










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Colombiana de Reumatología
versión impresa ISSN 0121-8123
Rev.Colomb.Reumatol. vol.21 no.1 Bogotá ene./mar. 2014
Case Report
bMédico Internista, Reumatólogo, Pontificia Universidad Javeriana, Hospital Universitario San Ignacio, Grupo Javeriano de Investigación en Enfermedades Reumáticas, Bogotá, Colombia
cMédico cirujano, Pontificia Universidad Javeriana, Bogotá, Colombia
dMédico Internista, Reumatólogo, Hospital Universitario Clínica San Rafael, Bogotá, Colombia
* Corresponding author.
E-mail address: danielfernandezmd@gmail.com (D.G. Fernández-Avila).
Article history:
Received November 19, 2013 Accepted April 1, 2014
Abstract
We report the case of a 70-year-old male with chronic abdominal pain, who presented with increased intensity of the pain, and was initially diagnosed and treated for acute biliary pancreatitis. However, the symptoms persisted after hospital discharge, and he was subsequently studied with cholangio-MRI, abdominal CT scan, and ERCP, which revealed dilation of the biliary tract and a mass in the head of the pancreas. An excisional biopsy of the lesion showed chronic inflammation with severe sclerosing fibrosis and a lymphoplasmacytic infiltrate. A diagnosis of autoimmune pancreatitis was made, and the patient was initiated on azathioprine with good clinical response.
Keywords: Abdominal pain, Autoimmune pancreatitis, Cholelithiasis, Abdominal mass.
Resumen
Presentamos el caso de un varón de 70 años con dolor abdominal crónico, que se presenta con aumento de este; se le diagnostica y se lo trata inicialmente como cuadro de pancreatitis biliar. A pesar del manejo inicial, los síntomas persisten después de la primera hospitalización, y se estudia con tomografía computarizada de abdomen, colangiorresonancia y colangiopancreatografía retrograda endoscópica, estudios en los cuales se detecta dilatación de la vía biliar y masa en la cabeza del páncreas. Se llevó a cabo biopsia excisional, que demuestra inflamación crónica con intensa fibrosis e infiltrado linfocitario. Se hace diagnóstico de pancreatitis autoimmunitaria y se inicia azatioprina, con adecuada respuesta.
Palabras clave: Dolor abdominal, Pancreatitis autoinmunitaria, Colelitiasis, Masa abdominal.
Introduction
Autoimmune pancreatitis is a rare disease that presents with clinical, serologic, and histologic characteristics of a defined autoimmune process that usually responds to the use of steroids.1 Yoshida introduced the term in 1995, replacing others that did not properly define the disease such as primary chronic pancreatitis, sclerosing chronic pancreatitis, duct destructive chronic pancreatitis, and sclerosing lymphoplasmacytic pancreatitis.2-6
Most information comes from Japan, where the number of documented cases has increased, probably due to improvements in diagnostic techniques and greater awareness of the disease. Cases have been reported in Europe, USA, and South Korea, which suggest that autoimmune pancreatitis has a worldwide prevalence. This disease may present as an isolated primary entity or it can be associated to other autoimmune diseases such as primary sclerosing cholangitis, primary biliary cirrhosis, retroperitoneal fibrosis, rheumatoid arthritis, sarcoidosis and Sjögren's syndrome.7,8
Case report
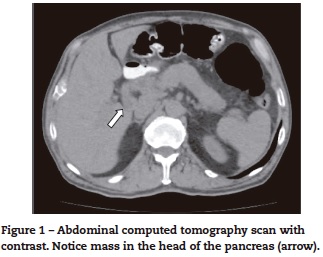
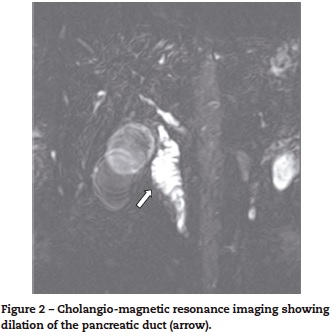
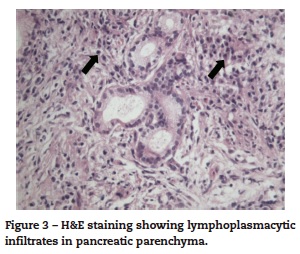
We report the case of a 70-year-old male with a 10 month history of upper abdominal pain, jaundice, dark urine, pale stools, night sweats, generalized pruritus and weight loss of 28kg and no history of autoimmune disease. An initial diagnosis of biliary pancreatitis was made, and an endoscopic retrograde cholangiopancreatography (ERCP) was attempted, without success. Labs showed normal transaminase levels, direct hyperbilirubinemia, and elevated levels of alkaline phosphatase (972 UI/L), amylase (174 U/L) and lipase (1314 U/L). Hepatobiliary ultrasound showed a distended gallbladder with thickened walls, dilated intra and extra-hepatic ducts, a 17 mm dilation of the common bile duct, and a distal image that suggested biliary sludge associated with a diffuse growth of the pancreas. A new ERCP was attempted without success so a computed tomography (CT) scan was performed. The scan showed dilation of the biliary tree and a mass in the head of the pancreas (figure 1). The main differential diagnoses that were initially considered were cholangiocarcinoma and pancreatitis (Balthazar B). Subsequently, a cholangio-magnetic resonance imaging (MRI) revealed an obstruction of the biliary duct at the level of the intra-pancreatic tract, which could correspond to a multi-focal cholangiocarcinoma (figure 2). The patient was finally taken to surgery for an exploratory laparotomy, and frozen section biopsy revealed a chronic inflammatory process. Further histological studies showed destruction of glandular architecture with severe sclerosing fibrosis and lymphoplasmacytic infiltrates (figure 3). The patient was started on azathioprine, with good response.
Discussion
Since autoimmune pancreatitis is a rare disease, its exact frequency is unknown. The prevalence has been estimated between 3.8 and 11% in patients with chronic pancreatitis, with a male-female ratio of 2.85.1,9,10. Most patients are diagnosed with the disease at age 55 or older, and up to 50% of them present with concomitant diabetes mellitus.9 In the United States, approximately 2.5% of the pancreaticoduodenectomies that were performed for masses that were diagnosed as cancer, and 23% of those that were done for suspected benign lesions, resulted in a histological diagnosis of autoimmune pancreatitis.11,12 This disease has been associated with other autoimmune diseases such as Sjögren's syndrome (12.2%), inflammatory bowel disease (7.6%), and retroperitoneal fibrosis (5.6%).13
Pathophysiological mechanisms described for autoimmune pancreatitis include both cellular and humoral immunity. Commonly, histological studies reveal lymphoplasmacytic infiltrates within the pancreatic lobules and ducts with a predominance of CD4+ and CD8+ lymphocytes.14 Patients with autoimmune pancreatitis may test positive for the following antibodies: anti-nuclear antibodies (ANAs), rheumatoid factor, lactoferrin, carbonic anhydrase II, and anti-smooth muscle antibody.14,15 These patients can also present with hypergammaglobulinemia and elevation of IgG, particularly IgG4, where even a systemic syndrome consisting of elevation of IgG4 and inflammation of the pancreas, salivary glands, biliary ducts and thyroid has been described.16-23 Finally, there also appears to be an association with DRB1*0405-DQB1*0401 HLA types.24
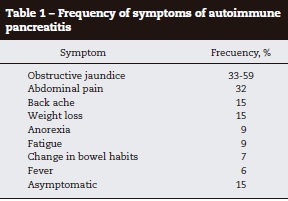
Clinical presentation may vary but there are two main patterns (table 1). Type 1 autoimmune pancreatitis presents in adults older than 60 years of age with obstructive jaundice and enlarged pancreas. The histological findings include lymphoplasmacytic infiltrate with elevation of IgG4. Type 2 autoimmune pancreatitis also presents with obstructive jaundice, but is associated to extensive destruction of the pancreatic ducts, usually presents in middle-aged patients, there is no elevation of IgG4, and is greatly associated with inflammatory bowel disease.25
Autoimmune pancreatitis presents with chronic abdominal pain accompanied by acute, chronic or recurrent pancreatitis.14 Up to 85% of patients present with a pancreatic mass that might be mistaken for carcinoma or lymphoma with stenosis pancreatic ducts.15-17 ;Up to 80% of patients may develop exocrine dysfunction of the pancreas, and almost 77% may have altered endocrine functions.26 The diagnosis of autoimmune pancreatitis should always be considered in patients that present with symptoms that suggest cholangitis or inflammation of the pancreas, especially when there is history of autoimmune disease or recurrent episodes of pancreatitis. Even though it is a rare disease, its opportune diagnosis and treatment limit the progression of the disease, and can reduce the need of surgery and further complications.19,20
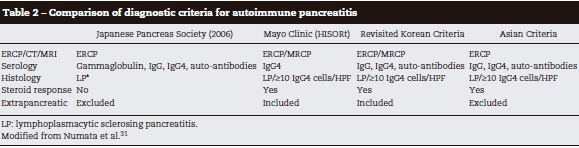
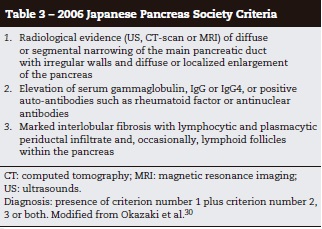
Different groups have proposed various diagnostic criteria for the disease (table 2).22,27-29 The most accepted are those established by the Japanese Pancreas Society (table 3).30
The main histological finding is lymphoplasmacytic sclerosing pancreatitis.32,33 The inflammation may compromise the peripancreatic fat, the pancreatic parenchyma and ducts, the veins (obstructive phlebitis), and the common bile duct.
Abdominal ultrasound normally reveals a “sausage shaped” diffuse enlargement of the pancreas with low echogenicity, and the common bile duct may appear dilated with thickened walls.34 CT scan usually shows an enlarged gland with parenchymal fibrosis and a capsule-like rim surrounding the lesions. This finding is very specific for autoimmune pancreatitis.23,27 MRI findings include diffuse enlargement of the pancreas with low signal in T1-weighted images and also a capsule-like rim in delayed-enhancement T2-weighted images.23,31 ERCP usually shows narrowing of the common bile duct and sometimes the intrahepatic ducts as well.19,22,35
Usually there is hypergammaglobulinemia (43%), elevation of serum IgG (62-80%), IgG4 (68-92%), ANAs (40-64%) and RF (25%).36 Other markers that may be found are: antibodies against carbonic anhydrase II (55%), lactoferrin (75%), and plasminogen binding protein (94%).36,37 The serologic marker with greater diagnostic value is IgG4, with an 80% sensitivity and a 98% specificity. Values 2 times greater than normal (140 mg/dL) are highly suggestive of autoimmune pancreatitis.19
Treatment decisions are based on data of observational studies. Expectant treatment has been considered, since some patients show spontaneous resolution of pancreatic oedema and narrowing of the pancreatic duct.38 Glucocorticoids are indicated in patients with obstructive jaundice, abdominal or back pain, and extra-pancreatic symptomatic lesions because this has been shown to prevent complications, and control symptoms in up to two thirds of patients.39-41 Rate of remission with steroid therapy has been described to be as high as 98% with an average remission time of 98 days.42 The recommended dose of prednisone is 0.6 mg/kg daily for 2 to 4 weeks, and then it should be decreased by 5 mg every 1 to 2 weeks depending on the clinical response of the patient, and on the serologic and radiologic evidence of improvement.43 The recommended maintenance dose ranges from 5-10 mg daily during the following 2-3 months after the initial schedule is completed.43-45 Suspension of medication after achieving remission has been associated to a greater rate of relapses.46 There is no consensus regarding the exact duration of treatment with steroids, but it is recommended that it should be continued for 3 years for patients that show serologic and radiologic improvement.41 Once the treatment is suspended, the patient needs to be monitored to detect relapses. If there is a relapse, the patient must be started on the same initial dose of prednisone as described above, but the subsequent doses have to be decreased at a more gradual rate.41
Immunomodulatory agents have also been used to control the disease. The most widely used has been azathioprine at a dose of 50 mg daily. Others, such as mycophenolate and cyclophosphamide, have also been administered to patients with refractory disease, but there are no clear indications for their use.15,18 There are two case-reports where rituximab was administered with improvement of symptoms in patients with autoimmune pancreatitis refractory to treatment with corticoids.47
Conclusions
Autoimmune pancreatitis is a rare disease that may present with systemic compromise and should be considered as a differential diagnosis of pancreatic tumours. Once there is a clinical suspicion, diagnosis should be made using current diagnostic criteria. When indicated, treatment with steroids must be initiated rapidly in order to improve symptoms and avoid relapses. There is a need for new studies that help determine the ideal duration of treatment as well as the accurate management of relapses and disease refractory to treatment with steroids.
Conflict of Interests
No conflict of interests reported.
References
1. Finkelberg DL, Sahani D, Deshpande V, Brugge WR. Autoimmune pancreatitis. N Engl J Med. 2006;355:2670-6. [ Links ]
2. Garber T, Farrell TJ. Autoimmune Pancreatitis: Time for a single nomenclature. Gastroenterology. 2004;126:255-9. [ Links ]
3. DiMagno EP. Autoimmune chronic pancreatitis: a plea for simplification and consistency. Clin Gastroenterol Hepatol. 2003;1:421-2. [ Links ]
4. Yoshida K, Toki F, Takeuchi T, Watanabe S, Shiratori K, Hayashi N. Chronic pancreatitis caused by an autoimmune abnormality. Proposal of the concept of autoimmune pancreatitis. Dig Dis Sci. 1995;40:1561-8. [ Links ]
5. Cavallini G. Is chronic pancreatitis a primary disease of the pancreatic ducts? A new pathogenetic hypothesis. Ital J Gastroenterol. 1993;25:391-6. [ Links ]
6. Ectors N, Maillet B, Aerts R, Geboes K, Donner A, Borchard F, et al. Non-alcoholic duct destructive chronic pancreatitis. Gut. 1997;41:263-8. [ Links ]
7. Kamisawa T, Egawa N, Nakajima H. Autoimmune pancreatitis is a systemic autoimmune disease. Am J Gastroenterol. 2003;98:2811-2. [ Links ]
8. Hirano K, Shiratori Y, Komatsu Y, Yamamoto N, Sasahira N, Toda N, et al. Involment of the biliary system in autoimmune pancreatitis: a follow-up study. Clin Gastroenterol Hepatol. 2003;1:453-64. [ Links ]
9. Pearson RK, Longnecker DS, Chari ST, Smyrk ST, Okazaki K, Frulloni L, et al. Controversies in clinical pancreatology: autoimmune pancreatitis: does it exist? Pancreas. 2003;27:1-13. [ Links ]
10. Nishimori I, Tamakoshi A, Otsuki M. Prevalence of autoimmune pancreatitis in Japan from a nationwide survey in 2002. J Gastroenterol. 2007;42:6-8. [ Links ]
11. Hardacre JM, Iacobuzio-Donahue CA, Sohn TA, Abraham SC, Yeo CJ, Lillemoe KD, et al. Results of pancreaticoduodenectomy for lymphoplasmacytic sclerosing pancreatitis. Ann Surg. 2003;237:853-9. [ Links ]
12. Abraham SC, Wilentz RE, Yeo CJ, Sohn TA, Cameron JL, Boitnott JK, et al. Pancreaticoduodenectomy (Whipple resections) in patients without malignancy: are they all 'chronic pancreatitis'? Am J Surg Pathol. 2003;27:110-20. [ Links ]
13. Pezzilli R. Acute recurrent pancreatitis: an autoimmune disease? World J Gastroenterol. 2008;14:999-1006. [ Links ]
14. Frulloni L, Scattolini C, Falconi M, Zamboni G, Capelli G, Capelli P, et al. Autoimmune pancreatitis: differences between the focal and diffuse forms in 87 patients. Am J Gastroenterol. 2009;104:2288-94. [ Links ]
15. Ghazale A, Chari ST, Zhang L, Smyrk TC, Takahashi N, Levy MJ, et al. Immunoglobulin G4-associated cholangitis: clinical profile and response to therapy. Gastroenterology. 2008;134:706-15. [ Links ]
16. Raina A, Yadav D, Krasinskas AM, McGrath KM, Khalid A, Sanders M, et al. Evaluation and management of autoimmune pancreatitis: experience at a large US center. Am J Gastroenterol. 2009;104:2295-306. [ Links ]
17. Church NI, Pereira SP, Deheragoda MG, Sandanayake N, Amin Z, Lees WR, et al. Autoimmune pancreatitis: Clinical and radiological features and objective response to steroid therapy in a UK series. Am J Gastroenterol. 2007;102:2417-25. [ Links ]
18. Sandanayake NS, Church NI, Chapman MH, Johnson GJ, Dhar DK, Amin Z, et al. Presentation and management of post-treatment relapse in autoimmune pancreatitis/ immunoglobulin G4-associated cholangitis. Clin Gastroenterol Hepatol. 2009;7:1089-96. [ Links ]
19. Chari ST, Takahashi N, Levy MJ, Smyrk TC, Clain JE, Pearson RK, et al. A diagnostic strategy to distinguish autoimmune pancreatitis from pancreatic cancer. Clin Gastroenterol Hepatol. 2009;7:1097-103. [ Links ]
20. Kamisawa T, Egawa N, Nakajima H, Tsuruta K, Okamoto A, Kamata N. Clinical difficulties in the differentiation of autoimmune pancreatitis and pancreatic carcinoma. Am J Gastroenterol. 2003;98:2694-9. [ Links ]
21. Chari ST, Smyrk TC, Levy MJ, Topazian MD, Takajashi N, Zhang L, et al. Diagnosis of autoimmune pancreatitis: the Mayo Clinic experience. Clin Gastroenterol Hepatol. 2006;4:1010-6. [ Links ]
22. Eerens I, Vanbeckevoort D, Vansteenbergen W, Van Hoe L. Autoimmune pancreatitis associated with primary sclerosing cholangitis: MR imaging findings. Eur Radiol. 2001;11:1401-4. [ Links ]
23. Irie H, Honda H, Baba S, Kuroiwa T, Yoshimitsu K, Tajima T, et al. Autoimmune pancreatitis: CT and MR characteristics. AJR Am J Roentgenol. 1998;170:1323-7. [ Links ]
24. Varadarajulu S, Cotton PB. Autoimmune pancreatitis: is it relevant in the west? Gastroenterology. 2003;125:1557-8. [ Links ]
25. Park DH, Kim MH, Chari ST. Recent advances in autoimmune pancreatitis. Gut. 2009;58:1680-9. [ Links ]
26. Nishimori I, Tamakoshi A, Kawa S, Tanaka S, Takeuchi K, Kamisawa T, et al. Influence of steroid therapy on the course of diabetes mellitus in patients with autoimmune pancreatitis: findings from a nationwide survey in Japan. Pancreas. 2006;32:244-8. [ Links ]
27. Members of the Autoimmune Pancreatitis Diagnostic Criteria Committee, the Research Committee of Intractable Diseases of the Pancreas supported by the Japanese Ministry of Health, Labor and Welfare, and Members of the Autoimmune Pancreatitis Diagnostic Criteria Committee, the Japan Pancreas Society. Clinical diagnostic criteria of autoimmune pancreatitis 2006. Suizo. 2006;21:395-7. [ Links ]
28. Otsuki M, Chung JB, Okazaki K, Kim MH, Kamisawa T, Kawa S, et al. Asian diagnostic criteria for autoimmune pancreatitis: consensus of the Japan-Korea symposium on autoimmune pancreatitis. J Gastroenterol. 2008;43:403-8. [ Links ]
29. Kim MH, Lee TY. Diagnostic criteria for autoimmune pancreatitis (AIP); a proposal of revised Kim criteria. J Gastroenterol Hepatol. 2007;22:104. [ Links ]
30. Okazaki K, Kawa S, Kamisawa T, Naruse S, Tanaka S, Nishimori I, et al. Clinical diagnostic criteria of autoimmune pancreatitis: revised proposal. J Gastroenterol. 2006;41:626-31. [ Links ]
31. Numata K, Ozawa Y, Kobayashi N, Kubota T, Akinori N, Nakatani Y, et al. Contrast-enhanced sonography of autoimmune pancreatitis: comparison with pathologic findings. J Ultrasound Med. 2004;23:199-206. [ Links ]
32. Notohara K, Burgart LJ, Yadav D, Chari S, Smyrk TC. Idiopathic chronic pancreatitis with periductal lymphoplasmacytic infiltration: clinicopathologic features of 35 cases. Am J Surg Pathol. 2003;27:1119-27. [ Links ]
33. Zamboni G, Luttges J, Capelli P, Frulloni L, Cavallini G, Pederzoli P, et al. Histopathological features of diagnostic and clinical relevance in autoimmune pancreatitis: a study on 53 resection specimens and 9 biopsy specimens. Virchows Arch. 2004;445:552-63. [ Links ]
34. Irie H, Ito T. US, CT and MRI findings of autoimmune pancreatitis based on ''Clinical diagnostic criteria of autoimmune pancreatitis 2006''. Suizo. 2007;22:629-33. [ Links ]
35. Yang DH, Kim KW, Kim TK, Park SH, Kim SH, Kim MH, et al. Autoimmune pancreatitis: radiologic findings in 20 patients. Abdom Imaging. 2006;31:94-102. [ Links ]
36. Okazaki K, Uchida K, Ohana M, Nakase H, Uose S, Inai M, et al. Autoimmune-related pancreatitis is associated with autoantibodies and a Th1/Th2-type cellular immune response. Gastroenterology. 2000;118:573-81. [ Links ]
37. Frulloni L, Lunardi C, Simone R, Dolcino M, Scattolini C, Falconi M, et al. Identification of a novel antibody associated with autoimmune pancreatitis. N Engl J Med. 2009;361:2135-42. [ Links ]
38. Kamisawa T, Yoshiike M, Egawa N, Nakajima H, Tsuruta K, Okamoto A. Treating patients with autoimmune pancreatitis: results from a long-term follow-up study. Pancreatology. 2005;5:234-40. [ Links ]
39. Hirano K, Tada M, Isayama H, Yagioka H, Sasaki T, Kogure H, et al. Long-term prognosis of autoimmune pancreatitis with and without corticosteroid treatment. Gut. 2007;56:1719-23. [ Links ]
40. Moon SH, Kim MH, Park DH, Hwang CY, Park SJ, Lee SS, et al. Is a 2-week steroid trial after initial negative investigation for malignancy useful in differentiating autoimmune pancreatitis from pancreatic cancer? A prospective outcome study. Gut. 2008;57:1704-12. [ Links ]
41. Okazaki K, Kawa S, Kamisawa T, Ito T, Inui K, Irie H, et al. Japanese clinical guidelines for autoimmune pancreatitis. Pancreas. 2009;38:849-66. [ Links ]
42. Nishimori I, Okazaki K, Kawa S, Otsuki M. Treatment for autoimmune pancreatitis. J Biliary Tract Pancreas. 2007;28:961-6. [ Links ]
43. Kamisawa T, Shimosegawa T, Okazaki K, Nishino T, Watanabe H, Kanno A, et al. Standard steroid treatment for autoimmune pancreatitis. Gut. 2009;58:1504-7. [ Links ]
44. Kamisawa T, Egawa N, Nakajima H, Tsuruta K, Okamoto A. Morphological changes after steroid therapy in autoimmune pancreatitis. Scand J Gastroenterol. 2004;39:1154-8. [ Links ]
45. Wakabayashi T, Kawaura Y, Satomura Y, Watanabe H, Motoo Y, Sawabu N. Long-term prognosis of duct-narrowing chronic pancreatitis: strategy for steroid treatment. Pancreas. 2005;30:31-9. [ Links ]
46. Nishimori I, Otsuki M. Study about steroid therapy for autoimmune pancreatitis. Annual reports of Research Committee of Intractable Pancreatic Diseases supported by Ministry of Health. Labour and Welfare of Japan. 2008;137-44. [ Links ]
47. Rueda JC, Duarte-Rey C, Casas N. Successful treatment of relapsing autoimmune pancreatitis in primary Sjogren's syndrome with Rituximab: report of a case and review of the literature. Rheumatol Int. 2009;29:1481-5. [ Links ]
