











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Capillaroscopy is a simple, non-invasive microscopy method that allows a morphological evaluation of the vascular bed in a qualitative and semi-quantitative manner in different areas of the body in order to detect abnormal patterns. This method facilitates the diagnosis of some autoimmune diseases. In some cases, it offers information about the degree of activity and severity of the disorder.1,2
There are three types of systemic scleroderma, defined by the tissues affected in the disease. First, there is the limited cutaneous systemic scleroderma, which has a skin involvement limited to the hands, face, feet and forearms. It has a nailfold capillary pattern typical of scleroderma predominantly with nailfold capillary loops and capillary dropout. The common features of the condition are: calcinosis, Raynaud's phenomenon, esophageal motility dysfunction, sclerodactyly, and telangiectasia. Renal disease rarely occurs and the blood tests show a high incidence of anticentromere antibodies (ACA) in 50-60%.
Second, diffuse cutaneous scleroderma is a subtype characterized by truncal and acral skin involvement with tendon friction rubs. The nailfold capillary pattern typical of scleroderma has dilatation (early), dilatation and dropout (active), and tortuosity with dropout (late). The disease usually manifests itself in people between 40 and 50 years of age. Pulmonary fibrosis is frequently seen (60% of cases) and pulmonary hypertension may also occur in 10-15% of cases. Significant incidence of renal, interstitial lung, diffuse gastrointestinal, and myocardial disease occurs earlier than in other types of the condition and blood tests show Anti-Scl-70 in 30-40% of cases and anti-RNA polymerase I, II, or III antibodies in 12-15%. In the third type of systemic scleroderma, called systemic sclerosis sine scleroderma there is not skin involvement. Fibrosis affects one or more internal organs and antinuclear antibodies (anti-Scl-70, ACA, or anti-RNA polymerase I, II, or III) may be present in the laboratory tests.
In the case of Systemic Sclerosis (SS), it has been concluded that 90-95% of patients develop peripheral microangiopathy that is followed by a typical scleroderma pattern, which can be characterized as early, active and late. In the early pattern, the presence of isolated mega-capillaries is observed, with relative preservation of the distribution of the capillaries in the nail bed and scarce microhemorrhages without evidence of capillary loss.3 The active pattern highlights the presence of mega-capillaries, microhemorrhages, moderate loss of capillaries, and slight disorganization of the capillary structure with the presence of edema without branched capillaries or neoangiogenesis. Finally, the late pattern is characterized by irregular thickening of capillaries, irregular capillary dilatation, avascular areas, disorganization of the capillary structure, and aberrant neoangiogenesis of ramified or bushy capillaries with few or no megacapillaries.4
It is believed that the progression from early to active stage and from early to late stage is 28±20 months and 36±29 months, respectively. It is currently clear that these patterns are useful in the diagnosis and monitoring of systemic sclerosis.21 Therefore, capillaroscopy has been included within the diagnostic criteria of 2013, by the American College of Rheumatology.5
Capillaroscopy has also been used as a predictor of organ involvement in SS, including the development of skin ulcers. The Risk Index of Ulceration in Systemic Sclerosis (CSURI) assesses the risk of developing a digital ulcer in the next 3 months when the score obtained is higher than 2.96, with an area under the curve of 0.884 (95% CI: 0.835-0.922), a specificity of 81.4% and a sensitivity of 92.9%.6,7
Likewise, it has been found that capillaroscopy allows the detection of patients that will present organ involvement, with the development of pulmonary hypertension, interstitial lung disease, digital ulcers or esophageal, heart, and kidney involvement.8
Methods
This review was developed according to the Cochrane Handbook for Systematic Reviews of Interventions. Eligible studies were those that reported the relationship between the findings of capillaroscopy and the development of organ involvement in SS and the relation with different subtypes. Based on the PICOT strategy, eligibility criteria were defined by formulating inclusion and exclusion criteria within the literature.
Inclusion criteria
- Population: All studies conducted on patients over 18 years of age diagnosed with SS were considered eligible.
- Intervention: Studies that reported the usefulness of capillaroscopy in the prediction of organ involvement in patients diagnosed with SS.
- Comparison: It was not made.
- Study designs: Descriptive studies.
- Time: Publication dates limited between 2000 and 2019.
Information sources and search criteria
A systematic and exhaustive literature search was conducted in the following electronic databases: Medline Pubmed, Embase, Cochrane, and Lilacs. The research question was structured under the PICOT model, and a generic search strategy was designed based on the key terms "Microscopic Angioscopy," "Scleroderma systemic," "Scleroderma diffuse," Scleroderma Limited," "Early Diagnosis". The search strategy used MeSH terms with Boolean operators and was restricted to Spanish and English languages, with publication dates between 2000 and 2019.
Studies selection
The references were assessed by two independent reviewers (DL AND JL) based on titles and abstracts, applying the eligibility criteria. The articles that met those criteria were selected. In case there were disagreements between the peer reviewers, a discussion and verification of the information was carried out with the full texts of the articles in which there was assurance about compliance with the inclusion criteria, resolving the discrepancies by consensus. Finally, the results were summarized using the PRISMA flow chart.
Data selection and summary of selected studies
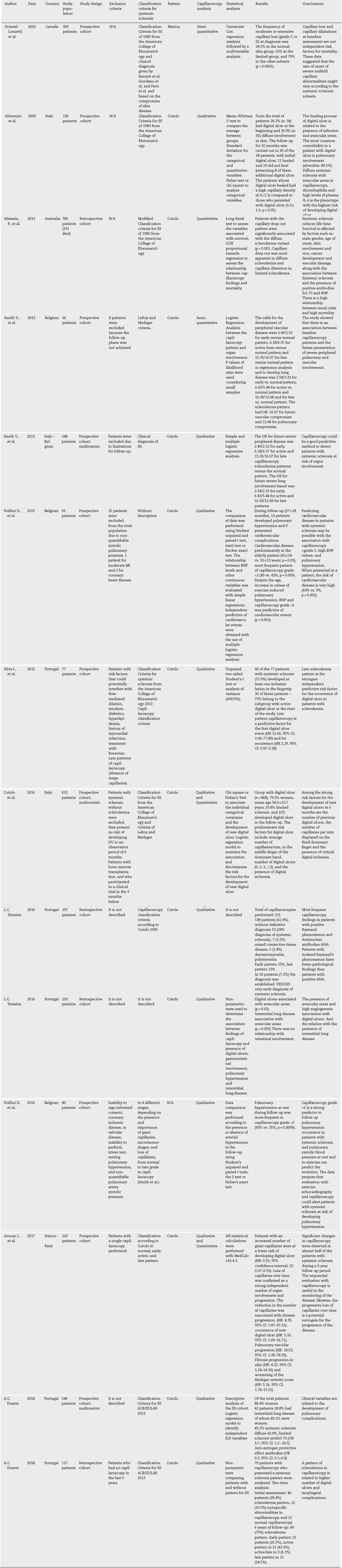
The data selection was carried out independently by two reviewers (DL and JL), based on what was reported in the original publications, the characteristics of each study and its results. The information was organized in a standard Microsoft Excel 2011 format. The data extracted included author, year, location, sample size, study design, exclusion criteria, classification criteria used in SS, results, population percentages for the limited, diffuse and Very Early Diagnosis of Systemic Sclerosis (VEDOSS) samples, and conclusions. With the extracted information, a summary table of evidence was constructed. (Table 1)
Risk of bias assessment
It was performed independently by the two authors (DL and JL) using the Cochrane QUIPS tool to assess the risk of bias of the clinical trials. All the articles were evaluated by the two researchers, and by common agreement, the risks of bias were established (Table 2).
Table 2
| Articles | Year | Selection bias | Desertion bias | Measurement bias | Assessment bias | Confounding factors | Bias in relation to analysis and statistical reports | |
|---|---|---|---|---|---|---|---|---|
| 1 | Scussel-Lonzetti et al. | 2002 | High | Low | Low | Unclear | Low | No |
| 2 | Alivernini et al. | 2009 | Low | Low | High | Moderate | Low | High |
| 3 | Hissaria P., et al. | 2011 | Low | Low | Low | Low | High | Moderate |
| 4 | Smith V., et al. | 2012 | Low | Low | Low | Low | High | Moderate |
| 5 | Smith V., et al. | 2013 | Moderate | Moderate | Low | Low | Low | Moderate |
| 6 | Voilliot D., et al. | 2015 | Moderate | Low | Moderate | Low | High | Moderate |
| 7 | Silva I., et al. | 2015 | Low | Low | Moderate | Low | Moderate | Low |
| 8 | Cutolo et al. | 2016 | Moderate | Low | Low | Moderate | Low | Low |
| 9 | L.C. Teixeira | 2016 | Moderate | Moderate | Moderate | Moderate | Moderate | High |
| 10 | L.C. Teixeira | 2016 | Moderate | Moderate | Moderate | Moderate | Moderate | High |
| 11 | Voilliot D., et al. | 2016 | Moderate | Moderate | Moderate | Low | High | Moderate |
| 12 | Avouac J., et al. | 2017 | Low | Low | Low | Low | Low | Low |
| 13 | A.C. Duarte | 2018 | Moderate | Moderate | Moderate | Moderate | Moderate | Moderate |
| 14 | A.C. Duarte | 2018 | Moderate | Moderate | Moderate | Moderate | Moderate | Moderate |
Results
The search was carried out independently by each of the researchers. The databases used by each researcher were randomly assigned. A total of 138 articles were found in the selected databases: Medline (n: 115), Embase (n: 66), Cochrane (n: 2), Lilacs (n: 0). After carrying out the removal of articles by title and abstract, a total of 66 items were obtained. For these articles, a screening process was carried out based on the title and the abstract, taking into account the eligibility criteria, obtaining 21 references. Both researchers assessed the selected articles (full text), and all disagreements were solved by a consensus decision. Finally, a total of 14 articles were included. The majority of studies (11/14, 78%) reported associations between baseline capillaroscopic features (using qualitative, semi-quantitative and quantitative endpoints) and organ involvement including digital ulcers occurrence, progression of skin lesions, pulmonary arterial hypertension, interstitial lung disease, esophageal complications and analysis of cardiovascular risk. Among them (2/14, 14.2%) found a progressive loss of capillaries as a potential surrogate for the progression of the disease; and (2/14,14.2%) considered a relationship with mortality (Fig. 1).

Studies description
Most of the studies were conducted in Italy (n: 6), Portugal (n: 5) and Belgium (n: 4), one of them being the product of a collaboration between two of these countries: Belgium and Italy. Regarding the research group, Sebastiani et al., Smith V., et al. and L.C. Teixeira and collaborators, conducted the majority of these studies. The other publications were made by researchers in Spain, Australia, France, Brazil and Canada. Regarding the publication year, the articles were published between 2002 and 2018. The included references were primary studies with diagnostic validity in men and women in adulthood, and no studies conducted in Colombia were identified. The study sample sizes varied between 40 and 786 patients.
The majority of the studies were prospective cohorts and the criteria used for the classification of SS were those of the American College of Rheumatology of 1980, Criteria of Le Roy and Medsger, Criteria of Classification for ES ACR/EULAR 2013 and Cutolo's criteria.
In several articles, scleroderma patterns were associated with multisystemic involvement, including the kidneys, scleroderma "renal crisis"; heart, cardiomyopathy, symptomatic pericarditis, or arrhythmia; lungs, pulmonary fibrosis; GI tract, malabsorption, skin, digital ulcers, and vascular complications and their respective clinical manifestations, as in the case of pulmonary hypertension which is one of the most common complications in patients with SS. Voilliot et al.9 found that capillaroscopy grade >2 according to the LeRoy and Medsger criteria (semi-quantitative method on the report of Cutolo's criteria) is a strong predictor of the development of pulmonary hypertension in patients with SS; pulmonary systolic blood pressure at rest and during exercise could be helpful measures to predict its evolution. The data show that evaluation with exercise echocardiography and capillaroscopy could alert patients with SS who are at risk of developing pulmonary hypertension.
In 2012, Smith et al.10 conducted a prospective cohort study in Belgium, in which they found an association between baseline capillaroscopy patterns and the future development of pulmonary (p: 0.003) and severe peripheral vascular (p: 0.001) involvement. An initial patient evaluation was made and images described as normal, early, active and late pattern were obtained. Subsequently, a second measurement was made in a period between 18 and 24 months, in which they found a relationship between the progression of severity at the pulmonary level and the presence of digital ulcers, although it was not predictive. In this study, the baseline clinical data were not described. Therefore, it was not possible to confirm if a variation of clinical characteristics occurs during the period between measurements.
Silva and Collaborators11 found that among scleroderma patterns, the late pattern was the strongest independent predictive risk factor for the occurrence of digital ulcers for the first event and subsequent events in patients with SS (HR: 12.66,95% CI: 2.06-77.89 and HR: 2.29,95% CI: 0.97-5.38). In this study, smokers, diabetic patients with hyperlipidemia, history of myocardial infarction and patients on Bosentan treatment, who might have risk factors that could potentially interfere with flow-mediated dilation or could skew the findings of capillaroscopy, were excluded from the study. The most important limitation was not having the number of fingers that were evaluated and the description of the images obtained.
Cutolo and colleagues12 described other findings related to the development of new digital ulcers at 6 months. Among these are the number of previous digital ulcers, the number of capillaries per millimeter displayed on the 3rd finger of the dominant hand, and the presence of critical digital ischemia, which were considered strong risk factors for recurrence.
Furthermore, Avouac et al.13 found in a 3-year prospective cohort study, that progressive loss of capillaries over time is a finding related to disease progression (HR: 4.35, 95% CI: 1.87-10.12), organ involvement, occurrence of new digital ulcers (HR: 5.33, 95% CI: 1.69-16.71), pulmonary vascular progression (HR: 18.53, 95% CI: 1.28-78.33) and progression of skin fibrosis (HR: 4.22,95% CI: 1.24-14.36) so the capillaroscopy, would be considered a useful method for monitoring it.
Regarding the healing of digital ulcers, Alivermini14 found a relationship between the presence of greater avascular areas and a longer duration of lesions, apparently related to the microangiopathic damage caused by the disease. Additionally, he reported as direct risk factors for the development of digital ulcers: the simultaneous presence of diffuse sclerosis, avascular areas, thrombophilia and high levels of IL-6. The most common comorbidity found in this study was pulmonary alveolitis in 89.5% of the patients.
Hissaria15 in 2011, conducted a retrospective study for 14 years with 786 patients and described the relationship between various subtypes of scleroderma compromise and systemic complications. The most common were scleroderma renal crisis, pulmonary arterial hypertension and pulmonary fibrosis with a high impact on survival rates. A relationship between capillaroscopy patterns and mortality was also reported (95% CI: 1.06-2.42); however, it was not clear whether the analysis was adjusted for the presence of diffuse scleroderma, interstitial lung disease or the presence of anti-Scl-70 autoantibodies, as each of them has been independently related to mortality in other studies.
Reported prognostic associations of NVC in subtypes identification
Findings regarding systemic complications and classification by subtype have been described. In 2002, Scoussel-Lonzetti1 in a prospective study with 309 patients being studied for 15 years, described the correlation between different rates of capillary loss and the subtype found. Thus, after 2.5 years of initial symptoms of SS, 75% of patients presenting with diffuse pattern had already presented severe capillary loss, in contrast with 40% and 15% in the intermediate and limited subtypes, respectively.
Smith et al., established16 the association between findings in capillaroscopy and different findings in systemic sclerosis, (early, active and late), with organ involvement in 2 independent cohorts. As for the Belgian cohort, 25/55 patients (45%) had severe involvement of any of the organs of the nine systems. This study showed a statistically significant association between the NVC pattern and the involvement of some of the organs. The estimated OR after the simple and multiple logistic regression analysis, showed that organ involvement was stronger in those patients in whom the NVC patterns were more severe. These findings were similar to those found in the Italian cohort, in which 31/79 patients (39%) had any of the nine organs affected.
L.C. Teixeira, in two different studies17,18 revealed the association between stages and organ involvement. The first study was conducted from January 2013 to December 2015. Capillaroscopy was considered abnormal in 79.4% of patients with positive Raynaud's phenomenon and ANA, and 41.2% had specific findings of rheumatic disease, suggesting that this combination is associated with a higher disease incidence. Patients with isolated rheumatoid factor had less pathologic capillaroscopy findings than those with isolated ANA positivity. Similarly, in patients with SS, the late and early patterns were the most frequent in capillaroscopy.
The other study showed that the presence of avascular areas and neo-angiogenesis in capillaroscopy was significantly associated with the existence of digital ulcers. Also, interstitial lung disease and higher values of NT-proBNP were more common in patients who presented avascular areas. These results suggest that abnormalities detected in the capillaroscopy might help predict organ involvement.
Duarte,19 in Portugal, analyzed 146 patients of which 42 developed interstitial disease, identifying results of capillaroscopic findings in 23 of them; 21 presented a pattern for SS at different stages (5 early, 6 active and 10 late). In addition, in a multivariate analysis, the presence of anti-Scl70 (OR: 3.7, 95% CI: 1.3-10.5) and digital ulcers (OR: 2.2,95% CI: 1.9-5.3) was associated with the development of pulmonary interstitial disease. Otherwise the presence of anti-centromere antibodies behaves as a protective factor (OR: 0.3, 95% CI: 0.1-0.8).
In a second retrospective cohort study, Duarte20 found that the scleroderma pattern was significantly associated with a higher number of digital ulcers and these patients had a higher prevalence of esophageal involvement. Scleroderma pattern was associated with the presence of digital ulcers (OR 1.49, 95% CI: 1.17-1.92).
This study demonstrates that nailfold capillaroscopy is useful for monitoring endothelial injury and potential vascular and systemic damage.
Discussion
This review identified an essential relationship between the evolution of capillary abnormalities and the progression of the disease in systemic sclerosis. The increase in capillary loss predicts more significant vascular and organic complications.
Once more, capillaroscopy seems to play a crucial role in early identification and as a follow-up tool in patients with systemic sclerosis. It is also useful as a method for predicting secondary complications, as it was observed with the development of digital ulcers, pulmonary hypertension, and other vascular complications.
The results from the studies included were similar over time without finding significant differences between the data obtained in each of them.
These results support why this diagnostic method has been included within the diagnostic criteria of the American College of Rheumatology of 2013 and reflect its importance as an economical, reproducible and non-invasive technique reinforcing the need for its incorporation as a prognostic factor for disease progression.
Capillaroscopy follow-up directions
In patients with autoimmune disease (mainly systemic sclerosis) and Raynaud's phenomenon that remains active, it is important to perform video-capillaroscopic monitoring every 3-6 months to verify the evolution and changes derived from treatment, and which in turn determines the need for optimize vasodilator and/or immunomodulator treatment.
In patients with autoimmune disease and Raynaud's phenomenon who have had adequate control in the frequency and intensity of attacks, annual video-capillaroscopic control is indicated.
Study limitations
There are several limitations in the present study:
The wide heterogeneity of the primary studies (which in turn prevents the meta-analysis of the studies), about the follow-up time after the symptoms appear (mainly the Raynaud's phenomenon), the temporality of the studies (retrospective, mostly cross-sectional and small prospective), and the lack of unification of the evaluation criteria for the findings of abnormality in the capillaries.
Lack of standardization in the procedure (not explained) and the process of concordance between the observers to verify the confirmation of the results.
Being a predominantly semi-quantitative method, it lends itself to classification biases and diagnostic error.
The overlapping of the findings in various autoimmune conditions, including in some healthy patients (moderate performance of the technique).
In daily clinical practice, capillaroscopy is useful not only for confirming the diagnosis of systemic sclerosis but also for monitoring endothelial injury, potential macrovascular systemic damage, and cardiovascular risk. However, more studies are required to determine its real predictive value.

