










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Colombiana de Reumatología
versión impresa ISSN 0121-8123
Rev.Colomb.Reumatol. vol.22 no.3 Bogotá jul./sep./ 2015
https://doi.org/10.10167j.rcreu.2015.05.006
http://dx.doi.org/10.10167j.rcreu.2015.05.006
Original Investigation
The epidemiology of rheumatoid arthritis in a cohort of Colombian
patients
Epidemiología de la artritis reumatoide en una cohorte de pacientes colombianos
Jorge Enrique Machado-Albaa,*, Andrés Felipe Ruizb, Diego Alejandro Medina Moralesc
a Director Grupo de Investigación en Farmacoepidemiología y Farmacovigilancia, Universidad Tecnológica de Pereira-Audifarma S.A. Pereira, Colombia
b Director Farmacoeconomía-Audifarma S.A. Bogotá, Colombia
c Grupo de Investigación en Farmacoepidemiología y Farmacovigilancia, Facultad Ciencias de la Salud, Universidad Tecnológica de Pereira-Audifarma, S.A., Pereira, Colombia
* Corresponding author. E-mail address: machado@utp.edu.co (D.A. Medina Morales).
Article history: Received 23 February 2015 Accepted 29 May 2015 Available online 11 July 2015
Abstract
Background: Rheumatoid arthritis (RA) is a chronic autoimmune disease with an estimated prevalence of between 0.8% and 1.0%. It is most common in women. Epidemiological RA data in Colombia is scarce. The objective was to determine epidemiological and pharmacological characteristics of a population diagnosed with RA across 5 Colombian cities between the years 2009 and 2013.
Methods: A descriptive study was developed that used information from medical records at a rheumatology patients care facility. The records were identified according to the keywords "rheumatoid arthritis". The socio-demographic, clinical, para-clinical and pharmacological variables were then recorded. The analysis was performed using IBM SPSS-22.0 software.
Results: Out of a total of 1364 patients, disease prevalence was estimated at 0.15%, with a mean age of 53.2 ± 13.9. The symptoms started at 41.3 ± 14.0 years old, and 81.9% were women. The DAS-28 (Disease Activity Score in 28 joints) mean was 3.46, and 12.9% of the patients were smokers. Osteoporosis (32.3% of patients) and high blood pressure (32.1%) were the most common comorbidities, while methotrexate was the most prescribed medication (98.4%).
Conclusions: This is the first study in Colombia to use a large cohort in order to gather valid information that establishes clinical characteristics, disease behavior, comorbidities, and medication trends in the country.
Keywords: Anti-rheumatic agents, Juvenile arthritis, Rheumatoid arthritis, Epidemiology, Methotrexate, Colombia (DeCS).
Resumen
Antecedentes: La artritis reumatoide (AR) es una enfermedad crónica autoinmune, cuya prevalencia se estima en 0,8-1,0% y es más frecuente en mujeres. Los datos epidemiológicos sobre AR en Colombia son escasos. El objetivo fue determinar las características epidemiológicas y farmacológicas de una población con diagnóstico de AR, en 5 ciudades de Colombia, durante los años 2009 a 2013.
Métodos: Se realizó un estudio descriptivo a partir de la información de historias clínicas de una institución de atención a pacientes reumatológicos. Se identificaron según la palabra clave artritis reumatoide y se identificaron las variables socio-demográficas, clínicas, paraclínicas y farmacológicas. El análisis se hizo mediante IBM-SPSS 22.0.
Resultados: De un total de 1.364 pacientes, se estimó una prevalencia de enfermedad de 0,15%, con edad promedio 53,2 ± 13,9 años y de inicio de síntomas 41,3 ± 14,0 años. El 81,9% fue de sexo femenino. La media de DAS-28 fue 3,46. El 12,9% de pacientes era fumador. La osteoporosis (32,3% de pacientes) e hipertensión arterial (32,1%) fueron las comorbilidades más frecuentes y metotrexate (98.4%) el medicamento más prescrito.
Conclusiones: Es el primer estudio en Colombia que utiliza una cohorte amplia y aporta información válida que establece las características clínicas, comportamiento de la enfermedad, comorbilidades y tendencias de la medicación en el país.
Palabras clave: Agentes antirreumáticos, artritis juvenil, artritis reumatoide, epidemiologia, metotrexate, Colombia (DeCS).
Introduction
Rheumatoid arthritis (RA) is a chronic disease characterized by inflammation, pain, the destruction of synovial joints and systemic manifestations including cardiovascular, lung, bone and psychological involvements which lead to severe disability and premature mortality.1-4 It is considered an autoimmune disease because of the presence of autoantibodies such as rheumatoid factor (RF) and anti-citrullinated peptides (ACPA) or (cyclic citrullinated peptide [anti-CCPs] antibodies) that may be found and precede clinical manifestations of the disease by several years.1 The prevalence for RA is estimated at 0.8-1.0% across the general population, affecting 2-4 times more women than men. Its prevalence increases with age and gender differences decrease.3-7 It is estimated that the incidence in the United States is at 25 per 100,000 men and 54 per 100,000 women, which means that about 2.1 million people have the disease. Most European and North American studies estimate an average annual incidence of 0.02-0.05%.8 The age of onset is usually between 30 and 50 years old and this is related to the interaction of environmental agents and the person's individual genetic predisposition.3,4,6,7 Juvenile RA and the elderly-onset RA (older than 65 years old) may also occur.7 In Colombia little available data exists that characterizes RA and variables related to its clinical behavior. The study attempted to determine socio-demographics, clinical, para-clinical and pharmacological variables in a cohort of patients diagnosed with RA in five cities.
Materials and methods
Taking as a base a population of 858,045 patients from the contributory scheme of the Health System of Colombia (SGSSS), Health Assurance Company (EPS) affiliates was selected from all ages and both genders with a diagnostic in medical record that included the words "rheumatoid arthritis." This was carried out in five of Colombia's main cities (Bogotá, Cali, Manizales, Medellin, and Pereira) in patients who had been treated at the Service Providing Institution in the application of medications (IPS-Especializada de Audifarma S.A.) between December 2009 and August 2013. Diagnoses according to the International Classification of Diseases (ICD-10), were: (1) Rheumatoid arthritis, unspecified (M069). (2) Arthritis, unspecified (M159). (3) Seropositive rheumatoid arthritis, not otherwise specified (M059). (4) Juvenile arthritis, unspecified (M080). (5) Seronegative rheumatoid arthritis (M060). (6) Juvenile rheumatoid arthritis (M080). (7) Other seropositive rheumatoid arthritis (M058) and (8) Other specified rheumatoid arthritis (M068). All diagnoses were made by physician who specializes in rheumatology.
Information was obtained by a team of four physicians trained for this purpose and the data was reviewed and audited by a pharmacoepidemiologist who recorded them in an Excel database for initial analysis. The following variables were considered: socio-demographic: age, gender, educational level. Clinical: specific diagnosis according to the ICD-10, age of the onset of symptoms, age at moment of diagnosis, progression time of the disease, DAS-28 mean, comorbidities. Pharmacological: the international non-proprietaryname (generic) of disease-modifying antirheumatic drug (DMARDs) which were being received. Behavioral factors were also described such as those who were smokers and the active consumption of alcohol (yes/no).
Information from the Excel® database was analyzed using IBM-SPSS 22.0 software for Windows (IBM Chicago Illinois, USA). Data was expressed in frequencies and percentages.
The study was classified as non-risk research and received endorsement from the Universidad Tecnológica de Pereira's Bioethics Committee, under Ministry of Health Resolution 8430 of 1993 that sets forth the principles of scientific research according to the Declaration of Helsinki.
Results
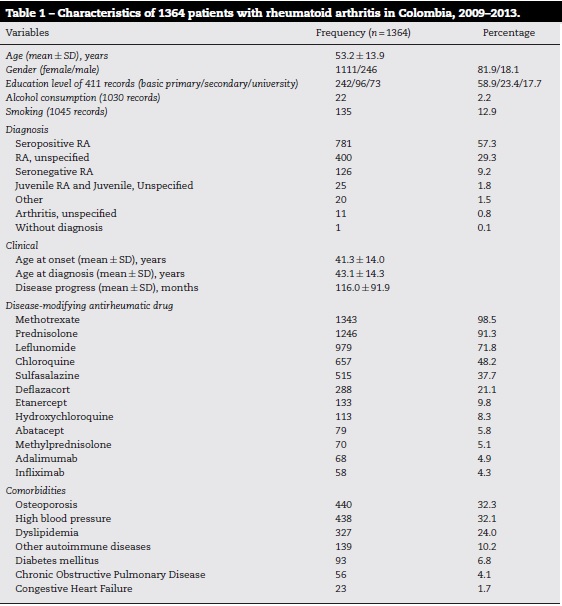
A total of 1364 patients were found that complied with the inclusion criteria. The estimated disease prevalence was 0.15%. General results showed that the average age of patients was 53.2 ±13.9 years old. 81.8% of patients were women. The male:female ratio was 4.5:1.0. The average age for the onset of symptoms was 41.3 years old and the average time of disease duration was 116 months (data from 710 patients where the date at which symptoms started was established). Most people had only attained a basic primary education level. A very low percentage of patients admitted to being smokers or consumers of alcoholic drinks. In 87 (55.8%) of 156 patients who had information on X-rays of hands or feet erosions were found. The most common diagnoses in order of frequency were: seropositive RA, unspecified RA and seronegative RA (Table 1). The average DAS-28 at the beginning of the cohort was 3.43. Remission was found in 20.2% (n = 216) of patients, while 39.7% (n = 425) had mild, 34.6% (n = 370) moderate and 5.5% (n = 59) to high disease activity. The most common comorbidities included: osteoporosis, high blood pressure, dyslipidemia and other autoimmune diseases (Table 1). Methotrexate was the most prescribed DMARD followed by Prednisolone, Leflunomide, Chloroquine and Sulfasalazine (Table 1).
Discussion
As part of the study, data for the distribution of various variables were obtained in individuals diagnosed with RA across five of Colombia's main cities between 2009 and 2013. Since there are no population databases that estimate the prevalence of the disease in the country, these findings provide important information regarding the understanding of this condition. Discovering that 0.15% of this population has or is being treated for RA is an indicator that may reflect an under-diagnosis of the disease and that few patients have easy and timely access to treatment. Furthermore, the disease's prevalence in Colombia is lower than in other countries where statistics have estimated that the prevalence is between 0.5% and 1.0% of the population, although the incidence of the disease has shown variations depending on geographical location.9,10
While international literature shows that the disorder is three times more common in females, in this study's cohort it was found that this figure was 4.5 times more common in women than in men. More research is needed in order to explain this difference.9,11,12 Differences were also found in the age of patients as this cohort was younger than those reported in Albania (53.2 vs. 62.4 years old),11 but older than those reported in Greece (46.8 years old),13 while the progress time of the disease is also slightly higher than the figure reported by Kirchhoff et al. (9.6 years old in Colombia vs. 8.0 years old in Germany).14 No available data was found on comorbidities that accompanied the patient with RA. However, association with osteoporosis, high blood pressure and dyslipidemia are not surprising because there have already been reports across the country of patients with these morbidities and the use of anti-inflammatory drugs.15,16 The use of DMARDs such as Methotrexate and Leflunomide as the most prescribed examples is consistent throughout the literature which supports its use as a first-line of treatment and leaves biotechnology drug products as alternatives in managing refractory patients.3,4,7,14,17
According to the above, these findings are related to some extent with data published by other authors, however, this study in the country to use a large cohort, valuable information is provided that establishes clinical characteristics, disease behavior, comorbidities and medication trends in Colombia, allowing the epidemiological profile of patients with RA to be determined.
This study has several limitations that must be recognized, among them the study population included only patients with a specific institution and for certain variables analyzed no information available in the medical record and the ICD-10 considered can create a selection bias.
Since information was obtained from patients affiliated to just one insurer covering about 5.0% of the Colombian population, results may only be extrapolated to groups with equal insurance conditions. Therefore more studies are needed so as to estimate across all population groups in the country what the disease's incidence and prevalence is, how patients are being treated and what the costs of this care are.
Ethical responsibilities
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of Data The authors declare that no patient data appears in this article.Right to privacy and informed consent
The authors declare that no patient data appears in this article.
Sources of funding
Universidad Tecnológica de Pereira, Audifarma S.A. Grant number: 2012-13
Conflicts of interest
The authors declare that Pfizer Colombia financed the data collection process in medical records. There was no intervention in the stages of processing, analysis or publication of that data.
References
1. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62:2569-81. [ Links ]
2. McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med. 2011;365:2205-19. [ Links ]
3. Wasserman AM. Diagnosis and management of rheumatoid arthritis. Am Fam Phys. 2011;84:1245-52. [ Links ]
4. Davis JM, Matteson EL, American College of Rheumatology, European League Against Rheumatism. My treatment approach to rheumatoid arthritis. Mayo Clin Proc. 2012;87:659-73. [ Links ]
5. van Vollenhoven RF. Sex differences in rheumatoid arthritis: more than meets the eye. BMC Med. 2009; 7:12. [ Links ]
6. Moura MC, Zakszewski PT, Silva MB, Skare TL. Epidemiological profile of patients with extra-articular manifestations of rheumatoid arthritis from the city of Curitiba, south of Brazil. Rev Bras Reumatol. 2012;52: 686-94. [ Links ]
7. Birch JT, Bhattacharya S. Emerging trends in diagnosis and treatment of rheumatoid arthritis. Prim Care. 2010;37: 779-92. [ Links ]
8. Alamanos Y Drosos AA. Epidemiology of adult rheumatoid arthritis. Autoimmun Rev. 2005;4:130-6. [ Links ]
9. Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet. 2010;376:1094-108. [ Links ]
10. Jordan K, Clarke AM, Symmons DP, Fleming D, Porcheret M, Kadam UT, et al. Measuring disease prevalence: a comparison of musculoskeletal disease using four general practice consultation databases. Br J Gen Pract. 2007; 57:7. [ Links ]
11. Duraj V, Tafaj A, Backa T. Epidemiology of rheumatoid arthritis in Tirana, Albania. Mater Sociomed. 2013;25: 96-7. [ Links ]
12. Costenbader KH, Chang SC, Laden F Puett R, Karlson EW. Geographic variation in rheumatoid arthritis incidence among women in the United States. Arch Intern Med. 2008;168:1664. [ Links ]
13. Anagnostopoulos I, Zinzaras E, Alexiou I, Papathanasiou AA, Davas E, Koutroumpas A, et al. The prevalence of rheumatic diseases in central Greece: a population survey. BMC Musculoskelet Disord. 2010;11:98. [ Links ]
14. Kirchhoff T, Ruof J, Mittendorf T, Rihl M, Bernateck M, Mau W, et al. Cost of illness in rheumatoid arthritis in Germany in 1997-98 and 2002: cost drivers and cost savings. Rheumatology (Oxford). 2011;50:756-61. [ Links ]
15. Isaza CA, Osorio FJ, Mesa G, Moncada JC. Patrones de uso de antihipertensivos en 11.947 pacientes colombianos. Biomédica. 2002;22:476-85. [ Links ]
16. Machado JE, Moncada JC, Mesa G. Prescription patterns for antilipidemic drugs in a group of Colombian patients. Rev Panam Salud Publica. 2008;23:179-87. [ Links ]
17. Machado-Alba JE, Ruiz AF, Machado-Duque ME. Adverse drug reactions associated with the use of disease-modifying anti-rheumatic drugs in patients with rheumatoid arthritis. Rev Panam Salud Publica. 2014;36:396–401. [ Links ]
