











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Osteoarticular manifestations (OAM) are frequently present in patients with systemic sclerosis (SSc) with a reported prevalence between 40-80 % of cases.1,2 These OAM are related to important functional disability and a severe impact on patient's life quality. Clements et al. previously alerted on the knowledge gap regarding OAM in SSc and the need to further investigate this issue.3
During the past few years the importance of OAM in SSc has grown, increasing the number of published literature regarding this topic. Given the amount of new information available, we decided to do a systematic review of the literature with the purpose of determining the frequency of reported OAM in SSc patients, the general impact of OAM in patient's condition and the tools available for diagnosis and treatment
Methodology
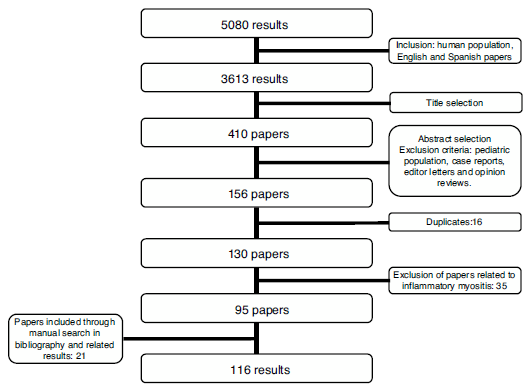
A systematic review of the literature was performed for information published between January 1970 and December 2018. The search strategy was conducted in the medical research databases of: Medline, Embase, Lilacs, Scielo, Cochrane and clinicaltrials.gov. The terms used were: Scleroderma, Systemic,- "CREST syndrome", "scleroderma", "SSc", "systemic sclerosis", Joint diseases-,, Musculoskeletal Diseases-,- and "arthritis" (Supplementary material, Table S1) Search was limited by language to English and Spanish, and only articles regarding humans were included. The search included articles discussing research design, cohort, case control, and cross-sectional studies according to the objective of the review. Exclusion criteria considered were: pediatric population, individual case reports, genetic studies, narrative reviews, editor letters and opinion papers. Initially, 3613 articles were screened by title content, afterwards, two independent researchers reviewed the papers based on their abstracts. Duplicates were discarded (Fig. 1). In case of disagreement regarding the inclusion of an article, the article was reviewed by the two researchers. In case that no consensus was achieved the decision was made by the senior researcher. The first phase resulted in 130 articles to be selected by full text research (Fig. 1). After reading the studies related to musculoskeletal manifestations (21 articles), we considered that an independent systematic review focused on these manifestations should be performed. For this reason, we excluded these articles from the current revision. Fourteen additional articles were excluded based on their content (Table S2). Twenty-one papers were included after reviewing related articles and bibliography. Thus, a total of 116 articles were included (Table 1) in the present review. The information to be included was extracted independently by two independent researchers. In case of disagreement, the same methodology was used as in the selection of studies. The bias risk assessment was performed by two independent researchers (Table S3-S6).

Results
SSc can have different levels of OAM affecting directly articular units or their adjacent tissue (Table 2). OAM are more frequently seen in the diffuse variety of SSc and their development is related to severity biomarkers of vascular, muscular and pulmonary compromise.2,4
Inflammatory articular manifestations
Arthritis and synovitis are frequent manifestations during the course of the disease. Literature reports 9-70 % of OAM among patients with similar early and late disease stages2,4-11 (Fig. 2). The most frequent manifestation is mild arthritis with small and discrete erosions.11-13 However, the presence of erosive arthritis similar to that seen in rheumatoid arthritis (RA) patients has been reported (Fig. 3); which opens the debate regarding the presence of a clinical overlap between RA and SSc or an isolated manifestation of the latter.11,14,15 Overlap is highly suspected in patients who develop articular manifestations and Raynaud's phenomenon.16 Monoarthritis, oligoarthritis or polyarticular involvement17 are more frequently seen in diffuse SSc compared to the limited variety,2 although some studies report that deforming arthritis manifestations are more prevalent in SSc limited variety.11 OAM are also related to acute phase reactants with an OR of 2.1 (95 % CI 1.67-2.64).2 Furthermore, the presence of arthritis is a predictive factor for: general disease progression, reduced left ventricular function, development of digital ulcers and worsening in Rodnan score18; thus making it a highly valuable severity feature to evaluate in all SSc patients.18 Sacroiliac joint manifestations are not unusual, and the presence of high C-reactive protein (CRP) level or back pain should alert the clinician for the possibility of sacroiliitis.19

Fig. 2 Detection of inflammatory joint and tendon involvement with MRI (arrows). Adapted (with permission) from Avouac et al.1
Joint contractures
Joint contractures are very frequent during the course of the disease with a prevalence of 30-80 % in all patients throughout all disease stages.2,4,9,10,20-22 The articular units involved are mainly the first and second metacarpophalangeal (MCP) joints with damage described in up to 82 % of patients with joint contracture. The involvement of wrists, shoulders and second and third proximal interphalangeal (PIP) joints is usually described20 (Fig. 4), while the hips, knees and elbows are seldom involved. Patients with: diffuse SSc, positive titers for anti-topoisomerase I, and pulmonary, cardiac and esophageal involvement are more prone to joint contractures.2,7,20,21 Additionally, the diffuse SSc variety is an independent predictor for contracture progression.23 Also, it has been described that patients with more than four joints involved per hand have a lower survival rate, thus, articular contractures can be interpreted as a disease severity marker.20

Fig. 3 Erosive radiographic arthritis characterized by erosions and joint space narrowing involving the PIP and DIP joints (arrows). Adapted (with permission) from: Avouac et al.1

Fig. 4 Flexion contracture involving the hands. Adapted (with permission) from Tas et al.27Tendon friction rubs (TFR)
TFR also appear in patients with SSc with a reported prevalence of 5-37 %, ocurring more often in patients with diffuse SSc.2,4,10,22,24 TFR manifest mainly in hands, elbows and ankles.24,25 They are found more frequently in young patients and during early stages of the disease (OR 2.58, 95 % CI 1.87-3.56), and their presence is related to a progression of the disease, and other severe manifestations such as pulmonary, renal and vascular compromise.2,18,24,26 Additionally, patients with early diffuse SSc who develop TFR have a lower five to ten-year survival, and more severe compromise of their life quality.24
In general, synovitis, articular contractures and TFR manifest together, thus, the presence of any one of the OAM is a risk factor for the development of other osteoarticular involvement.2
Acroosteolysis
Distal phalanges bone resorption, or acroosteolysis, is another usual OAM, seen in up to 25 % of patients27 (Fig. 5). Some studies have described this manifestation related to more severe and systemic compromise of SSc.28 Furthermore, acroosteolysis is associated with digital ischemia severity,29,30 as well as with the presence of advanced videocapillaroscopy patterns, particularly capillary loss and angiogenesis.31 Similarly, the presence of digital ulcers is an independent predictor for acroosteolysis progression.23 Thus, distal bone resorption may correspond to an ischemic manifestation of SSc.
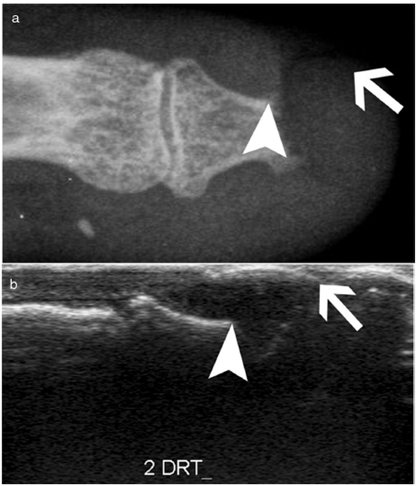
Fig. 5 Acroosteolysis of the index finger in a SSc patient. a. plain radiograph imaging. b. ultrasonography imaging. Adapted (with permission) from: Freire et al.73
Calcinosis
Calcinosis, which has been described in up to 25 % of patients, is more frequently described in older patients and is related to the presence of osteoporosis and digital ulcers32,33 (Fig. 6). Additionally, digital ulcers are an independent progression factor for calcinosis.23 Some studies suggest a possible role for vascular damage in the pathogenesis of calcinosis since it is associated to advanced videocapillaroscopy patterns and digital ulcers.31
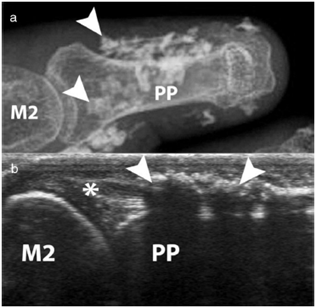
Fig. 6 Calcinosis of the index finger in a SSc patient. a. plain radiograph imaging. b. ultrasonography imaging. Adapted (with permission) from: Freire et al.73
Avascular necrosis
Avascular necrosis in the femoral head has been reported as an infrequent OAM, although severe, in SSc patients. In early stages of the disease the patients maybe asymptomatic. However, as it progresses the cardinal symptom is pain in the groin, thigh and buttocks.35 Some rare cases involving the carpal bones have been reported, yet necrosis of the lunate bone might be underestimated and frequently misinterpreted as carpitis (erosive arthritis in the wrist).36,37
Feet involvement
Osteoarticular manifestations in the feet tend to appear later in the disease course and cause severe disability. At the time of SSc diagnosis, articular contractures, TFR and acroosteolysis involvement of the feet are far less common than these of the hands; nonetheless, feet arthralgia might be a common complaint.34 Moreover, feet involvement worsens during the course of the disease unlike hand involvement which tends to remain steady once it is manifested.34
Bone mineral density in SSc
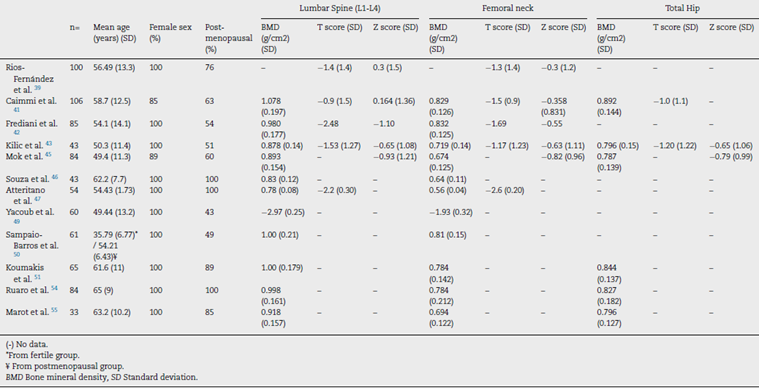
SSc patients have multiple known risk factors for the development of osteoporosis, i.e., chronic inflammation, steroids use, immobility and early menopause.38 Low bone mineral density (BMD) has been reported in around 27 %-62 % of SSc patients,38-45 while osteoporosis has been reported varying between 10 %-51 % of patients depending on the studied populations41-48 (Table 3). In SSc patients low BMD is more frequently seen in the femoral neck compared to the lumbar spine (0.829 + 0.126mg/cm2 vs. 1.078 + 0.197mg/cm2).41 The change in BMD seems to be influenced by the lower body mass index reported in this patients group compared to normal population.41,42,46
In a study in Moroccan population by Yacoub et al. the SSc population had a lower BMD, as well as lower vitamin D levels compared to healthy controls. In addition, there was an association between a low BMD and low vitamin D levels with the presence of severe joint involvement.49 Similarly, in two Spanish populations the presence of SSc and the longer duration of the disease were associated with a lower BMD when compared with a group of healthy women. However, vitamin D deficiency was not associated with lower BMD.39
Similar results were found in the femoral neck bone density in a group of 43 patients with SSc when compared with matched controls with RA43; however, a previous study with a larger number of patients did not find this difference.44 The cumulative dose of steroids is not a risk factor for the development of osteoporosis or fractures in SSc when evaluated with bone densitometry44,50; although patients receiving doses of prednisone of 5 mg or more per day have an altered bone microarchitecture when evaluated by tomography.51 In a prospective study of 50 Canadian SSc patients, those who were non-Caucasian had a lower BMD than Caucasians.40 The presence of calcinosis seems also to influence the appearance of osteoporosis32; nonetheless, this finding is not reproducible in all series.52 A low BMD in SSc patients is not associated with the severity of involvement of other organs.45
The presence of fragility fractures is not negligible. Omair and colleagues reported fragility fractures in up to 14 % of patients.40 In a previous study, up to 24 % of patients had a documented vertebral fracture, with a predominance of grade 1 fractures in the Genant classification.47 Avouac et al. found that 35 % had fragility fractures in a cohort of 71 patients with SSc, the number of fractures was similar to that found in patients with RA, and was higher than the reported in other SSc cohorts, probably due to the older age of patients in this cohort.44
Fauny et al. found that despite the increased risk of bone mineral density alteration, only 43 % of SSc patients are screened with Dual Energy X-ray Absorptiometry (DEXA).53 In addition, there are complementary strategies applied to tomography that allow to determine fracture risk in SSc patients, which seem to be more sensitive than DEXA in this specific population.53 The Trabecular Bone Score (TBS), a recent tool to evaluate bone microarchitecture, has been used in patients with SSc with good results.51,54 Ruaro et al. reported TBS as capable of discriminating patients with altered bone microstructure that increases the risk for fracture.54 In addition, TBS appears to be more altered in patients with early or active videocapillaroscopy patterns, suggesting a correlation between microvascular damage and bone involvement.54 In a previous study by Marot et al. an important compromise of trabecular bone was found, which seems to be related to the presence of digital ulcers.55 Bone microstructural characterization through TBS opens the possibility to its potential use as a complementary diagnostic tool for bone involvement secondary to corticosteroids, thus TBS could be used with DEXA to detect osteoporosis induced by corticosteroids.51
Serological markers
Anti-cyclic citrullinated peptide antibodies (anti-CCP) Several studies have looked at the relationship of anti-CCP with the development of joint manifestations in SSc. Anti-CCP positivity is reported in between 3 %-14 % of SSc patients according to the test generation and the cut-off point used.56-59 In Latin American population anti-CCP positivity has been described in up to 12 % of cases with SSc, however, their association with arthritis in this demographic group is not completely clear.56 Due to the high specificity of these antibodies for RA diagnosis, there is controversy regarding the usefulness of anti-CCP to diagnose the overlap of SSc with RA (SSc-RA). Santiago et al. found a significant association between positive titers of anti-CCP and the onset of arthritis, although there was no statistically significant association between the presence of these antibodies and the diagnosis of SSc-RA58; unlike other studies where anti-CCP were considered useful for identifying SSc-RA patients.57,60,61 Stamenkovic et al. also reported a significant relationship between anti-CCP and clinically evident arthritis.59 Similarly, a recent study found that the presence of anti-CCP is related to the appearance of bone erosions, and when associated with the presence of positive rheumatoid factor (RF) is related to the development of arthralgia in SSc patients.62 A meta-analysis by Laustriat et al. reported that in addition to conferring high risk of erosive arthritis (OR = 22.48 [95 % CI: 10.71-47.21]), anti-CCP positivity in SSc patients increases the risk for pulmonary fibrosis, as well as for esophageal and diffuse skin involvements.63
Other antibodies
The presence of antinuclear and double-stranded DNA antibodies (ANA and anti-dsDNA, respectively) in limited SSc patients seems tobe related to joint manifestations.11,64 Antibodies against SCL-70 (anti SCL-70) are higher among patients with low BMD.39,40,41 In addition, an association of anti SCL-70 with the development of articular contractures and deformity in hands has been reported (OR 7.01, 95 % CI 1.02-48.69), although it is not associated with the presence of arthralgia, or TFR.21,65 There is some debate about whether the presence of anti-topoisomerase I antibodies is associated with the presence of joint manifestations, especially joint contractures, since some of the studies that have established this association have selection biases.66
Cartilage oligomeric matrix protein (COMP)
COMP, a protein found in cartilage, and believed to be an important regulator of collagen fibers type I and II maintenance, has been studied as a possible marker of arthritis in SSc. A study of 40 SSc patients found that COMP levels were related to disease activity, presence of arthritis, anti-CCP and anti SCL-70 antibodies.67 However, a significant number of patients show positive COMP, so it does not seem to be very specific to identify arthritis.67
Platelet-activating factor acetylhydrolase (PAF-AH)
Normal levels of PAF-AH correspond to a risk factor for arthralgia or arthritis (OR 19.8, [95 % CI 2.4-164] and OR 1.86, [95% CI 1.33-2.59] respectively), which suggests that the presence of elevated PAF-AH has a possible protective role for joint involvement.68
YKL-40 or human cartilage glycoprotein 39 (HC gp-39)
YKL-40 was evaluated in a study of 40 SSc patients by La Montagna et al. reporting that YKL-40 levels are elevated in patients with arthralgia or arthritis, which suggests that it can be a possible serological marker of joint involvement in SSc.69
Radiological evaluation
Conventional radiography
Conventional radiography is a useful tool to address joint involvement in SSc used in conjunction with RF and anti-CCP, especially in cases where doubt exists of a possible overlap with RA.27 The findings can be divided into three patterns: articular degenerative damage, periarticular fibrotic changes, or articular inflammatory involvement; although this is a classification that is not reproducible in all studies.9
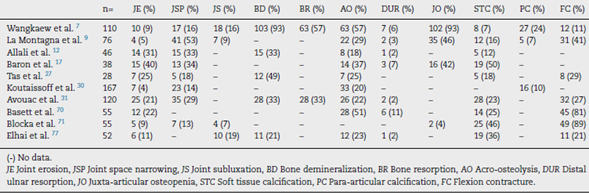
One of the most frequent findings described in simple X-rays is juxta-articular demineralization, reported in up to 42 % of cases with SSc. Decreased joint space and small and discrete joint erosions are common, up to 33 % and 31 % respectively12,27,33,70,71 (Fig. 7). Flexion deformities are present in a considerable number of patients.70 Extra-articular calcifications can appear in up to 18 % of cases12,27,30,33 (Table 4). Unlike RA, involvement of styloid process is uncommon, occurring only in 2 % of patients.12 In the distal phalangeal tuft (DPT) the most frequently described finding corresponds to DPT resorption reported in up to 28 % of the cases.12,30,70,72
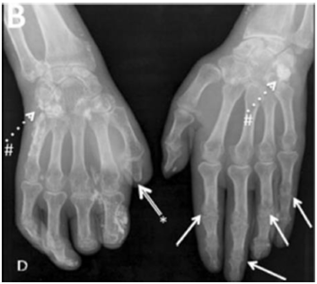
Fig. 7 Typical hand findings in simple radiography of a patient with SSc. (white arrow: yuxta articular erosions with joint space loss, asterix: acroosteolysis, hash: calcinosis). Adapted (with permission) from: Avouac et al.1

Fig. 8 A transverse ultrasonographic view of the common extensor tendon at the level of the wrist showing by grayscale tenosynovitis in the form of effusion (arrow). Adapted (with permission) from: Abdel-Magied et al.75
Other findings reported are calcinosis in up to 12 %,30 as well as DPT proliferation or erosions, although with less frequency.72 When feet radiographs are evaluated, there is a lower frequency of acroosteolysis, erosions and calcinosis compared to hands. However, there are no significant differences in dem-ineralization, decreased joint space, or joint subluxations.34
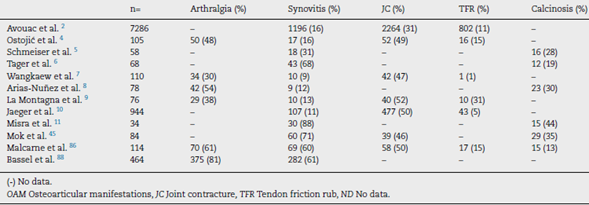
Ultrasonography (US)
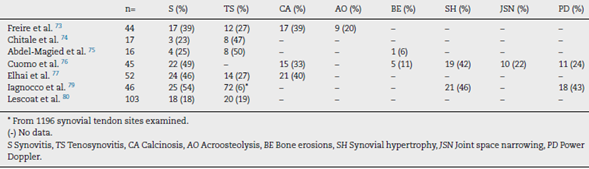
Due to the poor sensitivity of conventional radiography to detect early findings of joint involvement, the role of ultra-sonography in this scenario has been evaluated (Table 5). Freire et al. evaluated the US findings at the joint level in SSc patients with recent diagnosis.73 Synovitis was found in 39 % of patients, mostly mild. In addition, 27 % of patients presented tenosynovitis with greater involvement in extensor tendon sheaths than in flexors73 (Fig. 8). US is able to identify arthritis and tenosynovitis during the follow-up of the disease in SSc patients with arthralgias without clinically evident inflammatory changes, although it is not equally useful to identify erosions.74-76 Sclerosing tenosynovitis and soft tissue calcifications are specific findings of SSc that allow for differentiation from other pathologies such as RA.77 Likewise, US has an acceptable sensitivity to detect calcinosis and acroosteolysis, with a value of 89 % and 90 %, respectively,73 and is able to detect the presence of enthesopathy in SSc patients.78 Iagnocco et al. evaluated the prevalence of abnormal US findings combined with Power Doppler in carpal and hand joints from SSc patients.79 Similar to previously published studies, a high prevalence of abnormal findings was reported when compared to healthy population. The most frequent findings described were: synovial hypertrophy, joint effusion and tenosynovitis. In addition, the use of Power Doppler US improves the ability to recognize local inflammatory signs, often in the absence of clinically evident synovitis.79 Lescoat et al. in a recent study confirmed these results, reporting inflammatory synovitis in 17.5 % of patients, and sclerosing tenosynovitis in up to 18.5 %.80 These findings were associated with elevated CRP, clinically evident synovitis and pericarditis. In turn, sclerosing tenosynovitis was more frequently seen in men and was associated with pulmonary compromise, antibodies against RNA polymerase III, and diffuse type SSc.80

Magnetic resonance imaging (MRI)
Interest in MRI usefulness to detect joint involvement in SSc patients has increased in recent years. Synovitis with mild erosions and joint effusion associated with the presence of bone marrow edema are predominantly described (Table 6).81,82 Articular MRI is more sensitive than ultrasound to identify joint involvement in patients with arthralgia without clinically evident synovitis.74,75 Unlike US and radiography, MRI is able to identify early changes, especially at the level of the car pus with predominant involvement of the lunate bone, which seems to be a distinctive feature of the disease.81
MRI has a high yield to identify tenosynovitis involving the hands in patients with arthritis,83 as well as changes in SSc patients, in whom tenosynovitis is described in up to 88 % of those with arthralgia.74,75 Similarly, in patients with evidence of TFR, MRI identifies tenosynovitis in up to 50 % of cases.84
Clinimetry and impact on general functionality and quality of life
The quality of life of patients with SSc is affected at different levels,85 largely due to skin involvement86 and osteoarticular commitment that affects the development of daily activities in a moderate to severe degree.10,87,89 Moreover, psychological stress and the perception of disability negatively affect the quality of life in these patients.90 There are multiple factors that are associated with the loss of hand function, especially the presence of joint contractures, digital ulcers, and severe Raynaud's phenomenon.91
The Health Assessment Questionnaire (HAQ) disability index (DI), the Short Form 36 (SF-36) health survey physical component score (PCS) and the mental component score (MCS) have been validated in SSc.92 Wiese et al. documented that there is a correlation between the HAQ DI and SF36 PCS (r= -0.79), as well as between HAQDI and global health measurements given by physicians and patients with early diffuse SSc (r = 0.43 and r = 0.57, respectively).22 These measurements had an important association with the modified Rodnan score, although they did not have the same association with mus-culoskeletal manifestations or OAM.22 Additionally, using the same instruments, the disability generated by joint involvement is greater than that presented in PsA patients, with more intense pain than in RA patients.93 In a subsequent study of 326 patients with early diffuse SSc it was found that the loss of hand function, determined by the Cochin Hand Function Scale (CHFS), also contributes significantly to the disability generated by SSc.94
Kwakkenbos et al. validated in a cohort of 696 patients the PROMIS-29v2, a tool that evaluates seven domains related to quality of life in addition to the intensity of pain in SSc patients.89 They found that SSc negatively impacts quality of life largely due to joint contractures and gastrointestinal symptoms.89
The hand mobility test in SSc (HAMIS) was evaluated in a longitudinal study of 43 SSc patients with less than three years' duration of the disease.95 A follow-up of at least four years was carried out, reporting that, although it varied in 72 % of the patients, there were no significant changes in the mobility of the hand during the first years of the disease.95 In turn, in patients with longer duration of the disease, there is an important limitation to perform movements that involve handgrip or twisting.96 The delta finger-to-palm test has also been validated to evaluate the mobility of the hands in SSc patients,97 as well as the Michigan Hand Questionnaire (MHQ).98 Similarly, the hand anatomic index (HAI) corresponds to a useful tool to objectively assess hand deformity and secondary functional impairment in SSc patients.99
Erol et al., used the health-related quality of life (HRQoL) with the Duruöz Hand Index (DHI) to assess hand function in 44 SSc patients compared to RA patients.100 They described that the loss of hand function in SSc is not only similar to that of RA, although joint changes in both diseases are different, but it has an important influence on the quality of life in these patients.100 A previous study that used HAMIS and Cochin Scale (CS) reported similar findings.101
Furthermore, Lorand et al., validated the usefulness of the Disease Activity Score 28 (DAS 28) using PCR and ESR, as well as of the Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI), to assess joint involvement in SSc.102 They reported that, although the four instruments are valid to determine severity of joint involvement in SSc patients, DAS28-ESR showed the best performance regarding reliability and construct validity.102
The levels of fatigue reported in SSc patients, measured by means of the general fatigue index (IGF), are similar to the ones reported by patients with neoplasms, RA or systemic lupus erythematosus (SLE).103 In addition, fatigue has a negative impact at many different levels in patients with autoimmune diseases, including SSc.104 Fibromyalgia, a disease frequently associated with high rates of fatigue, is very common in SSc patients, occurring in between 57 %-72 %.105
Treatment
There are few studies on specific treatment of OAM in SSc. The first line treatments for the management of synovitis are adapted from the RA management schemes. A small retrospective study with patients from the EUSTAR database suggests a beneficial effect of hydroxychloroquine in the management of the inflammatory joint involvement in SSc.106 Patients who develop contractures in the first years of the disease could benefit from the use of cyclophosphamide, methotrexate or leflunomide.20 Immunoglobulin, used in a treatment scheme over six months, could be effective in reducing joint symptoms and secondary impact on quality of life in SSc patients with severe joint involvement refractory to first-line treatments.107
The possible role of anti TNF-α in the management of SSc has increased the interest of different groups worldwide. There are reports of studies that give a possible role for this group of treatments in the management of arthritis in the SSc population.108 In a study conducted by EUSTAR in 2011 in centers specialized in SSc management, it was evidenced that the majority of experts from this society recommended the use of anti TNF-α molecules only in randomized clinical trials since their potential adverse effects on the disease are unknown.109 However, due to the difficulty of conducting a randomized clinical trial with biological drugs, only observational studies have been published in this field.
Elhai et al. evaluated through an observational study the effect of tocilizumab, a humanized antibody against the IL-6 receptor, and abatacept, a recombinant fusion protein that modulates T-cell co-stimulation mediated by CTLA4, in the management of refractory polyarthritis or myopathy associated with SSc.110 DAS 28 was used to evaluate the response to treatment, and HAQ-DI to evaluate its impact on quality of life, suggesting that both drugs could improve polyarthritis secondary to SSc.110 A phase 3 study is currently underway to evaluate the response to rituximab compared with placebo in SSc patients with OAM who do not respond to first-line treatments.111
In SSc patients with painful hands of multicausal origin, including osteoarticular involvement, the carpal tunnel hydrodissection with lidocaine guided by US, associated to local corticoid injection reduces pain scores by up to 67 %, with a sustained duration of up to six months.112
Orthotic management for joint contractures can be ineffective in late stages of the disease, not only because it exacerbates symptoms such as Raynaud's phenomenon, but because it does not generate significant relief in the deformities generated by contractures.113 On the contrary, surgical management can be considered to reduce pain in patients with advanced disease refractory to other treatments.114 Procedures such as: sympathectomy, calcinosis resection, arthroplasties or capsulotomies have been practiced but the real benefits are few, so they have fall into disuse.115,116
In conclusion, OAM in SSc are frequent. They also have an important impact on patient's quality of life, especially due to the limitation in hand functionality. Treatment is difficult and requires a multidisciplinary approach. Due to the above, OAM in SSc require early identification and intervention. In addition, further research including good quality randomized clinical trials is required to establish the best treatment strategy for these patients.

