











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink1.Introduction
The practice of football or any type of physical activity planned with a specific objective, involves the application of loads that have a normal and necessary physiological response. Muscle fatigue is one of these responses, with both central and peripheral mechanisms that depend on several factors such as the characteristics of the subject and the exercise, as well as muscles involved, heat and humidity 1; the cause is multifactorial and sometimes it may not be perceived by the athlete, the acidification of muscles in contraction is one of the most important factors in its etiologic 2.
The lactate is a metabolic intermediary that increases with high-intensity exercise, has an inhibitory effect on the release of Ca+ from the sarcoplasmic reticulum, important factor in the mechanism of fatigue3)(4)(5. The peak of blood lactate (BL) values in approximately 3 to 8 minutes at the end of the exercise6; found the recovery of normal lactate values at 30 minutes, with a peak percentage of lactate clearance in this period 7. In a study with non-professional teams, observed that the BL was around 15 mmol, and can change according to the position of game8, add that when the different signs and symptoms of peripheral fatigue have been identified, it is essential to provide recovery strategies along with those established within the training plan 9.
That makes the organism look for its homeostasis and is in conditions to receive the new loads helping the adaptation process of the organism. Currently, the interest of professionals to prevent injuries in athletes has generated the development of programs or activities aimed at keeping players in optimal performance conditions. Took different models of analysis for the prevention of injuries in sports based on research that refers to the search for protocol designs where several steps should be considered for the development of programs to prevent sports injuries, starting with the identification of the problem and ending with the control of the results, this scheme has been used by professionals in different areas applied to sport worldwide, adjusting to specific needs 10.
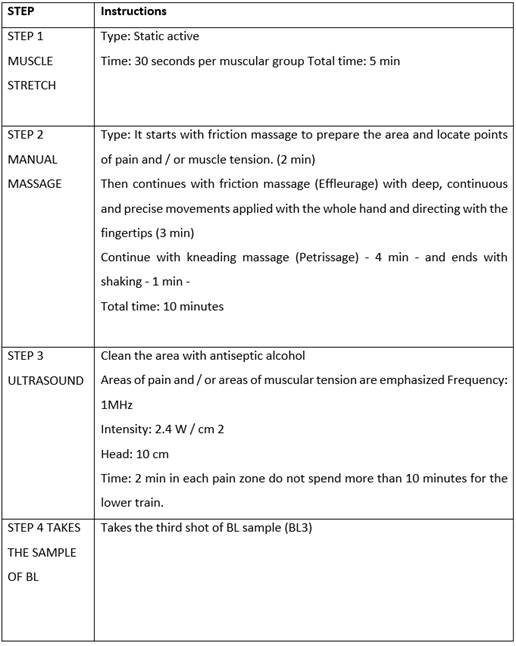
This group of activities is called “Physioprophylaxis” (PP) in which the physiotherapist, who attends the athlete, applies techniques to reduce the signs of muscle fatigue and collaborate in the process of recovery11)(12. For the design it must be take into consideration the training plan and specifically the higher intensity cycles where the athlete refers the fatigue response. Some physical and manual techniques used in physiotherapy such as stretching, massage, cryotherapy, hydrotherapy and ultrasound have been used as part of post-load recovery strategies, finding decreased pain and increasing muscle relaxation 13.
In the literature review, no scientific evidence is found of a protocol or guide based on the evidence of the effect of a plan that integrates the active - static stretches, manual massage and ultrasound (US) on the blood lactate concentrations for the management of acute muscular fatigue that prove their effectiveness. Report that the most used means of physical recovery post load are stretching and massage 13. The objective of this research is to determine the effects of a physio prophylaxis plan on blood lactate clearance as a sign of acute muscular fatigue, to reduce one of the risk factors for overload injury and propose a recovery guide protocol for physiotherapy professionals who work with this sport.
2.Materials and methods
Design: The investigation is quantitative of experimental type, longitudinal section. The study was carried out in the first semester of 2016.
Population and sample: The population consisted of 23 000 students in the degree program at the Pedagogical and Technological University of Colombia (UPTC), in Tunja, first semester of 2016. The sample corresponds to soccer players of the base group of the UPTC.
Instrument: The methodology applied is based on the protocols established for data collection, application of maximal incremental stress test (MIST) on cycle ergometer CYCLUS II, and application of the proposed psycho-prophylactic plan, taking two independent moments to perform inter- and intra-subject control. The tests are carried out in the moderate altitude of Tunja (2750 masl) and the conditions of the laboratory were Temperature 17.9 ° ± 0.4 and 17.3 ° ± 0.9 and Relative Humidity% 60.8 ± 2.8 and 61.5 ± 4.4, first and second moment, respectively. The group is divided into CG who perform passive recovery and in EG to whom the Physioprophylaxis plan is applied.
Procedure for data collection:The data collection was carried out during the second semester of 2016, and the link was available for a month. Subsequently, the data was exported to SPSS for analysis.
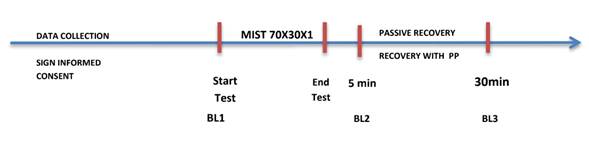
Figure 1 Research steps. BL1: Blood lactate, shot 1. BL2: Blood lactate, shot 2. BL3: Blood lactate, shot 3.
Maximal incremental stress test (MIST):The sample is divided into a control group for passive recovery and experimental group to apply the physio-prophylactic plan (moment 1) and changing the control group to experimental group (moment 2).
Physioprophylaxis plan: It is done after the stress test and takes 2 of BL
Statistical analysis : The data are presented with mean and DS; the Shapiro-Wilk normality test is applied and then the t-test is performed to compare the blood lactate clearance in the control and experimental groups at each time and in the same subject. The statistical analysis was carried out with the SPPS V22 and Jamovi V1.0.0 programs. A level of significance of p < 0.05 was considered.
Ethical considerations: All procedures were approved by the Ethics Committee of agenf.org (Act 15 of 07/16/2016 of www.agenf.org). Subjects were instructed to avoid strenuous physical activity in the 24 h prior to each experimental session. Each subject also abstained from food (overnight fasting), caffeine, and alcohol for 12 h prior to each experiment.
No personal data was collected that would allow the identification of the students, and participation was completely voluntary and anonymous. The study complied with current legislation in Colombia on the protection of personal data, and the ethical principles of the Declaration of Helsinki were always respected (beneficence, non-maleficence, autonomy, and justice). That informed consent was obtained for experimentation with human subjects.
3.Results
The demographic data of the 12 soccer players of the UPTC (n = 12) male, living in the city of Tunja are shown in table 1. Age (a) 23.4 ± 4.9, height (cm) 173 ± 6.1 and body weight (kg) 72.6 ± 8.2
Table 1 Demographic data of the sample (n = 12) age (a), height (cm) and body weight (kg) in M and DS

3.1 Kinetics of BL in CG and EG
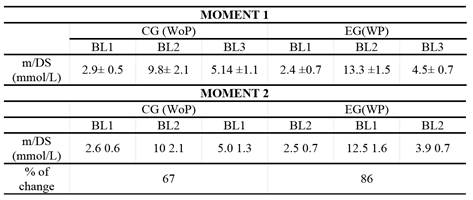
Table 2 shows the BL concentrations obtained at each measurement point of the 12 study subjects: rest, 5 and 30 min after the MIST for CG (passive recovery) and EG (recovery with plan). The percentage of change in relation to blood lactate concentrations in the number of mmol/L is higher in the experimental group 86% than in the control group, which is 67% compared to moments 1 and 2.
3.2 Blood lactate clearance (BLC)
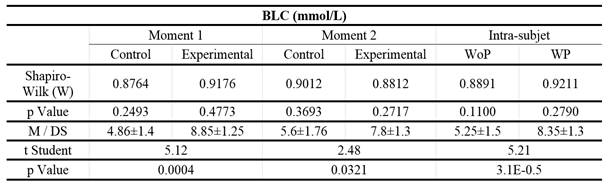
To obtain the data of the amount of mmol/L clarified, the difference between the samples BL2 and BL3 is taken. Moment 1 and 2 are compared between control group - experimental group and intra subject with and without plan application. The results were analysed with the Shapiro-Wilk test (W) to determine normality (p≥0.05). The BLC in both groups, control and experimental, in moments 1 and 2 and intra subject, were found to come from a variable with normal distribution.
Moment 1: The amount of blood lactate clearance expressed in mmol/L is lower in the control group (4.86 ± 1.4) and higher in the experimental group (8.85 ± 1.25). The p value of the test (p = 0.00044, p <0.05, t = 5.1298) indicates that the averages do show significant differences.
Moment 2: When calculating the amount of mmol/L of clarified lactate in blood, it´s observed that it is lower in the control group (WoP: 5.63 ± 1.85) and higher in the experimental group (WP: 7.87 ± 1.38). The p value of the test (p = 0.0321, p <0.05, t = 2.4862) indicates that the averages do show significant differences. Intrasubject: The statistical analysis of the BLC in the same subject, shows that in the period of passive recovery is lower (WoP: 5.25 ± 1.58) compared to the recovery period with plan (WP: 8.35 ± 1.33). The p value of the test (p= 0.0000316; p<0.05; t = 5.2114) indicates that the averages do show significant differences. (Table 3)
4.Discussion
In the research made in databases no studies that analyse the effects of a physio- prophylactic plan that integrates static active stretching, manual massage, and ultrasound on BLC as an indicator of peripheral muscle fatigue were found. The results show that the combination of these media obtains a positive response as a post-effort recovery method. The incremental exercise test on a cycle ergometer to produce lactate, has been used in several studies to measure lactate concentrations, a study with cyclists in Australia compared the effects of active versus passive recovery on metabolism and performance compare the effects of active versus passive recovery on metabolism and performance, taking 15 minutes of recovery and BLC in active and passive recovery of 4.4±0.7 and 7.7±1.4 mmol/L respectively, conclude that these data do not support the benefit of active versus passive recovery in the maintenance of subsequent performance 14.
The highest BLC found in this study were 13.3± 1.5 mmo/L similar to those found by Mohr 15 during a soccer game with individual BLC values around 12mmol/L and above to the study by Krustrup 16 that examined the behavior of blood lactate in the two stages of a soccer game whose result was 6±0.4 mmol/L, which means that the test performed in the present study had blood lactate concentrations that can be present at a soccer game.
Previous studies compare strategies of recovery after the load of training and competitions in different sports to determine the most efficient technique; In the year 200017, evaluated the removal of blood lactate (BL) in maximal exercise; after 15 minutes they found that during the whole intervention phase BL extraction rates were 0.37±0.03; 0.38±0.04, for active and combined recovery; and 0.21±0.04 and 0.16±0.06 mMxmin-1 for recovery with massage and passive; Comparing with the results obtained in this research, in maximal exercise after 30 minutes the BLC values for moment 1 in the control group was 4.86 ± 1.4 mMol/L and for experimental group of 8.85±1.25 mMol/L; at moment 2 for the control group it was 5.6±1.76 and for the experimental group it was 7.8±1.3; intra-subject control group of 5.25±1.58 and experimental of 8.35±1.3 mMol/L, this shows that a greater number of clarified mMol/L of BL is present in a combined recovery with static active stretching, manual massage and ultrasound. And much more significant if you take as a reference the study conducted by Krustup 16, where the average rate of blood lactate decrease taken at half time of a soccer game was 0.1 mMol/L, which means that it would take 60 minutes to reduce the blood lactate concentration by 6 mMol/L.
In other study was determined the effect on physical performance of 3 recovery modalities after a game in 28 players 18. The positive effects observed in the perception of recovery after the combined modality (cold water immersion and active recovery) suggest that this approach can be effective in young players after intense soccer match and that the combined strategies have better results than individual methods. In Brazil compared three recovery methods on the clearance of BL where they performed a maximal test to induce lactacidemia in 23 players, dividing into group 1: active recovery with BL removal of 47.62%, group 2: passive recovery removal of 18.2% and group 3 with ice application had a removal of 16.9% with a recovery time of 10 minutes 19. Comparing these results with those obtained in the present study, it is observed that the physio-prophylactic plan demonstrates a blood lactate removal or clearance of 86% applying the proposed plan (experimental group) versus 67% clearance in passive recovery (control group), with a recovery time of 30 minutes, higher than in the study of these authors where the time is insufficient to observe major changes.
There are techniques such as cryotherapy, thermotherapy and compression measures, normally used as means of post-load recovery supported scientifically with objective parameters of physical performance; they affirm that although massage is one of the most used means as a recovery strategy, it lacks of studies that support its effectiveness 9. It is attributed anti-inflammatory benefits, reduces stress, effects on muscle pain of late onset, among others, but no results are shown on blood lactate concentrations; the present study complements the massage with stretching and ultrasound, demonstrating the effects that this physio-prophylactic plan has on the clearance of blood lactate as a sign of peripheral muscle fatigue.
Perspectives
By applying a physioprophylaxis plan that integrates static active stretching, manual massage, and ultrasound as a post-load recovery strategy on blood lactate clearance in university players, it shows that the amount of mmol/L of BL cleared at the end of 30 minutes of recovery in EG was higher with 8.8 mmol/L (86% of change), compared to the CG with 4.8 mmol/ BLC L (67% of change). The results obtained support the physioprophylaxis plan proposed for use in sports physiotherapy as part of acute muscle fatigue recovery strategies, for the prevention of overload injuries and the maintenance of performance conditions in the athlete.

