











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The SARS-CoV-2 virus responsible of the COVID-19 pandemic, presents mostly with constitutional symptoms such as fever, myalgias, headaches and respiratory symptoms, however, it has been evidenced that there is a procoagulant pattern with elevated fibrinogen, D-dimer and prothrombin time. The pathophysiology under this mechanism is believed to be due to endothelial damage, which causes microvascular thrombi that impede homogeneous flow and produce a vascular shunt that is reflected in hypoxia and end-organ damage. Tang et al. evidenced that the use of anticoagulation with low molecular weight heparin in patients with COVID-19 and D-dimer >6-fold of upper limit of normal is associated with better prognosis and decreased mortality.1
It is relevant to take into consideration diseases that are based on a chronic inflammatory state such as rheumatoid arthritis, since it can interfere with the management and development of both rheumatoid arthritis and co-infection with SARS-CoV-2. We present a possible association between tofacitinib therapy and increased D-dimer in a patient with rheumatoid arthritis and COVID-19 infection.
Case report
We present the case of a 32-year-old female with past medical history of rheumatoid arthritis diagnosed approximately 10years ago, and no other relevant medical condition. No allergies, no surgical and obstetric history. Her treatment included tofacitinib 2.5 mg twice a day, leflunomide 20 mg daily, folic acid 1 mg daily and vitamin D 800UI daily. In the early stages of her disease the patient received etanercept and infliximab with no adequate response. She has been in remission since tofacitinib was initiated approximately 4 years ago. No history of thrombotic events since the initial diagnosis.
On April 2020, the patient reported flu-like symptoms, diarrhea and positive contact exposure to COVID-19. She underwent self-isolation, her symptoms resolved within the next 10 days. She tested positive for COVID-19 RT-PCR via nasopharyngeal swab. Additionally, the household members tested positive for COVID-19 antibodies.
She visited the rheumatology clinic on May 2020 due increased polyarthralgia and fatigue. On physical exam she presented bilateral painful and swollen metacarpophalangeal (MCP) and proximal interphalangeal joints (PIP) with a CDAI of 21 which represented moderate disease activity. Laboratory results are available in Table 1. Elevation of D-dimer was evidenced. COVID-19 antibodies test was IgM 0.51 (-) and IgG 20.77 (+). CXR and chest CT negative for infiltrates or consolidations. Hematology service was consulted in the setting of the hypercoagulable state of COVID-19, recommended rivaroxaban 10 mg daily, further modified to rivaroxaban 2.5 mg and prednisone 6mg. Further studies included lower extremity doppler negative for deep venous thrombosis, echocardiogram showed an EF of 60% with no structural abnormalities. On July 2020 COVID-19 antibodies test was IgM 0.98 (-) and IGG 12.09 (+).
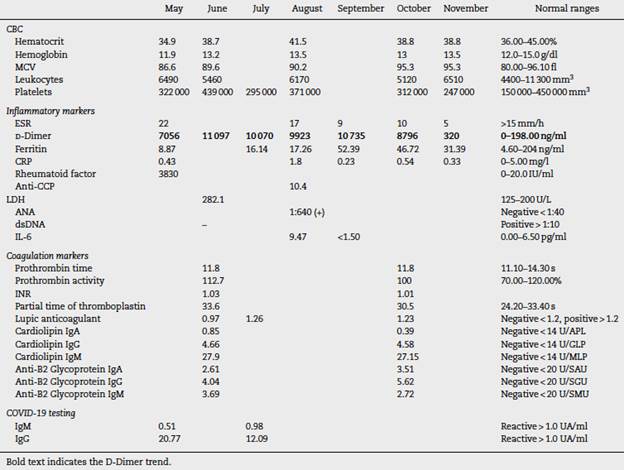
Further follow up showed an increase D-dimer trend for approximate 6 consecutive months (Fig. 1). In the mist of this situation, it was decided to discontinue tofacitinib in late October and start tocilizumab 8 mg/kg. Anticoagulation treatment was discontinued after 6 months and D-dimer reduction was seen. During her last visit in December 2020, the patient denied polyarthralgia, further CDAI was 0 and D-dimer levels were back to normal.
Discussion
We present the case of a patient with rheumatoid arthritis under treatment with tofacitinib of approximately 4 years duration without major complications, who in the presence of SARS-CoV-2 infection developed a hypercoagulable state with persistent elevation of D-dimer of approximately 6 months. The patient did not present any thromboembolic event, however, due to a history of rheumatoid arthritis, it was decided to start anticoagulant therapy. A normalization of D-dimer level was not evident until tofacitinib was discontinued, suggesting a possible association between the increase in D-dimer and background medication, which is potentiated with SARS-CoV-2 infection.
Miesbach et al. reported an incidence of thromboembolic events in 40% of critical patients infected with SARS-CoV-2,2 Zhang et al. reported an incidence of stroke in 5.7% of critically ill patients with the infection.3 Due to the presence of a hypercoagulable state, it is considered to start anticoagulation with LMWH in patients with elevated D-dimer in 3- to 4-fold increase.4
Mehta et al. highlighted in a letter to the editor the possible association between increased risk of thromboembolic events and the use of janus kinase inhibitors (JAKi).5 Tofacitinib is a JAK1/3 inhibitor used in the treatment of rheumatoid arthritis and ulcerative colitis, and has an FDA box warning for venous or arterial thrombotic events. The discussion is whether tofacitinib is a causal agent of thrombotic events,6 or if there is a background factor that contributes to the hypercoagulable state, as is the case of RA, where the risk of DVT is 0.3-0.7 per 100 patients/year compared to the general population where the risk is 0.1-0.4 per 100 patients/year.7
The FORWARD study has a registry of approximately 530 patients with rheumatic diseases who were asked if they made any changes to their therapeutic regimen during these months of the COVID-19 pandemic, 14% reported havingmade changes on their own and 11% Based on medical advice, this demonstrated a perception of an increased risk of complications from COVID-19 secondary to the immunosuppressants indicated for their underlying disease.8 However, it has been shown that patients with rheumatic diseases have a similar incidence of contagion and evolution of the disease compared to the general population.9,10
Because SARS-CoV-2 is a procoagulant risk factor and rheumatoid arthritis can be a causative agent as well, it is important to evaluate these patients, and if necessary, consider anticoagulant therapy.
Conclusion
The presence of rheumatic diseases such as rheumatoid arthritis is a risk factor for venous and/or arterial embolic events, however, the possible association with COVID-19 is uncertain. In addition, the added factor of the use of tofacitinib should be studied. In this case, the levels of D-dimer decreased to normal after discontinuing tofacinitib, which makes a possible association between the drug and an increase in the hypercoagulable state in COVID-19 more evident. More studies are needed to confirm this possible relationship.

