











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Cultural diversity implies that health professionals, including nurses, face the challenge of offering coherent, effective, and efficient responses to the need for cultural or intercultural care 1,2. This situation requires a greater commitment on the part of Public Health Nurses (PHN), since their functions are related to acting as a bridge between cultural practices and health systems, being responsible for considering cultural differences for the adaptation of care and developing public policies that tend to defend ethnic and racial minorities.
In relation to this, cultural competence for nursing is conceived as an orientation that aims to improve the results of the care provided in intercultural contexts 3-5. It is recognized that nursing has made valuable contributions to the evolution of cultural competence by focusing on the development of instruments that make the measurement of the level of nurses in this area 6,7 possible, and on the recognition of the barriers that are set up when people from different cultures are cared for, e.g., minority groups 8,9.
In recent years, important results that inform about the relationship of the nursing professional with the indigenous population 3,9-11 have also been obtained, which is highly relevant for cultural competence since this population group is characterized by a cultural situation different from that of the general population 12-14.
In the information obtained on nursing care for the indigenous population, the still incipient area of the professional’s feelings corresponds to an element of vital importance to understand the dynamics and experiences of professionals in environments where the population assisted is culturally different from that of the professional. These results can be used to improve direct care, health services, care, and institutional dynamics 15. Therefore, the objective of this study was to interpret the perception of the public health nurses when they provide the indigenous Embera Chami community with culturally competent care.
Methods and Materials
Interpretive ethnography 16, intentional sampling, participation of three mestizo PHN, which correspond to the total number of professionals who carry out care actions in an Institution Providing Health Services (IPS) according to intercultural guidelines exclusively for indigenous people. The inclusion criteria were: (1) Colombian nationality and (2) past or present care actions regarding controls of outgrowth and development, arterial hypertension, and family planning to the Embera Chami indigenous people in the department of Caldas in the last 6 months.
The field work, which began in 2015 and ended in 2017, was characterized by participant observation and ethnographic interviews with PHN, and allowed to obtain more than 30 field diaries, approximately 480 minutes of verbatim transcribed recording and the selection of 40 ethnographic photos. These documents were analyzed with the help of the Atlas ti software and guided by Leininger’s proposal 5, a spiral scheme was followed. Furthermore, the six criteria proposed by the same author related to the guidelines were used to demonstrate validity and reliability in qualitative research. Categories and subcategories were generated by regrouping and renaming them through constant reflection with an expert ethnographer and members of the research group. At the end, the results were shared with the collaborators as part of the methodological rigor and suggestions for language precision were made.
The ethical endorsement of the National University of Colombia and the permission of the indigenous leaders, the municipality’s department of health, the intercultural IPS and the PHN were obtained, which is verified with the signing of the informed consent. A pseudonym was used for all collaborators and the data was kept confidential.
Results
The perception of the PHN when they provide culturally competent care to the Embera Chami indigenous people was interpreted in the category called “As a nurse I am happy with intercultural work, creating bonds of affection with the Embera.” This category is made up of three subcategories that reveal the feelings of the PHN regarding various aspects of their daily life, both at work within an intercultural IPS in which they only serve Embera individuals, and in the experiences in a municipality in which these indigenous people prevail. In these situations, an affective bond is generated between the nurse and the Embera Chami indigenous people. Each of the subcategories is specified below.
Subcategory 1: As a nurse I am happy in the municipality, in the intercultural IPS and with the traditional doctor
The PHN, for work and family reasons, decides to live in the municipality of the Embera Chami indigenous people. This municipality has a population of approximately 63,000 inhabitants, its rural area consists of four reservations: “Nuestra Señora Candelaria de la Montaña”, Cañamomo Lomaprieta, Escopetera Pirza and San Lorenzo, which have geographic and climatic variety. The urban area, where the nurses live, has a climate between 16 and 22 degrees Celsius, it has traditionally been a “coffee town”, and provides PHN security, tranquility, and lower costs of living compared to capital cities. In addition, it offers professionals the possibility of studying at the postgraduate level, since geographically they have access to four capital cities, the most distant of which is 150 km away.
“I am surprised by the characteristics of the town, much larger and more modern than I imagined. Paved streets, brick houses, 3 Catholic churches, a hospital, two parks, a police station, the city hall, it has a lot of commerce” (Participant Observation, 17-21: 2).
Another pleasant situation for the PHN, who lives in the municipality, is the fact of sharing daily life with the indigenous Embera Chami. The experience of daily encounters allows the professionals to identify that, in general, the Embera are characterized by being simple, kind, and gentle people. In relation to this, nurses feel accepted, valued, supported, and loved by most people in the community.
“[Referring to the Embera]. If they make me feel very good, then I am not capable of making the community look bad” (Nurse SV, 28-152: 52).
For the PHN, the form of institutional organization of the IPS where they work brings them financial, spiritual, and personal benefits. In relation to economic benefits, they have an indefinite term contract that includes all the benefits granted by the country’s Law and their payment is received in a timely manner.
The intercultural guidelines of the IPS allow PHN to experience the typical dynamics of the Embera Chami indigenous culture. One of the most enjoyable activities for nurses is the rituals and harmonization that the institution performs for its employees. These rituals, in addition to promoting a change of thought in the health-disease processes in the professionals, involve them in an accepted and respected syncretism, to the point that they find their own benefits aimed at tranquility and serenity (figure 1: participant observations, 56: 37).
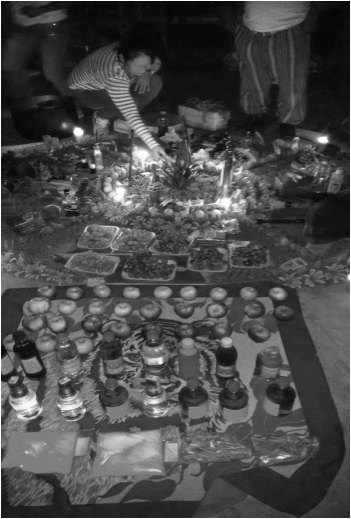
Source: Liliana Orozco (author, 56: 37)
Figure 1 Ritual organized by the indigenous IPS for its officials. San Lorenzo Resguardo, Riosucio, Caldas.
The relationship of the PHN with the indigenous person within the institution - be it a patient, coworker, boss, traditional doctor, or midwife - produces personal and professional well-being since they feel happy with the work done because they adjust to the studies and the competencies learned at the university. Likewise, the coordination within the IPS is homogeneously distributed and the goals set are possible to achieve.
“Having learned from traditional doctors, from the community, that I can cure a patient and then put a plaster made of a plant because the traditional doctor recommended it and see that the patient is perfect after two days, is very satisfying” (Nurse SV 21-72: 132).
In this subcategory, PHN experience a positive and satisfactory feeling and professional and personal development when they carry out their care directed and integrated with the municipal and institutional systems and policies of an intercultural nature. Therefore, they interact, work, provide care and live in greater harmony with people of a culture different from their own, in this case the Embera Chami indigenous people.
Subcategory 2: As a nurse, I create bonds of affection with the Embera in various settings
Living close to the indigenous people slowly makes the nurses begin to enjoy a series of typical activities of the indigenous daily life. Thus, the professionals participate in social activities of the Embera, either for their own pleasure, to understand the organization of the indigenous people, or out of full responsibility.
“I sit on the field to watch a football game, everyone greets me: « Hello boss! Who is going to win? », I do not know, they take me into account, so I arrive as if I were at home” (Nurse SV, 13-72: 79).
Coexistence with the Embera Chami also allows PHN to learn about their history, characteristics, political organization, developments, tastes, life situations, and customs. Thus, each nurse, in the manifestation of affection, adapts the care to the needs of the indigenous people.
“At 11 am, an indigenous person, who had the control scheduled at 8:00 am, arrives and he says he forgot, and the nurse decides to assist him” (Participant Observation, 15-49: 20).
The nurses also have contact with indigenous professionals who work in the health area. These indigenous people are recognized by the nurses as leaders and work with them jointly, such dynamics make their interaction increase. The indigenous leaders and the nurses have periodic meetings and conversations to discuss issues in favor of the welfare of the indigenous community.
For public health nurses, the situation of meeting and integrating with the indigenous Embera Chami in the work, social, cultural, and personal sphere, specifically, being close to them and providing care has brought satisfaction. This bond generates ties of affection with the indigenous people, who return that familiarity by seeking greater closeness with the nurses.
“They are very lovable [referring to the indigenous]. If you show yourself as an ordinary person, you can reach out, they can talk to you, you become a friend, you become family. I’m telling you, they fight to invite me to lunch, to be with me, they sit with me” (Nurse SV, 13-72: 78).
Subcategory 3 I recognize the importance of the Embera language, and I join the efforts to recover it
The PHN are involved in the process of recovering the Embera language in conjunction with some indigenous people from the municipality. At present, this cultural characteristic is considered lost, since only some indigenous leaders use it in very specific contexts, such as rituals.
The Caponias (the name given by the indigenous to the mestizos) and the indigenous (especially the leaders) place the Embera language as a fundamental element for the strengthening of the indigenous identity, which they have the firm desire to preserve. To achieve this objective, they sometimes use some posters with information in the Embera language and with a translation into Spanish, which is the predominant language. Additionally, students from public schools and colleges receive Embera language classes with teachers from other regions such as Antioquia, who teach them basic words related to greetings, colors, relationships, and the alphabet, among others (figure 2: participant observations, 24:28).
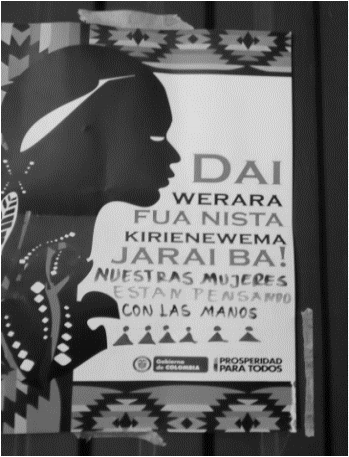
Source: Liliana Orozco (author, 24:28)
Figure 2 Poster located in the House of Culture. San Lorenzo Resguardo, Riosucio, Caldas.
Another setting for teaching the Embera language and where PHN participate is in the intercultural IPS. This institution teaches Embera classes to all employees. The nurses, mostly mestizo and whose native language is Spanish, attend Embera classes, and learn some words and phrases with difficulty. Despite not being necessary for everyday life, or to carry out controls, since all the Embera Chami indigenous people in the municipality speak Spanish, they do so out of pleasure and interest in learning the language.
“In general, none of the reservations have Embera speakers, but we are learning. They are teaching all IPS employees on Saturdays” (Participant observation, 24-51: 22).
Discussion
As there is little research development on the feelings of PHN when they provide care for the indigenous population, the results obtained become a base element to understand the Consciousness and Cultural Ability constructs proposed by Bacote 17 and, thus, formulate proposals that improve the cultural competence with this population group. In the results, a positive, satisfactory, and professional and personal development feeling of the PHN is perceived when they provide care directed and integrated with the municipal and institutional systems and policies of an intercultural nature. These actions allow PHN to interact, work, provide care and live-in greater harmony with people from a culture other than their own, in this case, that of the indigenous Embera Chami. These findings differ from the ones of the review of experiences of hospital nurses about compassion and care for culturally diverse people, which showed evident tensions between personal, professional, and institutional culture 18.
The positive feelings of the nurses indicate the strengthening of this element since the results make a new contribution opposed to the difficulties of health professionals, including nurses, when they provide care for patients from cultures different from their own and there is no direct support from the health institution in terms of elements, tools, and training. Berlin 19 support and help. A majority (84% and Whitman & Davis 20 support and help. A majority (84% demonstrate how the lack of institutional support is associated with difficulties in interacting with patients and dissatisfaction with the work done by professionals. In contrast, the experience of working in an institution with intercultural guidelines produces satisfaction in nurses and good relationships with the patient they care for, which is expressed as a necessary idea in the materialization of cultural competence.
In recent years, some researchers have warned about the importance of knowing the perception of the care recipient to fully understand the phenomenon of cultural competence 7,21-23 which motivated this research to also focus on knowing the perception of indigenous people regarding the care received, and defined the object of a different cultural article 23. In particular, the results of this research show the importance of the nurses’ perception of their work and the care offered, as it constitutes a fundamental part and factor of the act of care, which makes personal and professional feelings an element of the phenomenon of cultural competence.
The results also propose that the PHN generate other encounters with the indigenous Embera Chami, different from the act of care. These experiences in the daily life of the indigenous confirm the construct of cultural encounters proposed by Bacote 17 defined as the process of participating directly in cultural interactions with the client. In the latest version of his theory, Bacote 4 states that without such approaches, nurses could not develop cultural competence. Based on these characteristics, in this study, the PHN have fostered cultural encounters that emerged from their personal and work daily life, which strengthens their cultural competence.
There are barriers in nursing care to the indigenous population 3,11,24 however, the ability of nurses to interact with care recipients and with colleagues was constituted as an element of cultural competence in another study 25. Such fact coincides with the results of this research, in which the cultural competence of nurses is not limited to direct care spaces, but also extends to other contexts shared with the indigenous people they serve, the common indigenous people that share their daily lives, the indigenous co-worker and the indigenous community leader.
In relation to these cultural encounters, it is inferred that the cultural competence of the PHN when they take care of the Embera Chami population is nourished by moments of care and extends to everyday encounters derived from living and socializing with the indigenous population. Thus, the cultural knowledge of the PHN is potentiated, which allows them to develop their own concept of the Embera and, based on this, to carry out closer and more coherent care according to the customs and beliefs of these indigenous people.
The qualitative phase of Hagman’s study 26 determined that education was one of the most frequent methods to achieve the level of cultural self-efficacy. In this study, the fact that education in cultural competence can be acquired in different ways is affirmed. Job training, work experience, and life experience, through resources such as asking questions, listening to people, and collaborating with colleagues or other ethnic groups 26 are part of that education. What Hagman found supports the results of this study, in which there are different learning spaces that manage to establish close social relationships with the people of the ethnic group served, which has repercussions on the development of cultural competence.
On the other hand, the importance of assessing the linguistic needs of individuals appears as a characteristic that determines the recipient of care and, therefore, it is conceived as the basis for culturally competent care 4,12,27. Research shows how adaptation to a common language is one of the most relevant dimensions for the development of cultural competence 5,26,28, which in this particular case occurs between professionals and patients who speak the same language as a historical consequence of the colonization of Western culture in indigenous territories. The Embera have gradually lost their native language, therefore, they adopted the same language of the nurses (Spanish), which has eliminated a barrier to culturally competent care. However, in this case, the nurses are linked to the learning of the ancestral language of the community; it is not a need for them, but it could be for the indigenous people. For this reason, the cultural competence of the PHN in relation to this population goes beyond the limits of the act of care since they seek to relate to the essential elements that give identity to the indigenous culture.
A limitation of this research is the exclusivity of its development in an IPS with intercultural guidelines exclusively for indigenous people, which is why it is necessary to carry out other studies on the perceptions of PHN when caring for indigenous people in institutions with different foundations.
Conclusions
The data obtained allow us to interpret, as a result, the positive feeling that the PHN have regarding the care provided, which is manifested in the well-being, enjoyment, and personal and professional satisfaction when involved in the indigenous people context. This allows them to live and have work and personal experiences in daily life, which change the perspective and beliefs of life, thus, improving interventions and care provided for the indigenous people.
The importance of sharing everyday life and getting involved in the cultural system of the other as an essential component of cultural competence becomes evident, since this allows greater syncretism between care and generates satisfaction for those who provide care.
We are thankful to the participants and collaborators of the research. To the University of Caldas.

