











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Migration is understood as the movement of a group of people from one territory or state to another, or within it, whatever its size, composition or causes (IOM, 2006). In recent years, given the perception of Chile's economic stability and security, this country has become a migration destination for individuals and families seeking opportu nities and conditions not found in their homeland, mainly from neighboring South American countries, that is to say, from Peru, Ecuador and Colombia (ECLAC / CELADE, 2006; Stefoni, 2011). This immigration is characterized for coming from the border, since approximately 57% of the total migrant population during the period of 2005-2014, came from countries like Peru (31,7%), Argentina,(16,3% ) and Bolivia (8,8%). Additional sources of immigrants from other South American countries amount to 73% if Colombia, Ecuador and Brazil are added (DEM 2016).
Migration is considered a process "involving both causal and developmental factors as well as consequences, both to the society of origin as for the one of destination ': (Cano and Soffia, 2009, p. 5). In order to adapt themselves to their new environment the immigrant has to take into consideration both their mental and cognitive resources to cope with the changes that will confront them. Also, migration can constitute an instance of growth and develop ment, although it involves experiencing difficult situations and problems (Achotegui, 2010, 2012, Urzûa et al.2015). The immigrant must face new challenges such as cultural adaptation, xenophobia, poor access to public institutions, migratory legalization procedures and economic hardship, among others. These factors can become stressful and upset the psychological well-being of the immigrant, directly affecting their mental health.
The relationship between migration and mental health has been studied from the migrants' previous contexts to their environmental displacement, up to the time of establishing themselves in the new country. Variables present at the place of origin such as unemployment, lack of economic resources, low education, among others, function as a risk factor for developing some kind of psychopathology after migration (Levecque, Lodewyckx & Vranken, 2007). Also, suffering from anxiety disorders may be relevant and/ or influence the decision to migrate to another country, since the migration process forecasts the onset of anxiety disorders and subsequently may affect their state of mind (Breslau et al., 2007), causing, for example, the occurrence of depressive symptoms at any age (Sternberg & Lee, 2013).
Nevertheless, recent research findings suggest that there is not a direct link between migration and the occurrence of psychopathological disorders. For example, fewer cases of mood disorders, anxiety and abuse, and drug dependence in migrants were found in comparison to those born in the US (Alegría et al., 2007; Breslau & Chang, 2006; Grant et al., 2004. Takeuchi et al, 2007). In a study of Peruvian immigrants in Chile, it was found that the time residing in their new country is not linked to the presence of a psychia tric disorder (University of Chile Clinical Hospital, 2008).
Apparently, the relationship between migration and mental health is not simple, because migrating itself could not explain or predict the presence of psychopathological disorders, for there are multiple individual and contextual variables acting as mediating factors and moderators in this relationship (Collazos Qureshi,Antonin and Thomas-Saturday, 2008). In addition, migrating requires good physical and mental health to properly manage the series of changes that involve settling, adaptation and integration (Blight, 1994)
The acculturation process, as defined by Berry (2005), is one of the variables studied and can be regarded as the context where the relationship between mental health and migration occurs. It is a cultural change process where reactive changes (rejection of the new culture) or rather, indirect and psychological processes can occur, that could affect the adaptation to the new society when encounters between social groups with different customs, norms and ideologies interact. Faced with this reality, a series of internal changes is initiated, along with immigrants' behavioral repertoire, when interacting with the new culture. This process is defined by Graves (1967) as psychological acculturation, which is specified as praxis in the so-called acculturation strategies.
Acculturation strategies are governed by the desire to maintain one's cultural identity, and the interest in participa ting in the new culture (Berry, 2001). From Berry's model and the Interactive Model of Acculturation (MIA) proposed in 1997 by Bourhis, Moise, Perreault and Senecal (in Fajardo et al, 2008) there are four acculturation mechanisms: (a) integration (also called biculturalism), ,where the immigrant seeks to maintain their original values and participate in the new culture; (b) assimilation, where one chooses to take the values of the new culture, forgoing traditional and indigenous values; (c) marginalization, where individuals do not seek interaction with the new culture nor maintain their own cultural origin; and (d) separation, intended to validate and maintain only the tradition of their culture, having almost no contact with the new society (Berry, 2001; Sanchez and Lopez, 2008).
According to the way the immigrant chooses to follow the process of acculturation, rather than a decision, it is a negotiation between the components of the cultural context of the host country and the tools and skills of the immigrant (Yanez and Cardenas, 2010) which is going to influence their state of mental health. For example, a research done with immigrant women living in the US showed that acculturation generates higher levels of stress when having to deal with problems like cultural adaptation, legal situations and institutional systems that oppress them. Additionally, they face social discrimination and economic hardship, having increased risk of symptoms of depression that alter the level of their mental health, as compared to US-born Latinas (Sternberg & Lee, 2013). Studies done in Chile have shown that high levels of acculturation stress affect an increase in symptoms associated with mental health problems (Urzua, Heredia and Caqueo-Urizar, 2016).
Given that the evidence is not conclusive, the question arises: does the acculturation strategy used by adult immigrants affect their mental health? To respond to this question, the present study analyzed the relationship between mental health and acculturation strategies used in immigrant populations. It is hypothesized that the mental health of immigrants would be influenced by the type of strategy used in the encounter with the new culture. Specifically, the presence of psychopathological symptoms associated with mental health problems may be related to the presence of acculturation strategies of marginalization and separation, unlike the strategies of integration and assimilation.
METHOD
Sample
Participants in this study were 431 Peruvian and Colombian immigrants aged over 18 years old, residing for at least six months in the city of Antofagasta. Foreign visitors or tourists were excluded. Colombian and Peruvian immigrants were chosen to form this sample, considering that they constitute the highest migrant population in the city of Antofagasta (DEM 2015), attracted mainly by the mining industry and services derived (construction, trade, sales).
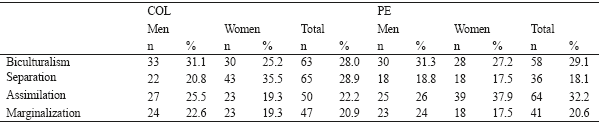
Of these participants, 207 were men (48%) and 224, women (52%). Their ages ranged between 18 and 65 years. The average residence time of the Colombians surveyed was 2.3 years, while that of Peruvians was 4 years. About 30% of both samples have completed high school and 20% of Colombians and 14% of Peruvians had completed technical training. In both populations, 75% declared to be actively employed. In the case of Colombians, 48% reported incomes between 100 and 300 thousand Chilean pesos (between $150 and $450 U.S. dollars), and 31% between 300 and 600 thousand CLP (between $450 and $900 US dollars), while 44 or 38% of the Peruvians declared themselves to be in similar categories. The distribution of respondents by gender and age is shown in Table 1.

Instruments
The instruments used were The Scale of Attitudes towards Acculturation (Basabe, Zlovina & Paez, 2004) and the Self-report Outcome Measure questionnaire OQ45.22 (Von Bergen & De La Parra, 2002).
Scale of Attitudes towards Acculturation
This questionnaire on strategies and attitudes of acculturation elaborated by Basabe, Zlovina and Paez was originally proposed by Berry (2001). It consists of two subscales that measure, on the one hand, the desire to maintain the customs of the society of origin, and on the other, to adopt the customs of the host country. Each of these subscales consists of 6 items that address how immigrants engage in private matters (3 items pertaining to customs related to family, friends, and beliefs) and public subjects (3items oriented to customs related to work, the welfare system and the political system of the government). Responses are marked within a range that goes from 1 (none) to 5 (very much).
This scale has been used in previous studies carried out with migrants in Chile (Arenas and Urzua, 2016) and other Latin American studies with similar populations (Castro, 2011; Sosa and Zubieta, 2012). However, information regarding its psychometric properties has not been recorded. The present study conducted a reliability test using Cronbach's Alpha, where the following values were obtained: .81 to maintain customs of the country of origin;,65 to adopt customs of the country of arrival; .81 for interest to maintain customs, and ,82 for interest in adopting customs.
Self-report Outcome Measure questionnaire OQ-45.2
This instrument measures the progress of psychological therapy in terms of assessing the patient's level of mental health during the process. It has consistency indicators above, 75; for concurrent validity, criterion validity and sensitivity (proportion of true positives correctly identified), of, 90; and for specificity, 93 (proportion of true negatives correctly identified) (Von Bergen and Parra, 2002).
It is a Likert ordinal level summative scale, which is answered by choosing between five categories according to how often happens what is stated in each item: "never=0", "rarely=1", "sometimes=2", "often=3" and "almost always=4". It consists of three dimensions: Symptoms (SD) with 25 items, to detect depression and/or anxious states; Interpersonal relations (IR), with 11 items to measure levels of satisfaction and problems in this area; and Social role (SR), with 9 items that measure the person's levels of conflict, dissatisfaction, disorder or inadequacy in relation to employment, family roles and leisure. The scores were obtained by adding the points in the full scale (values from 0 to 4 for each item), which range from 0 to 180 points, and adding up the scores in each dimension. The cut-off point of the full scale is 73, which is divided between low and high score, referring to the degree of discomfort with life in general, considering symptoms, interpersonal relationships, and social role. The cut-off point for these dimensions is 43, 16 and 14, respectively.
Procedure
The Ethics Committees of the Universidad Católica del Norte and the National Commission on Science and Technology (CONICYT) approved this research.
Since the exact number of the population universe was not known, nor was the sampling frame, a non-probabilistic sample was used through a random snowball strategy to choose the first participants, with a maximum of 6 chains in order to achieve adequate representation. People were invited to participate voluntarily in the study, explaining to them the purpose of the study and then asking them to sign the informed consent document, and requesting them to suggest three contacts as potential participants. In case any of them refused to participate or when a participant was already in the sample, the chain broke.
The application time of the instruments was approximately 2 hours, with 80% level of participation in the study. The data were entered into a constructed database built in SPSS 17,0.
The Student-T test was used to assess differences between means of the variables given, by gender and country of origin. Later, an ANOVA was performed to evaluate possible differences in mental health means among different acculturation strategies. Normality tests variables (Kolmogorov-Smirnov and Shapiro-Wilk) were performed; however, although some of them did not have a normal distribution, with sample sizes above 40, the T test and the ANOVA test were used even if the data distribution was asymmetrical and there were no outliers (Pardo, Ruiz and San Martin, 2014).
RESULTS
First, the descriptive statistics of the acculturation strategy variables and mental health are presented. Then the average of the mental health of the participants was categorized according to the strategy used, ending with the ANOVA results.
Acculturation Strategy
The most used strategy in the entire sample was biculturalism acculturation (also called integration), followed by assimilation. By stratifying the analysis by gender, biculturalism was maintained in men as the strategy most used, while in women it was assimilation followed by separation (See Table 2)

When analyzed by country, separation strategy was mostly used by the Colombian population, followed by biculturalism, while in the Peruvians assimilation was followed by biculturalism (See Table 3).
Mental Health
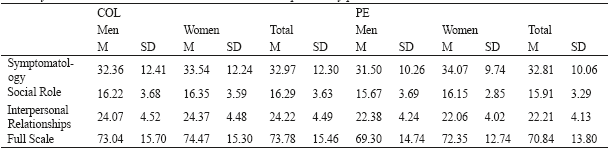
In the overall sample, women scored higher in all domains evaluated compared to men; however, this difference was not statistically significant for any of the dimensions evaluated (see Table 4).
Table 4 Means and SDs in mental health domains assessed by gender and total

Note: Differences between men and women are not significant (1) (t (403) = -1.626; p =, 105); (2) (t (407) = -1.111; p = .911); (3) (t (416) = - 858; p = 392); (4) (t (388) = -1.483; p = .139).
Analyzing the means by country of origin, it appeared that the Colombian population reported higher scores in all dimensions, and in the total scale than the Peruvian population (see Table 5). Only in the subscale of personal relationships did the probability of finding the value of T-even if the null hypothesis were true- was less than 0.05. Therefore, the null hypothesis that there were no significant differences between means was rejected, considering that the Colombians' average is significantly higher than the Peruvians' (t (407) = 4,666 ; p = 0.000).
Tabla 5 Medias y DE en dimensiones de salud mental evaluados por sexo y país COL PE
Note: PP = Peruvian population; COL: Colombian population
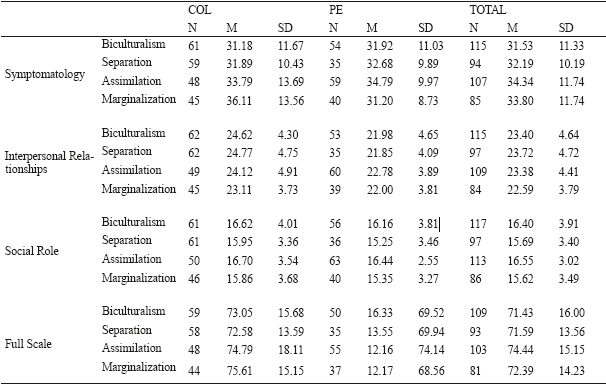
Table 6 shows the mean and standard deviation in each of the dimensions of mental health evaluated, divided by both categories of acculturative strategies and by country.
Table 6 Mean in mental health according to acculturation strategy and nationality.
Note: PP = Peruvian population; COL: Colombian population
At the level of the symptoms dimension, a greater presence of symptoms was observed in those who opted for an assimilation strategy, while bicultural (or integrated) reported fewer symptoms. Despite this, they were only statistically significant in the total sample (F (3.401) = 4.243; p = 0.006). Additionally, in the Colombian population (F (3.213) = 4.707; p = ,003), when marginalization strategy was used, it was observed to have a significantly higher mean than separation (p = 0,004 and p = 0,001 respectively).
In interpersonal relationships, those who assimilated reported a higher average in difficulty, while marginalization was lower (p = 0,012). This difference was only significant at the level of the total sample (F (3.405) = 3.648; p = 0,013). No other significant differences were observed when separating the sample by country.
In both the dimensions of social role and in the total scale, those who assimilated showed the highest scores over all the other strategies. However, no statistically significant differences were found between the scores of each strategy, or the total sample, or by stratifying the analysis by country.
DISCUSSION
The results showed identifiable common and specific factors for each migratory group. Both populations use the strategy of biculturalism (or integration); however, it is not the most used, as in the case of the Colombian population which mostly reported the use of separation, followed by biculturalism, while in the Peruvian population, it is assimilation followed by biculturalism. In the case of mental health, the Colombian population reported the worst results compared to the Peruvians evaluated, especially in the dimension of interpersonal relationships.
The initial hypothesis was that the type of strategies used when encountering the new culture would influence the mental health of immigrants. Specifically, the presence of psychopathological symptoms associated with mental health problems, may be related to the presence of acculturation strategies of marginalization and separation, unlike the strategies of integration and assimilation. The results found were different from expected, there were more symptoms declared in those who chose assimilation and less for those who chose biculturalism (especially in the Colombian population). In addition, immigrants who use assimilation have greater problems in their relationships.
As for mental health, migrants experience a general discomfort in their new life. This condition is particularly evident with respect to social relationships established in familiar terms and in terms of work, school, community and socializing. This could be linked to the difficulty of adjusting to the roles that are required when functioning in these areas. Women, in particular, have reported experiencing greater presence of symptoms of anxiety and depression, greater conflict in interpersonal relationships and greater difficulty in their ability to fit in the roles they assume. Hence, they tend to manifest or perceive a greater degree of discomfort when going about building their lives in their new Chilean society, in the context of the city of Antofagasta. In addition to this reality is the fact that Colombian and Peruvian families -in their respective countries of origin-face economic, political and social insecurity, which hinder the stability that people yearn for their survival (Stefoni, 2004). In this respect, a study by Levecque, Lodewyckx & Vranken (2007) showed that unfavorable conditions in employment, income, education and others constitute risk factors in terms of people's mental health.
Making the decision to migrate to another country suggests there is a means for solving the problems immigrants face in their homeland, while developing a set of expectations with respect to the new and different culture they will encounter. The aim is to find new and better job opportunities, less aggressive and dangerous social systems and a better socio-cultural-economic and political context that allows a healthy growth and development for the individual and their families, through nurturing environments. However, such expectations do not unfold as quickly or as easily as expected, thus, creating a gap between the real and the expected, which constitutes a risk factor for mental health.
In terms of acculturation strategies of Peruvian and Colombian immigrants, in their encounter with the Chile/ Antofagasta culture, there is greater dissatisfaction with life in general in those who have chosen to use assimilation, leaving aside their traditions and customs of origin. Although there is no evidence of this, graffiti around Antofagasta suggests that there is great resistance on behalf of the host community. Since immigrants are a new admission into the local system, this tends to break the order and stability in maintaining one's existence, and disrupts native Chilean and Antofagastino's sense of identity.
Due to the above, any attempt that might threaten to dilute their community is rejected, which may increase the discomfort of assimilated immigrants, who primarily have difficulties in interpersonal relationships. Both of these mechanisms are most commonly used in these two groups of immigrants in the context of the Antofagasta society. Seen in a broader perspective are the functions assumed in the immigrant's new context, such as their role at work, in the family, in the school system and the various areas of interaction.
Conversely, those who use the strategy of separation report feeling a lesser degree of dissatisfaction with the established way of life. In systemic terms, this can be interpreted as if migrants don't make enough efforts to be accepted or integrated into the host culture, thereby experiencing no rejection from the Antofagastino social system. This is due to having a lower degree of interaction, and because their sense of belonging and identity is linked to a more permanent contact with their countrymen, they try to maintain the balance within this social system, thereby ensuring their survival in the Antofagastino Chilean culture.
Additionally, the group who decided to adopt a marginalization acculturation strategy is not motivated to feel part of any cultural and social system. Given that on one hand, being recognized as Peruvian or Colombian immigrants implies dysfunctional interactions with the Chilean population, this situation moves them away from the chances of finding the psychological, economic, work and family welfare, which were the reasons that led them to emigrate. The reason for them being there is mainly for providing for their family back home, despite the distances. This is confirmed by Zapata (2009) with his study on transnational families in which he observed how immigrant parents fulfill their parental role and compensate for the physical distance that separate them from their children through available communication resources such as the telephone, the Internet, etc. (Pedone, 2007).
The social role is defined in social interaction, in the context of the relationship with others, in the encounter with other subjectivities, as Carabana and Lamo de Espinoza (1978) state. Social life involves a process whereby through interactions, symbols are internalized and stimuli are re gulated from the environment. One's own responses are processed to make sense of one's self-definition. In the occurrence of the social act, the individual takes a set of attitudes seen in others in the situation that it occurs. Along these lines is the trend to accept symbols, values and traditions of the culture of origin. The result of this process, in the new social group, if adopted, is breakdown, loss and grieving when it comes to what is allowed, and can result in a feeling of discomfort, uneasiness and difficulty, having to stop from being someone with a different identity. Even if it means conflict and the rejection of the Antofagastino-Chilean society, which resists immigrant's integration and sets stiff limits and barriers to impede the acknowledgment of the social roles of these immigrant groups.
In this regard the situation of immigrants is complex as they come and settle into the Antofagasta's society, with a high degree of vulnerability in terms of mental health. Thus, when the migrant has to face the rigid limits established by various social subsystems, it is possible that this condition triggers behaviors and symptomatic states that can affect a variety of factors impacting the functioning of the host context.
This situation highlights the urgent need to considering the implementation of actions, strategies and public policies in terms of social integration and work, to promote social welfare between host communities and immigrants. Harmonizing the tendency of habits and customs of the country of origin into a healthy coexistence with the new habits and customs of the host country, as the complete elimination of the identity of minority group (assimilation), constitutes a risk to their mental health and wellbeing.

