










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Colombiana de Reumatología
versão impressa ISSN 0121-8123
Rev.Colomb.Reumatol. vol.25 no.1 Bogotá jan./mar. 2018
https://doi.org/10.1016/j.rcreu.2017.08.004
Review Papers
Pharmacogenomics of etanercept, infliximab, adalimumab and methotrexate in rheumatoid arthritis. A structured review✩
a Facultad de Ciencias Farmacéuticas y Alimentarias, Universidad de Antioquia, Medellín, Colombia
b Laboratorio de Biología Molecular, Hospital Universitario Pablo Tobón Uribe, Medellín, Colombia
c Facultad de Farmacia, Universidad de Granada, Granada, España
Introduction:
Individual genetic variability favors the capacity of response and toxicity to the drugs is different in each person. Rheumatoid arthritis reported rates of response to the drugs etanercept, infliximab, adalimumab and methotrexate is close to 60%. This variability can be explained by genetic polymorphisms characteristic of each patient.
Objective:
To identify genetic polymorphisms reported in scientific articles that may affect the pharmacokinetics and pharmacodynamics of etanercept, infliximab, adalimumab, and methotrexate, and their response in patients with rheumatoid arthritis.
Materials and method:
A systematic search was performed in PubMed and Medline, with the key terms: "rheumatoid arthritis" and "pharmacogenomic" and "polymorphisms" and "methotrexate" and "infliximab" and "adalimumab" and "etanercept", obtaining 164 articles, 117 non-duplicates, and 19 articles that met the inclusion criteria.
Results:
Of the 19 articles, 2 reported polymorphisms affecting the pharmacokinetics of infliximab, adalimumab, etanercept, methotrexate, and 17, pharmacodynamics. In the 19 articles, 23 polymorphisms of clinical relevance were identified in European, Japanese, Jordanian, and Indian populations.
Conclusions:
A total of 23 polymorphisms with clinical relevance were identified, which could be the basis for the design of a specific test sequencing in rheumatoid arthritis patients being considered for treatment with infliximab, adalimumab, etanercept, or methotrexate. The practical usefulness of this strategy requires evidence in specific clinical studies, associated with a targeted and personalized genetic test, and its effect on the effectiveness and safety of drug therapy with these drugs prescription.
Keywords: Pharmacogenomics; Rheumatoid arthritis; Polymorphism; Etanercept; Infliximab; Adalimumab; Methotrexate
Introducción:
La variabilidad genética individual favorece que la capacidad de respuesta y toxicidad a los fármacos sea diferente en cada persona. En la artritis reumatoide se reportan índices de respuesta a los medicamentos etanercept, infliximab, adalimumab y metotrexato cercanos al 60%. Esta variabilidad puede explicarse por polimorfismos genéticos característicos de cada paciente.
Objetivo:
Identificar polimorfismos genéticos reportados en artículos científicos que pueden afectar la farmacocinética y la farmacodinámica de etanercept, infliximab, adalimumab y metotrexato, y su respuesta en pacientes con artritis reumatoide.
Materiales y método:
Se realizó una búsqueda sistemática en PubMed/Medline, con los términos clave: «rheumatoid arthritis» and «pharmacogenomic» and «polymorphisms» and «metotrexato» and «infliximab» and «adalimumab» and «etanercept» obteniendo 164 artículos, 117 no duplicados y 19 artículos que cumplieron los criterios de inclusión. Resultados: De los 19 artículos, 2 reportaron polimorfismos que afectan la farmacocinética de infliximab, adalimumab, etanercept y metotrexato, y 17, la farmacodinámica. En los 19 artículos se identificaron 23 polimorfismos de relevancia clínica en población europea, japonesa, jordana e india.
Conclusiones:
Se identifican 23 polimorfismos de relevancia clínica, los cuales podrían ser el soporte para el diseño de un test de secuenciación específica en pacientes con artritis reumatoide, en los que se considere la utilización de infliximab, adalimumab, etanercept o metotrexato. La utilidad práctica de este tipo de estrategia requiere ser evidencia en estudios clínicos específicos, relacionados con una prescripción orientada por test genéticos y personalizada, y su efecto sobre la efectividad y seguridad de la farmacoterapia con estos medicamentos.
Palabras clave: Farmacogenómica; Artritis reumatoide; Polimorfismo; Etanercept; Infliximab; Adalimumab; Metotrexato
Introduction
Human beings exhibit genetic variation associated with differences in their DNA sequences, which entails that the capacity to respond to the therapeutic and toxic effects of the drugs may be different in each individual.1,2 The discipline that studies this genetic variability in the response to a drug, at an individual level, is pharmacogenetics; meanwhile, pharmacogenomics also includes the environmental variables thereof. 3-5 These disciplines are useful in clinical practice to predict the individual response of patients to different drugs, especially for the treatment of autoimmune diseases. 6 Rheumatoid arthritis (RA) is a chronic heterogeneous autoimmune disease that causes inflammation in the synovial membrane, the cartilage and the bone; and over time it generates deformity, disability and deterioration in the quality of life. 7,8 Among the drugs used in its treatment are the inhibitors of tumor necrosis factor alpha (TNF- α) etanercept, infliximab, adalimumab, which report a response rate of 40%, and methotrexate (MTX) with 50%.8 This variability can occur due to genetic single-nucleotide polymorphisms that affect the pharmacokinetics and pharmacodynamics of these drugs.
A systematic review of the International Journal of Rheumatology in 2013 reports that approximately 50% of patients with RA in Europe interrupt their TNF- α inhibitor during the first 5 years due to problems of effectiveness or safety of the respective medication. 9 Similarly, the Brigham and Women's Hospital Rheumatoid Arthritis Sequential Study (BRASS), conducted in Boston, reports that 42% of patients with RA informed the withdrawal of their anti-TNF- α treatment. 10 In this context of a large number of patients who discontinue the treatment with anti-TNF- α, the generation of information that improves the ability to predict which patients will respond to specific therapies would be a significant contribution in the proper management of RA.
The mentioned problems of effectiveness and safety could be associated with the genetic variability of each patient, including the environmental variables, which are expressed by genetic polymorphisms. In general, a genetic polymorphism is a variation in a determined DNA sequence present in more than 1% of the individuals of a population. 11 According to the Canary Institute for Cancer Research "they are classified into: variable number of tandem repeats polymorphism (VNTR), restriction fragment length polymorphisms (RFLP) and single nucleotide polymorphisms (SNP)". 12 In this context, the genetic variability is associated in 90% with SNPs, due to the activity of the genes dependent on enzymes involved in the pharmacokinetics or pharmacodynamics of the drugs used in the treatment of RA, thus affecting their efficacy and safety. 13
RA is a major public health problem; in the last years, better health outcomes have been achieved with the incorporation of synthetic and biological disease modifying drugs. However, problems of variability in response are reported, which lead to ineffectiveness and adverse reactions in 30%-40% of patients. 14 In this sense, pharmacogenomics, through the study of genetic variants of proteins involved in the pharmacokinetics and pharmacodynamics of the drugs, becomes a way to maximize the efficacy and safety of the pharmacotherapy. In this aspect, pharmacogenomics favors a better understanding of the biological mechanisms and thus, the development of clinical models that predict the antirheumatic drug with greater benefit for each patient.
It is estimated that at 10 years of evolution of the RA, almost 80% of patients have some degree of limitation. The prognosis is uncertain and the lesions, which appear in the first years of disease, may continue despite clinical improvement, since the pathogenesis of these lesions may differ from a simple acute joint inflammation. 15
Common risk factors regarding the development of RA, such as smoking, female sex, the presence of HLA DRB1 and the educational level, have been found in Colombia. 16
Epidemiological data
In Canada and the United States the prevalence ranges between 0.8% and 1.1%.17,18 Similarly, the data of prevalence in Europe range between 0.5% and 1%.19,20 In Latin America, it has been reported between 0.45% and 0.9%.21-23 On the other hand, different studies show that the incidence of RA tends to decrease; thus, between 1955 and 1994 the incidence would have been reduced by 50%.24 In Europe, the reported incidence rates of RA range between 0.009%-0.045%; in North America they vary between 0.024%-0.075% in Caucasian population and between 0.09%-0.89% in American Indian population. Although it is not clear, several factors have been proposed to explain the differences in incidence, among which are genetic, environmental and cultural factors. 25
Etiology and pathogenesis of rheumatoid arthritis
RA is characterized by the presence of rheumatoid factor and anti-citrullinated peptide antibodies. It is observed in the initial phase of RA and involves the activation of both T and B cells. Proinflammatory cytokines, such as TNF, IL-1 and IL-17, stimulate the inflammation and degradation of bone and cartilage. However, there is no decrease in the number of Treg cells, which could contribute to the pathophysiology of the disease. 26
Genetic susceptibility
It is estimated that up to 66% of patients with RA have genetic risk, which has been associated with the presence of certain alleles of the major histocompatibility complex, especially with the HLA-DR4 type. In this sense, it is accepted that the disease is associated with a given genetic load that generates a greater susceptibility to the immune response against an antigen (Ag) and thus, inflammation of the synovial membrane and osteoarticular destruction is generated. 27
Globally, individuals respond to pharmacotherapy in a different way and no medication is 100% effective in all patients, 28 which may be due to an alteration in the pharmacokinetics and pharmacodynamics of the drugs associated with genetic-environmental conditions. 29 In this context, the study of pharmacogenomic candidate genes has been more successful than the study of the candidate genes of the disease in identifying and explaining the variation of the pharmacological response, 30 which has favored personalized prescription. 31 Within this framework, it is necessary to have systematic information on the pharmacogenomics of RA, identifying polymorphisms of clinical relevance in the response and toxicity of TNF- α inhibitors and methotrexate. This type of information could contribute to the development of genetic tools to support the pharmacotherapeutic decision and improve the response to the treatment of this disease. Therefore, the objective of this work was to identify the polymorphisms to be used in the design of the specific sequencing test in patients with RA before the prescription of infliximab, adalimumab, etanercept and methotrexate.
Methods
Systematic review in PubMed/Medline. To identify the studies, a search in PubMed/Medline was conducted from September 2011 to September 2016, without limits in language and type of study, using the terms: "rheumatoid arthritis" and "pharmacogenomic" and "polymorphisms" and "methotrexate" and "infliximab" and "adalimumab" and "etanercept". Specifically, it was contemplated the combination of keywords and filters: "rheumatoid arthritis" [MeSH Terms] AND "pharmacogenomic" [MeSH Terms] AND "polymorphisms" [MeSH Terms] AND "methotrexate" [MeSH Terms] AND "infliximab" [MeSH Terms] AND "adalimumab" [MeSH Terms] and "etanercept" [MeSH Terms]. Studies that reported polymorphisms of a single nucleotide and that affected the efficacy and safety of infliximab, adalimumab, etanercept and methotrexate were defined as inclusion criteria.
Data extraction
The articles that met the inclusion criteria were analyzed for data extraction. It was created a data collection form that included: the author and reference of the article reporting the polymorphism, the medication(s) studied, the type of study, the year of publication, the population, the polymorphism of interest, its manifestation and the report or not of pharmacodynamic or pharmacokinetic variability. Finally, each identified polymorphism was searched in Hap Map, in order to identify the gene to which it belongs, together with its alias, the organism, lineage, location and exon.
Results
Applying the defined search criteria, 164 articles were found (25 related to infliximab, 24 to adalimumab, 35 to etanercept and 80 to methotrexate), of which 47 were repeated, remaining 117. Of this group of 117 articles, 19 met the inclusion criteria (Fig. 1). Of the 19 articles, two reported polymorphisms that affect the pharmacokinetics of infliximab, adalimumab, etanercept and methotrexate, which are associated with increased plasma concentrations, while 17 articles identified polymorphisms that affect their pharmacodynamics, which is associated with blockade of receptors and is manifested by ineffectiveness of the drugs (Table 1).
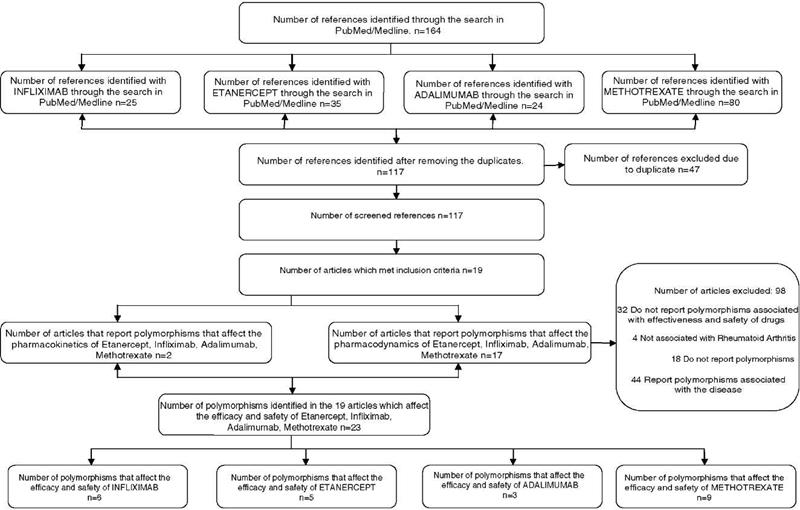
Table 1 - Single nucleotide polymorphisms associated with variability in pharmacokinetics and pharmacodynamics of methotrexate and tumor necrosis factor inhibitors: infliximab, etanercept, adalimumab.
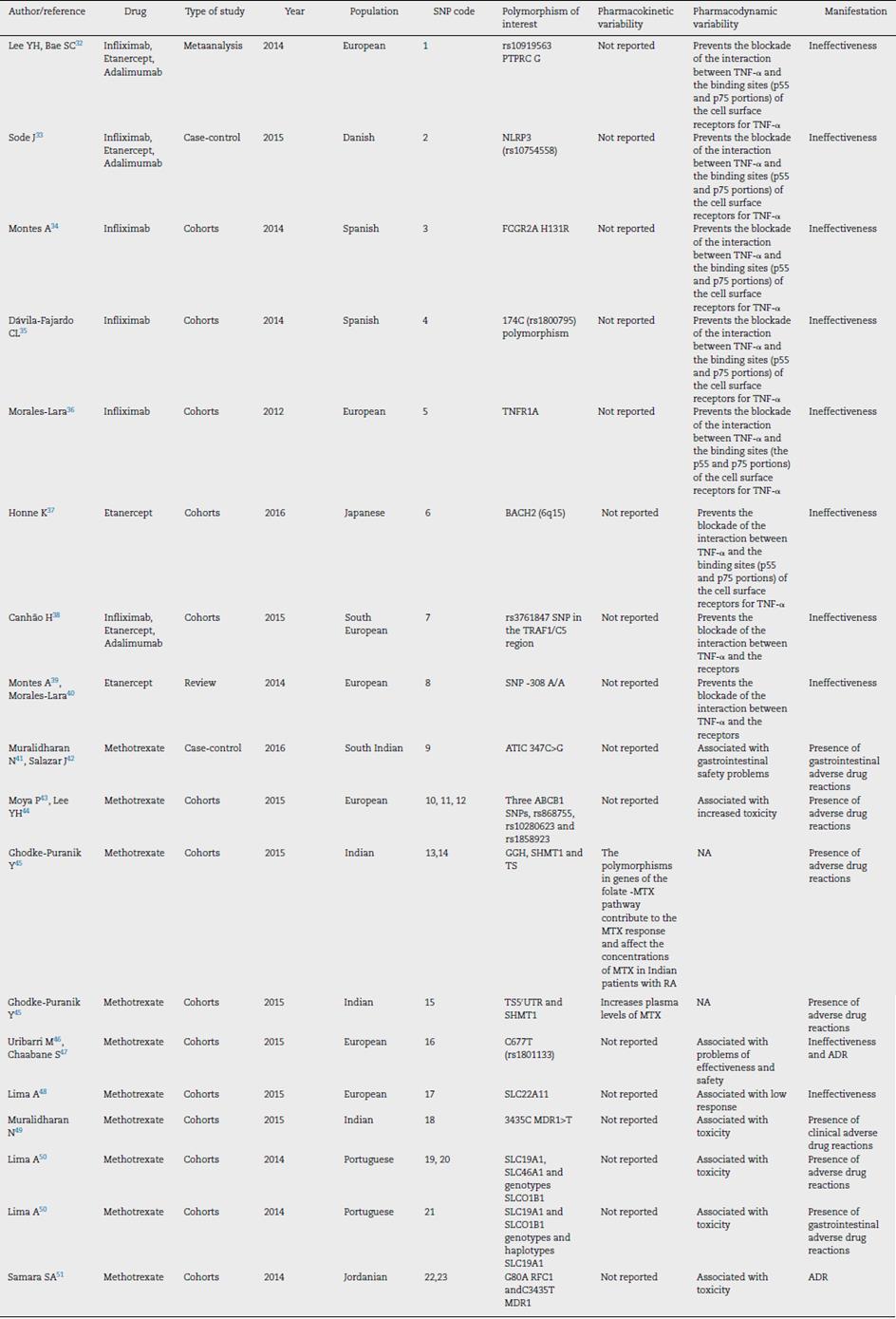
The 19 selected articles correspond to European, Japanese, Jordanian and Indian populations and they report the following 23 single nucleotide polymorphisms: rs10919563 PTPRC G, NLRP3 (rs10754558), FCGR2A H131R, 174C (rs1800795), TNFR1A, BACH2 (6q15), rs3761847 SNP in the TRAF1/C5 region, SNP -308 A/A, ATIC 347C>G, ABCB1 rs868755, rs10280623, rs1858923, GGH, SHMT1 and TS, TS50JTR, C677T (rs1801133), SLC22A11, 3435C MDR1>T, SLC19A1, SLC46A1 and SLCO1B1, G80A RFC1 and C3435T MDR1 genotypes (Table 1). Specifically, of these 23 polymorphisms, 6 were associated with infliximab, 5 with etanercept, 3 with adalimumab and 9 with methotrexate (Fig. 1).
The search of the 23 identified polymorphisms in the HapMap database allowed to register, for each of them, the gene that encodes it, the organism in which it is manifested, its lineage, its location or locus and the exon. In this sense, of the 23 identified polymorphisms stood out (Table 2):
Table 2 - Location and exons of genes identified with single nucleotide polymorphism that affect the effectiveness and safety of infliximab, etanercept, adalimumab and methotrexate.
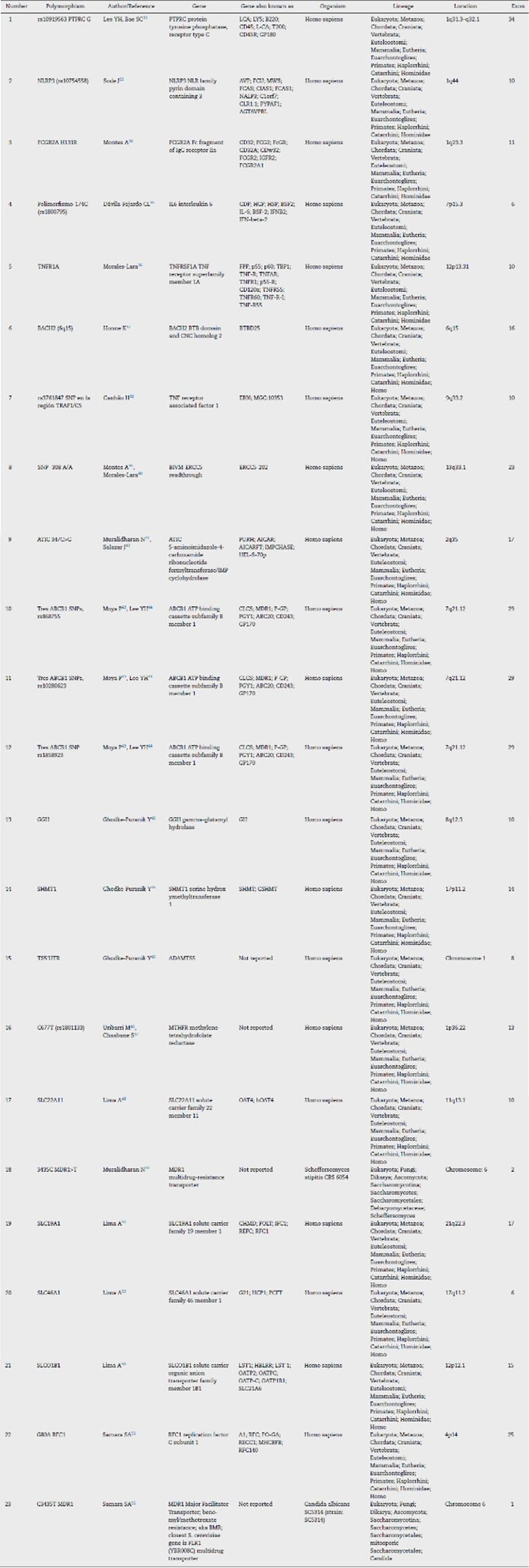
Nineteen (82.6%) correspond to the Homo sapiens species.
In the polypeptide sequence, the regions that are translated into amino acids come mainly from exon 10 (5 polymorphisms), from exon 29 (3 polymorphisms) and from exon 17 (2 polymorphisms).
The SLC gene (of different genetic families) was found associated with 4 polymorphisms, while the ABCB1 (ATP binding cassette subfamily B member 1) was found associated with 3 of the 23 polymorphisms and the MDR1 gene with 2 polymorphisms.
Discussion and conclusions
In RA, drugs such as methotrexate and TNF- α inhibitors like infliximab, adalimumab and etanercept are very important to achieve remission in patients; however, the genetic variability of the individuals implies that the capacity of response and toxicity to these medicines is different and that the reported rates are lower than 60%.8 Pharmacogenomics deals with the possible associations of genetic polymorphisms with responses to drugs, it is a branch of medical science that is still in its initial phase and requires more time to demonstrate positive results, so it depends on a good articulation between the research sector, legislation, pharmaceuticals companies and healthcare institutions that in the future, medicines can be developed for the benefit of improving health conditions and cost of treatments in small target groups; likewise, the value of non-genetic variables in the progression of a disease, such as age, gender, diet and lifestyle, which are also key in the response to a therapy, should not be left aside.
The relevance of this study consists in providing the possibility of applying the research of candidate genes selected for their biological importance, either in the kinetics or because of their relationship in the pharmacological action, in the identification of individuals at risk of experiencing adverse effects or with probability of being resistant to treatment. Therefore, it is expected that the information generated would be susceptible to be used in the design of specific sequencing tests, contributing to identify the best therapeutic option (greater effectiveness and safety) in patients with RA. 18
In the treatment of RA, the possibility of associating certain polymorphisms with the efficiency of the treatment, reducing the adverse effects of the use of a drug, can be of great value both for the patient and for the medical practice and its economic aspect. 1 The results obtained with this systematic review are a basis for the design of the specific sequencing test in patients with RA before the prescription of infliximab, adalimumab, etanercept and methotrexate; hence the importance of designing and validating with multicenter studies specific genomic tests that contribute to a personalized prescription to improve the effectiveness and safety of treatments with these drugs and achieve lower healthcare costs. The identification of the 23 polymorphisms of clinical relevance obtained with the review is very important for the design of genomic tests; however, it is necessary to include other genes in the multicentre studies, during exome sequencing, before validating and standardizing a test for use in clinical practice.
Acknowledgements
University of Antioquia, Colciencias, University Hospital Pablo Tobón Uribe.
REFERENCES
. Caskey CT. Using genetic diagnosis to determine individual therapeutic utility. Annu Rev Med. 2010;61:1-15. [ Links ]
2. Broder S, Venter JC. Sequencing the entire genomes of free-living organisms: The foundation of pharmacology in the new millennium. Annu Rev Pharmacol Toxicol. 2000;40:97-132. [ Links ]
3. Genetic Alliance; The New York-Mid-Atlantic Consortium for Genetic and Newborn Screening Services. Understanding Genetics: A New York, Mid-Atlantic Guide for Patients and Health Professionals. Washington (DC): Genetic Alliance; 2009 Jul 8. Disponible en: http://www.ncbi.nlm.nih.gov/books/NBK115563/. [ Links ]
4. Howard L McLeod, William E Evans. Pharmacogenomics: Unlocking the Human Genome for Better Drug Therapy. Department of Medicine, Division of Oncology, Washington University Medical School, St. Louis, Missouri. Annual Review of Pharmacology and Toxicology. Vol. 41: 101-121 (Volume publication date April 2001) DOI: 10.1146/annurev.pharmtox.41.1.101. [ Links ]
5. Hertz DL, Rae J. Pharmacogenetics of cancer drugs. Annu Rev Med . 2015;66:65-81, https://doi.org/10.1146/annurev-med-053013-053944. [ Links ]
6. Andrade, Luis E.C. Future perspective for diagnosis in autoimmune diseases. Anais da Academia Brasileira de Ciências. vol.81 no.3 Rio de Janeiro Sept. 2009. On-line version. Divisão de Reumatologia, Universidade Federal de São Paulo, Escola de Medicina, Rua Botucatu, São Paulo, SP, Brasil. Disponible en: https://doi.org/10.1590/S0001-37652009000300004. [ Links ]
7. Rielly DD, Rahman P. Pharmacogenetics of rheumatoid arthritis: Potential targets from susceptibility genes and present therapies. Pharmacogenomics Pers Med. 2010;3:15-31. [ Links ]
8. Tougaard P, Zervides KA, Skov S, Hansen AK, Pedersen AE. Biologics beyond TNF-a inhibitors and the effect of targeting the homologues TL1A-DR3 pathway in chronic inflammatory disorders. Immunopharmacol Immunotoxicol. 2016;38:29-38, https://doi.org/10.3109/08923973.2015.1130721. [ Links ]
9. Arora A, Mahajan A, Spurden D, Boyd H, Porter D. Long-term drug survival of TNF inhibitor therapy in RA patients: A systematic review of european national drug registers. Int J Rheumatol. 2013;2013:764518, https://doi.org/10.1155/2013/764518. [ Links ]
10. Agarwal SK, Glass RJ, Shadick NA, Coblyn JS, Anderson RJ, Maher NE, et al. Predictors of discontinuation of tumor necrosis factor inhibitors in patients with rheumatoid arthritis. J Rheumatol. 2008;35:1737-44. [ Links ]
11. Arribas, Ignacio Andrés. Farmacogenética y Variabilidad Interindividual. En: La Respuesta a los Medicamentos, 23 de Marzo de 2010. Academia de farmacia «Reino de Aragón» Zaragoza, [consultado 5 Abr 2016]. Disponible en: Disponible en: http://www.academiadefarmaciadearagon.es/docs/documentos/documento21.pdf . [ Links ]
12. Instituto Canario de Investigación del Cáncer. Research Journal ISS 1697-6452 [consultado 25 Abr 2016]. Disponible en: Disponible en: http://www.biocancer.com/journal/272/3-la-variacion-genica . [ Links ]
13 Tanaka E, Taniguchi A, Urano W, Yamanaka H, Kamatani N Pharmacogenetics of disease-modifying anti-rheumatic drugs. Best Pract Res Clin Rheumatol. 2004;18:33-47. [ Links ]
14. Prajapati R, Plant D, Barton A. Genetic and genomic predictors of anti-TNF response. Pharmacogenomics. 2011;12:1571-85, https://doi.org/10.2217/pgs.11.114. [ Links ]
15. Benito Ruiz P, Pros Simón A. ¿Por qué un tratamiento precoz en la artritis reumatoide? Medifam. 2001;11. [ Links ]
16. Muñetón Gerardo A, Quintana G. La epidemiología de la artritis reumatoide. Rev Colomb Reumatol. 2015;22:145-7. [ Links ]
17. Prajapati R, Plant D, Barton A. Genetic and genomic predictors of anti-TNF response. Pharmacogenomics . 2011;12:1571-85, https://doi.org/10.2217/pgs.11.114. [ Links ]
8. Zhou S, Di Y, Chan E, Du Y, Chow V, Xue C, et al. Clinical pharmacogenetics and potential application in personalized medicine. Curr Drug Metab. 2008;9:738-84. [ Links ]
19. Widdifield J, Paterson J, Bernatsky S, Tu K, Tomlinson G, Kuriya B, et al. The epidemiology of rheumatoid arthritis in Ontario, Canada. Arthritis Rheumatol. 2014;66: 786-93. [ Links ]
20. Malemba J, Mbuyi-Muamba J, Mukaya J, Bossuyt X, Verschueren P, Westhovens R. The epidemiology of rheumatoid arthritis in Kinshasa, Democratic Republic of Congo-A population-based study. Rheumatology. 2012;51:1644-7. [ Links ]
21. Neovius M, Simard JF, Askling J. Nationwide prevalence of rheumatoid arthritis and penetration of disease-modifying drugs in Sweden. Ann Rheum Dis. 2011;70:624-9. [ Links ]
22. Scublinsky D, Venarotti H, Citera G, Messina O, Scheines E, Rillo O, et al. The prevalence of rheumatoid arthritis in Argentina: A capture-recapture study in a city of Buenos Aires province. J Clin Rheumatol. 2010;16:317-21. [ Links ]
23. Senna ER, de Barros AL, Silva EO, Costa IF, Pereira LV, Ciconelli RM, et al. Prevalence of rheumatic diseases in Brazil: A study using the COPCORD approach. J Rheumatol . 2004;31:594-7. [ Links ]
24. Silman A. The changing face of rheumatoid arthritis: Why the decline in incidence? Arthritis Rheum. 2002;46:579-81. [ Links ]
25. Gorman JD, Lum RF, Chen JJ. Impact of shared epitope genotype and ethnicity on erosive disease: A meta-analysis of 3240 rheumatoid arthritis patients. Arthritis Rheum . 2004;50:400-12. [ Links ]
26. Mateen S, Zafar A, Moin S, Khan AQ, Zubair S. Understanding the role of cytokines in the pathogenesis of rheumatoid arthritis. Clinica Chimica Acta. 2016;455:161-71. [ Links ]
27. Uribe L, Gómez L, Amariles P. Guía de actuación farmacéutica en pacientes con artritis reumatoide. Medellín, Colombia: Medicarte; 2010. [ Links ]
28. Wilkinson G. Drug metabolism and variability among patients in drug response. N Engl J Med. 2005;352:2211-21. [ Links ]
29. Wijnen P, op den Buijsch R, Drent M, Kuijpers P, Kuipers P, Neef C, et al. The prevalence and clinical relevance of cytochrome P450 polymorphisms. Aliment Pharmacol Ther. 2007;26:211-9. [ Links ]
30. Johnson J, Cavallari L. Pharmacogenetics and cardiovascular disease-implications for personalized medicine. Pharmacol Rev. 2013;65:987-1009. [ Links ]
31. Duke Medicine. 2011. Personalized medicine. En: USA News, publicado el 20 de enero de 2011. Disponible en: Disponible en: http://health.usnews.com/health-conditions/cancer/personalized-medicine . [ Links ]
32. Lee YH, Bae SC. Associations between PTPRC rs10919563 A/G and FCGR2A R131H polymorphisms and responsiveness to TNF blockers in rheumatoid arthritis: A meta-analysis. Rheumatol Int. 2016;36:837-44, https://doi.org/10.1007/s00296-016-3476-5. Epub 2016 Apr 13. PMID: 27074847. [ Links ]
33. Sode J, Vogel U, Bank S, Andersen PS, Hetland ML, Locht H, et al. Genetic variations in pattern recognition receptor loci are associated with anti-TNF response in patients with rheumatoid arthritis. PLoS One. 2015;10:e0139781, https://doi.org/10.1371/journal.pone.0139781. [ Links ]
34. Montes A, Pérez-Pampin E, Narváez J, Cañete JD, Navarro-Sarabia F, Moreira V, et al. Association of FCGR2A with the response to infliximab treatment of patients with rheumatoid arthritis. Pharmacogenet Genomics. 2014;24:238-45, https://doi.org/10.1097/FPC.0000000000000042. [ Links ]
35. Dávila-Fajardo CL, Márquez A, Pascual-Salcedo D, Moreno Ramos MJ, García-Portales R, Magro C, et al. Confirmation of -174G/C interleukin-6 gene promoter polymorphism as a genetic marker predicting antitumor necrosis factor treatment outcome. Pharmacogenet Genomics . 2014;24:1-5, https://doi.org/10.1097/FPC.0000000000000013. [ Links ]
36. Morales-Lara MJ, Cañete JD, Torres-Moreno D, Hernández MV, Pedrero F, Celis R, et al. Effects of polymorphisms in TRAILR1 and TNFR1A on the response to anti-TNF therapies in patients with rheumatoid and psoriatic arthritis. Joint Bone Spine. 2012;79:591-6, https://doi.org/10.1016/j.jbspin.2012.02.003. [ Links ]
37. Honne K, Hallgrímsdóttir I, Wu C, Sebro R, Jewell NP, Sakurai T, et al. A longitudinal genome-wide association study of anti-tumor necrosis factor response among Japanese patients with rheumatoid arthritis. Arthritis Res Ther. 2016;18:12, https://doi.org/10.1186/s13075-016-0920-6. [ Links ]
38. Canhão H, Rodrigues AM, Santos MJ, Carmona-Fernandes D, Bettencourt BF, Cui J, et al. TRAF1/C5 but not PTPRC variants are potential predictors of rheumatoid arthritis response to anti-tumor necrosis factor therapy. Biomed Res Int. 2015;2015:490295, https://doi.org/10.1155/2015/490295. [ Links ]
39. Montes A, Perez-Pampin E, Joven B, Carreira P, Fernández-Nebro A, Ordóñez MC, et al. FCGR polymorphisms in the treatment of rheumatoid arthritis with Fc-containing TNF inhibitors. Pharmacogenomics . 2015;16:333-45, https://doi.org/10.2217/pgs.14.175. [ Links ]
40. Morales-Lara MJ, Cañete JD, Torres-Moreno D, Hernández MV, Pedrero F, Celis R, et al. Effects of polymorphisms in TRAILR1 and TNFR1A on the response to anti-TNF therapies in patients with rheumatoid and psoriatic arthritis. Joint Bone Spine . 2012;79:591-6, https://doi.org/10.1016/j.jbspin.2012.02.003. [ Links ]
41. Muralidharan N, Mariaselvam CM, Jain VK, Gulati R, Negi VS. ATIC 347C>G gene polymorphism may be associated with methotrexate-induced adverse events in south Indian Tamil rheumatoid arthritis. Pharmacogenomics . 2016;17:241-8, https://doi.org/10.2217/pgs.15.170. [ Links ]
42. Salazar J, Moya P, Altés A, Díaz-Torné C, Casademont J, Cerdà-Gabaroi D, et al. Polymorphisms in genes involved in the mechanism of action of methotrexate: are they associated with outcome in rheumatoid arthritis patients? Pharmacogenomics . 2014;15:1079-90, https://doi.org/10.2217/pgs.14.67. [ Links ]
43. Moya P, Salazar J, Arranz MJ, Díaz-Torné C, del Río E, Casademont J, et al. Methotrexate pharmacokinetic genetic variants are associated with outcome in rheumatoid arthritis patients. Pharmacogenomics . 2016;17:25-9, https://doi.org/10.2217/pgs.15.150. [ Links ]
44. Lee YH, Bae SC, Song GG. Association of the ABCB1 C3435T polymorphism with responsiveness to and toxicity of DMARDs in rheumatoid arthritis: A meta-analysis. Z Rheumatol. 2016;75:707-15, https://doi.org/10.1007/s00393-015-1618-x. [ Links ]
45. Ghodke-Puranik Y, Puranik AS, Shintre P, Joshi K, Patwardhan B, Lamba J, et al. Folate metabolic pathway single nucleotide polymorphisms: A predictive pharmacogenetic marker of methotrexate response in Indian (Asian) patients with rheumatoid arthritis. Pharmacogenomics . 2015;16:2019-34, https://doi.org/10.2217/pgs.15.145. [ Links ]
46. Uribarri M, Ruiz-Larrañaga O, Arteta D, Hernández L, Alcaro MC, Martínez A, et al. Influence of MTHFR C677T polymorphism on methotrexate monotherapy discontinuation in rheumatoid arthritis patients: Results from the GAPAID European project. Clin Exp Rheumatol. 2015;33:699-705. [ Links ]
47. Chaabane S, Marzouk S, Akrout R, ben Hamad M, Achour Y, Rebai A, et al. Genetic determinants of methotrexate toxicity in Tunisian patients with rheumatoid arthritis: A study of polymorphisms involved in the MTX metabolic pathway. Eur J Drug Metab Pharmacokinet. 2016;41:385-93, https://doi.org/10.1007/s13318-015-0288-z. [ Links ]
48. Lima A, Bernardes M, Azevedo R, Medeiros R, Seabra V. Pharmacogenomics of methotrexate membrane transport pathway: Can clinical response to methotrexate in rheumatoid arthritis be predicted? Int J Mol Sci. 2015;16:13760-80, https://doi.org/10.3390/ijms160613760. [ Links ]
49. Muralidharan N, Antony PT, Jain VK, Mariaselvam CM, Negi VS. Multidrug resistance 1 (MDR1) 3435C>T gene polymorphism influences the clinical phenotype and methotrexate-induced adverse events in South Indian Tamil rheumatoid arthritis. Eur J Clin Pharmacol. 2015;71:959-65, https://doi.org/10.1007/s00228-015-1885-0. [ Links ]
50. Lima A, Bernardes M, Azevedo R, Monteiro J, Sousa H, Medeiros R, et al. SLC19A1, SLC46A1 and SLCO1B1 polymorphisms as predictors of methotrexate-related toxicity in Portuguese rheumatoid arthritis patients. Toxicol Sci. 2014;142:196-209, https://doi.org/10.1093/toxsci/kfu162. [ Links ]
51. Samara SA, Irshaid YM, Mustafa KN. Association of MDR1 C3435T and RFC1 G80A polymorphisms with methotrexate toxicity and response in Jordanian rheumatoid arthritis patients. Int J Clin Pharmacol Ther. 2014;52:746-55, https://doi.org/10.5414/CP202098. [ Links ]
✩ Please cite this article as: Puentes Osorio Y, Amariles Muñoz P, Aristizábal Bernal BH, Pinto Peñaranda LF, Calleja Hernández MÁ. Farmacogenómica de etanercept, infliximab, adalimumab y metotrexato en artritis reumatoide. Revisión estructurada. Rev Colomb Reumatol. 2018;25:22-37.
Received: February 14, 2017; Accepted: August 08, 2017; Rev-request: December 06, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
