Results are presented from a simple analysis (no covariates).
Results
The sociodemographic, clinical, and neuro-psychological characterization of the case study participants (vmPFC & control) is described in table 1. All participants were male.
Table 1 Sociodemographic Data and Neuropsychological Evaluation
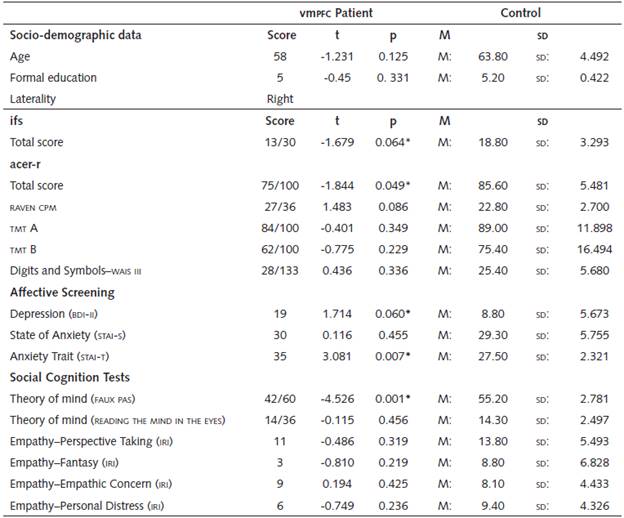
Notes: The values are expressed in means (M) and standard deviation (SD). * Significance level < .05
There were no significant differences in age (t = -1.231, p = .13) and years of formal education (t = -.45, p = .33) between the vmPFC patient and the control sample.
Neuropsychological Assessment
A statistically significant difference was found in the total Ineco Frontal Screening (IFS) score and a trend towards underperformance by the control group in terms of executive functions (t =-1.679, p = 0.064). The patient obtained a low and/or failed score in the subtests: Inhibitory Control (Go-No Go) in which he could not follow the instruction. Verbal working memory where he did not complete the task of saying the months of the year in reverse order. Proverbs where he only gave a correct explanation and Hayling test in the Inhibition stage where he only answered one option correctly. The other tasks were within the average compared to the reference group.
Likewise, in the overall cognitive functions measured on the Addenbr'oke's Cognitive Examination-Revised (ACER-COI), the vmPFC patient performed significantly less than the control group (t = -1.844, p = .049) in terms of the total score. The comparative performances for each subtest are divided in Table 2 below.
Table 2 ACER-R Detailed Score
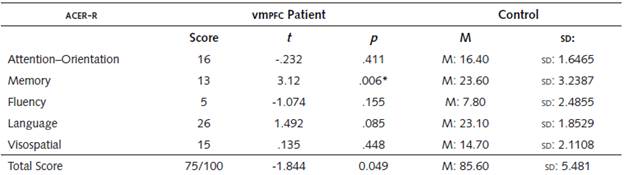
Notes: The values are expressed in means (M) and standard deviation (SD). * Significance level < .05
In this cognitive screening, the vmPFC patient obtained a significantly lower score than the control group (t = -3.12, p = .006) in the retrograde memory and evocation tasks, where he was able to remember only one stimulus of the information provided. The other dimensions of cognitive functions: Attention and orientation, verbal fluency, language, and visuospatial and perceptual skills are preserved and in the normal range.
The intelligence tasks represented in the Raven CPM Matrix test, did not show differences and are within the parameters of the group (t = 1.483, p = .086). In the WAis ill-Digits and Symbols subtest, the patient performed slightly better than the group in the direct score 28 vmPFc/25 controls. (t = .436, p = .336).
The cognitive flexibility tests measured with the Trail Making Test (TMT) part A and B, did not allow establishing significant performance differences below the reference group TMT-A (t = -.401, p = .35), TMT-B (t = -.775, p = .23).
Affective Screening
There were significant differences in the depression tests measured with the Beck Depression Inventory (BDI-II) for the patient in contrast to the control group (t = 1.714, p = .060). Anxiety as a state, measured with the Strate Trait Anxiety Inventory (STAI-S) did not show significant differences ( t = .1160, p = .455), however, anxiety measured as a trait with the Strate Trait Anxiety Inventory (STAI-T) allowed a difference to be observed between the vmPFC patient and the control group (t = 3.081, p = .007).
Evaluation of the components of Social Cognition (SC)
Table 3 Comparison Between the vmPFC Patient and the Control Group in CS
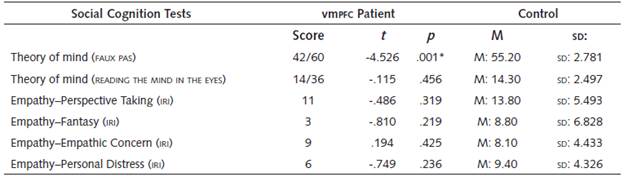
Notes: The values are expressed in means (M) and standard deviation (SD). * Significance level < .05
The Theory of the Mind measured with the Faux Pas Test, allowed to evidence a significant difference in the patient's performance (t = -4.526, p = .001). The other test applied for TOM: Reading Mind in the Eyes Test reported no difference (t = -.115, p = .456).
Finally, the Interpersonal Reactivity Index (IRI) measures cognitive and affective empathy processes in four subscales: Perspective Taking (PT) (t = -.486, p = .319), Fantasy (FS) (t = -.810, p = .219), Empathic Concern (EC) (t = .194, p = .425), and Personal Discomfort (PD) (t = -.749, p = .236), reported no significant performance differences.
Discussion
The usual neuropsychological approach in patients with stroke sequelae usually aims to assess cognitive functions as memory, attention, language domains, praxis, and mathematical knowledge (Njomboro, 2017). However, the impact of the disease on the domains of CS is, in most cases, overlooked. Hence the interest in identifying socio-cognitive changes associated with stroke in the vmPFC region.
The two groups (vmPFC patient and healthy controls) did not differ in age, education, laterality or estimated overall level of intellectual functioning, indicating that none of these demographic variables contributed to the extent of the deficits found.
Social Cognition Disorders
The Faux Pas Test (FPT) was where the patient performed the worst in relation to healthy controls. An important aspect of CS is TOM, a complex skill that seems to be influenced by EFS and emotion recognition (Baez et al., 2014).
FPT is a complex task, as it measures the person's ability to simultaneously understand the beliefs of two characters (Stone et al., 1998; Gregory et al., 2002). Therefore, this test implies a greater demand for EF. Ibáñez et al., (2017) report that the evidence suggests an association between TOM functions and EF in which EF performance should be considered when interpreting task performance.
In our study there are relatively intact intellectual skills (Shamay-Tsoory et al., 2005), so we assumed performance on the FPT as a reliable indicator of the TOM deficit. Studies using misstep recognition tasks as FPT have demonstrated a reliable deficit in vmPFC patients to correctly identify shame in others (Shamay-Tsoory et al., 2005; Stone et al., 1998).
In addition, Schneider & Koenigs (2017) found that vmPFC patients perform poorly on evidence of someone's second-order false beliefs based on another person's thoughts (Shamay-Tsoory et al., 2009, 2006, 2005; Shamay-Tsoory, and Aharon-Peretz, 2007; Stuss et al., 2001). This was consistent with what was found in the study.
In the Reading Mind in the Eyes Test (RMET), no differences were evident in the two groups. This is not unexpected since the RMET is a measure of mental state discrimination that is the first stage of attribution of TOM (Ibáñez et al., 2017).
In a study of TOM, its relationship to EFS and emotion recognition in borderline personality disorder (BPD), Baez et al., (2014) reported that their patients showed deficits in FPT scores but did not evidence low performance in RMET scores, this TOM study is consistent in this respect with the results of our case study.
With regard to laterality, emotional empathy studies have reported affective TOM deficits lateralized in right vmPFC (Shamay-Tsoory et al., 2003, 2005), while a false step recognition (FPT) study reported deficits for affective TOM in a left vmPFC lesion (Leopold et al., 2012). Consequently, we could state that the findings in our study are more consistent with those reported by Shamay-Tsoory et al., (2003) than with the study by Leopold et al (2012). This may be due to the limitation of sample size, in our case, because it was a study with one (1) patient and in that of Shamay-Tsoory et al. (2005) with 8. Further research is required to clarify the role of the lateralization of different domains of vmPFC function and their relationship to affective TOM.
Stuss et al., (2001) have suggested that the right frontal lobe, rather than the left, has an important role in detecting deception, a classic instance of TOM. TOM skills are usually divided into cognitive (beliefs and intentions of others) and affective (emotional states of others) components Ibáñez et al. (2017). It should be reiterated that the patient's injury is right.
Young et al., (2010) conclude that patients with vmPFC injuries make abnormal judgments in response to moral dilemmas and that these patients are especially affected in emotional responses triggering inferred or abstract-events -intentions- as opposed to real events.
Consequently, it is inferred that there may be presence of alterations in the affective TOM in terms of the capacity to correctly and completely perceive and interpret the impact on the social failure of "another" as well as to attribute intentions and affective representations derived from the context -specifically in the decoding of irony or sarcasm-. The latter was evidenced in the understanding and explanation of IFS sayings where the patient was underperforming. Conventionally, lesions in vmPFC have been associated with impaired affective TOM (Rowe et al., 2001; Dvash & Shamay-Tsoory, 2014).
Schneider & Koenigs (2017) support this inference with their conclusions when they state that deficits following a vmPFC injury "may be particularly pronounced for TOM tasks involving affective information. For example, while vmPFC patients exhibit normal performance in second-order false belief tasks involving emotionally neutral events, vmPFC patients perform poorly on such tasks involving affective information (i.e., understanding what someone thinks about how someone else feels) (Shamaysoory et al., 2006, 2005; Shamay-Tsoory and Aharon-Peretz, 2007)" (p.88).
In addition, in a battery of TOM tasks including emotional and non-emotional tests of irony identification, sarcasm, false attribution, lie understanding, and false belief tasks, vmPFC patients scored worse than other front-end patients only on the emotional items, showing intact performance on the non-emotional items in each task (Shamay-Tsoory et al., 2006).
Winner (1998), refers that irony is a common feature of everyday speech that is used to convey feelings indirectly. It is characterized by the opposition between the literal meaning of the sentence and the speaker's meaning and is supposed to imply the ability to create a meta-representation. Sarcasm is a form of ironic discourse used to convey implicit criticism and negative feelings. To detect sarcasm and irony, the listener must first make inferences about what the speaker knows and then infer the speaker's intentions (McDonald, 2010).
Understanding ironic expressions is not only based on the ability to understand false second-order beliefs, but also requires emotional processing, since the subject must also identify the affect transmitted indirectly. Shamay et al., (2002) showed that poor performance in this type oftask correlates significantly with empathic ability in patients with prefrontal cortex damage (PFC).
This supports the idea that the vmPFC patient is significantly impacted by the recognition of irony-squandering, social failure, or the presence of behavioral errors in a social context that demands to infer and attribute intentions and consequences. In other words, it is confirmed that the generation of affective states that inform the person in advance about the possible consequences of an action with an uncertain outcome (somatic marker hypothesis by Damasio, Tranel, & Damasio, 1990) is compromised in the patient. Furthermore, Schneider & Koenigs (2017) support this assertion, indicating that the somatic marker hypothesis does not address two critical sequelae of vmPFC damage.
In the first instance, patients with vmPFC injury exhibit deficits in a number of tasks that do not involve value-based choice or affective response, as confabulation and recall/recognition tasks. Second, in addition to exhibiting diminished levels of certain emotional responses (guilt, empathy, shame) vmPFC patients also exhibit exaggerated levels of anger, frustration, and irritability. The latter is analogous to what was reported by the BDI-II in this case study. Injuries in right vmPFC are associated with a more pronounced TOM deficit (Shamay-Tsoory et al., 2005). This finding is part of the altered impact on the patient's relational functions.
One aspect found contradictory to previous literature, is that while the patient has impacted his emotional TOM; his cognitive and affective empathy seems to be relatively intact. This contrasts with the evidence referred by Shamay-Tsoory et al., (2009) when they indicate that injury studies suggest that people with vmPFC damage are specifically affected in both cognitive and affective TOM implying a direct involvement in cognitive empathy. In our case, this is not consistent. The results of our study showed no significant differences in cognitive TOM, nor in the four empathy subscales of the IRI: Cognitive (PT) (t = -.486, p = .319), (FS) (t = -.810, p = .219), Affective (EC) (t = .194, p = .425), and (PD) (t = -.749, p = .236). It seems then that the deficiency of the patient is particularly evidenced in integrating empathy with the attribution of the mental state. This is consistent with what Baron-Cohen (1991) reported when he found in his studies of autism that people could understand the emotions of others if those emotions were caused by situations or desires. However, they did not understand emotions caused by belief.
The affective TOM limits with the concept of empathy, while the emphasis in the TOM is in the knowledge of the affective state of the other, the empathy is associated mainly with the "feeling" of the experiences of the other (Ibáñez, Sedeno, & Garcia, 2017). The study confirmed the deterioration in the affective TOM after an ABI in vmPFC, and allows to appreciate that the capacity to infer the thoughts and feelings of the others is critical for the appropriate, effective social interactions and the understanding of the speech, but it is not enough. Understanding belief does not guarantee understanding emotion; understanding emotion does not guarantee empathy; and empathy does not guarantee sympathy manifested by kindness to people (Davis and Stone, 2003).
Stone et al. (1998) concluded in their study of bilateral OFC patients that this region is part of the TOM circuit, perhaps particularly involved in affective TOM tasks. In our study, given the similarities in performance with the work of Stone et al. (1998), clinical evidence and functional neuroimaging could be associated and also conclude that vmPFC is linked to the affective component of TOM, as the results of Leopold et al, (2012) support the theory that vmPFC is associated with affective TOM skills. In conclusion, this study confirms and extends what has been reported in the previous literature.
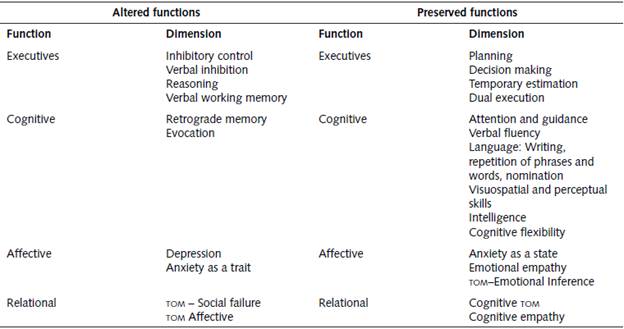
Committed functions
The sequelae of right ischemic stroke in vmPFC show a deficit in motor and verbal inhibitory control in the patient. There was also a slight impact on reasoning. These results are consistent with the literature (Shamay-Tsoory et al., 2005; Shamay-Tsoory et al., 2009). In addition, previous studies indicate that patients with vmPFC lesions develop significant impairment or deficits in a number of interrelated functions: value-based decision making, future and counterfactual thinking, physiological arousal to emotional stimuli, emotion recognition, empathy, moral judgment, and memory conspiracy (Schneider & Koenigs, 2017). However, intellectual abilities have been observed to be intact, and in addition, symptoms are not evident on traditional intelligence tests or standard neuropsychological measures (Shamay-Tsoory et al., 2005). This is consistent with the findings of this case study, where the patient shows relatively mild alterations in the EF.
Compared to the EF, there was a significant impact on verbal working memory. Injuries in vmPFC have an impact on the memory process (Petrides, 2005 cited by Contreras et al., 2008). Indeed, the patient evaluated presented and verbalized difficulties in tasks involving the use of verbal working memory and retrograde memory. Likewise, he presented difficulties in the evocation of information.
Petrides (2005) indicates that vmPFC innervates all other areas of the prefrontal cortex, that are attributed a fundamental role in EF and working memory. Schneider & Koenigs (2017) found that conspiratorial patients (who recover false information in their memory without conscious intent to deceive) with vmPFC injuries, make more errors or false positives in a memory recognition task, suggesting that vmPFC is involved in suppressing irrelevant information in the memory (Schneider & Koenigs, 2017). This may be associated with the deficit of verbal inhibitory control presented by the patient, and is consistent with what has been reported. We see then how some EFS and cognitive of the patient were impacted and the consistency of what was found with what was previously reported in this type of lesions.
Depression and altered anxiety were also recorded in terms of the patient's affective functions. He showed a propensity for irritability that was consistent with BDI-II. Difficulty in concentration, sensation of fatigue, and loss of interest in sex were also observed. The latter is consistent with Dimitrov, Phipps, Zahn & Grafman (1999) when they report that vmPFC injuries produce a set of symptoms that include: mood alterations, significant decrease in social competence, and deterioration of sexual behavior.
Similarly, the patient reported a slight increase in feelings of sadness, guilt, and worthlessness, which is somewhat contradictory to Koenigs et al. (2008), who preliminarily concluded that the results of the study of vmPFC injuries in a group of Vietnam War veterans could explain the reduced expression of emotion and therefore infer a lower likelihood of developing mood and anxiety disorders after vmPFC damage. In their study, this was evidenced by "somatic" symptoms of depression with normal levels of fatigue, appetite changes and sleep disturbances (similar results in our evaluated patient) but significantly decreased levels of "cognitive/affective" symptoms as feelings of sadness, guilt, and worthlessness (results with slight discrepancies in our evaluated patient).
Preserved functions
On the other hand, the impact of the patient's right ischemic stroke has not made a significant dent in the EFS as: Planning, decision making, time estimation, dual execution. Likewise, basic cognitive functions as attention and orientation, verbal fluency, language (writing, repetition of sentences and words, nomination) are preserved.
The visuospatial and perceptual skills, intelligence, and cognitive flexibility account for a minor or almost imperceptible impact, in fact the patient drives a motorcycle and makes his economic livelihood from transporting passengers in that vehicle. In this sense, the great majority of executive and cognitive functioning is stable, preserved and operating (Shamay-Tsoory et al., 2005).
In relation to affective functions, it was found that anxiety as a state is within the expected parameters compared to healthy people. Similarly, cognitive empathy and affective empathy are within the average. Finally, with regard to the patient's relational functions, it was found that TOM in its cognitive part, does not present significant alterations. This incompatibility with the previous study by Shamay-Tsoory et al., (2009) was already presented in the previous section.
It is important to highlight here that the patient did not develop, or there is not enough evidence to indicate that he has the well-known "acquired sociopathy" (Eslinger and Damasio, 1985), since although he presents some symptoms as apathy, impulsiveness, and irritability (registered in BDI-II and IFS, and by express manifestation of the patient and his or her companion) there were no indicators or references of uninhibited behavior, accentuated irresponsibility, "shameless" social behavior, or a significant change in personality (Blumer & Benson, 1975 cited by Schneider & Koenigs, 2017).
The answer to the question of why these areas are conserved has to do with the circumscribed location of the lesion in vmPFC, the anatomical dissociation between aspects of empathy (Shamay-Tsoory et al., 2009), and the role that this area has in the affective processes of cs. This finding also confirms and extends the previous findings regarding empirical evidence on brain plasticity and neural bases.
The neuropsychological profile found is similar to that reported in the previous literature in patients with lesions reported in vmPFC, OFC and PCF (Damasio, Tranel & Damasio, 1990; Baron Cohen, 1991; Dimitrov, Phipps, Zahn & Grafman, 1999; Shamay SG. Et al., 2002; Petrides, 2005; Shamay-Tsoory et al., 2009; Leopold et al., 2012; Dvash & Shamay-Tsoory, 2014; Ibáñez, Huepe, et al., 2013; Ibáñez et al., 2017).
Consistent with this, the present study found discrepancies with some previous research (Koenigs et al., 2008; Shamay-Tsoory et al., 2009; Leopold et al., 2012) but did not find anything new in relation to the reported scientific literature.
Limitations
Reduced number of participants as it was a case study, therefore, although the findings confirm the previous literature and suggest implications at the clinical and theoretical levels, the scope of the present study is limited and not generalizable.
The patient showed some anxiety and emotional dysregulation, although as we saw, this also occurred in the study by Shamay-Tsoory et al., (2005), with no direct inferences or correlations reported between the patient's state ofanxiety/depression and final task performance, particularly in the FPT.
No standardized tests were used to measure emotion recognition. No cognitive and/or experimental tasks were used and no tasks were used to measure irony and sarcasm. This would have allowed for richer conclusions and more telling findings.
Conclusions
The need to carry out longitudinal studies is highlighted, because most of the previous literature reports cross-sectional studies, which in their design do not facilitate the monitoring and a long-term approach to the phenomenon. This would allow monitoring changes and offer more evidence and greater understanding of the evolution of the impact of the injury.
It is also important to do more focused research on the findings of this study. In aspects related to the deterioration of affective TOM and how this element is impacted after a vmPFC injury. A framework or protocol for assessing and intervening in aspects of TOM that would involve documenting strengths and deficits in TOM: interpersonal and intrapersonal cognitive and affective TOM and affective empathy. Further research approaches are required to clarify the picture against the lateralization of different domains of function in vmPFC and their relationship to affective TOM.

