










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkActa Colombiana de Psicología
Print version ISSN 0123-9155
Act.Colom.Psicol. vol.21 no.2 Bogotá July/Dec. 2018
https://doi.org/10.14718/acp.2018.21.2.4
Articles
Negative affect as a high order emotional factor in cardiovascular patients
2 Universidad de los Andes, Colombia.
Depression, anxiety and anger trait have been shown to be factors related to poor prognosis in patients with cardiovascular disease. A sample of 168 patients with ischemic heart disease that have had a cardiac event in the last month (age: Mean = 64 years, SD = 11; 66.7 % men) was evaluated to verify the existence of negative affect as a common factor among the previous emotions in these patients. Patients answered the Spielberger depression, anxiety and anger trait questionnaires. Exploratory factorial analyses were carried out to confirm the factorial structure of the scales. Confirmatory factor analysis confirmed the existence of negative affect as a higher order factor (X 2 = 3.42, p > .05; CFI > .95, TLI > .95, SRMS < .05). These results suggest that it is important to consider dimensional models for the treatment of emotions in this population.
Key words: depression; anxiety; anger; cardiovascular diseases; prognosis
La depresión, la ansiedad y la ira rasgo han evidenciado ser factores asociados a un peor pronóstico de los pacientes con enfermedad cardiovascular. En el presente estudio se evaluó una muestra de 168 pacientes con cardiopatía isquémica que habían tenido un evento cardíaco en el último mes (edad media = 64 años, DT = 11; 66.7 % hombres) para contrastar la existencia del afecto negativo como factor común entre la depresión, la ansiedad y la ira rasgo. Los instrumentos utilizados fueron las escalas rasgo de los cuestionarios de depresión, ansiedad e ira de Spielberger. Como resultado, los análisis factoriales exploratorios realizados confirmaron la estructura factorial de todas escalas, y el análisis factorial confirmatorio corroboró la existencia del afecto negativo como factor de orden superior (X2 = 3.42, p > .05; CFI > .95, TLI > .95, SRMS < .05). Los resultados de este estudio señalan la importancia de considerar modelos dimensionales para el abordaje de la emoción en esta población.
Palabras clave: depresión; ansiedad; ira; enfermedad cardiovascular; pronóstico
A depressão-traço, a ansiedade-traço e a ira-traço mostraram evidências de que são fatores associados a um prognóstico pior dos pacientes com doença cardiovascular. No presente estudo, avaliou-se uma amostra de 168 pacientes com cardiopatia isquêmica que tinham sofrido um evento cardíaco no último mês (idade média = 64 anos, DP = 11; 66.7 % homens) para contrastar a existência do efeito negativo como fator comum entre a depressão, a ansiedade e a ira-traço. Os instrumentos utilizados foram as escalas traço dos questionários de depressão, ansiedade e ira de Spielberger. Como resultado, as análises fatoriais exploratórias realizadas confirmaram a estrutura fatorial de todas as escalas, e a análise fatorial confirmatória corroborou a existência o efeito negativo como fator de ordem superior (X2 = 3.42, p > .05; CFI > .95, TLI > .95, SRMS < .05 ). Os resultados deste estudo assinalam a importância de considerar modelos dimensionais para a abordagem da emoção nessa população.
Palavras-chave: ansiedade; depressão; doença cardiovascular; ira; prognóstico
INTRODUCTION
Ischemic cardiopathy is a term that groups together a number of medical conditions characterised by an atherosclerotic process and which manifest itself as angina pectoris; acute coronary syndrome, which includes severe myocardium infarct and unstable angina; and sudden death by cardiac arrest (Guyton & Hall, 2006), associated with high rates of mortality globally (WHO, 2011) and in Colombia (Ministry of Health and Social Protection, 2016). These are multicausal chronic diseases in which emotional factors, such as anxiety, depression and/or anger/hostility have proven to play a significant role in patient prognosis (American Heart Association, 2010; Kubzansky & Kawachi, 2000; Lanas et al., 2007; Yusuf et al., 2004).
Depression is considered a risk factor leading to worse prognoses in patients with acute coronary syndrome (Lichtman et al., 2014), as it doubles their risk of mortality from heart disease. It has been found that the risk of events increases as depression levels increase, in patients with treatment resistant depression presenting greater risk (Smith & Blumenthal, 2011). Anger-hostility is associated with a bad prognosis in people with cardiovascular disease (CVD) (Chida & Steptoe, 2009) and it increases the risk of the occurrence of an accident by around 20% (Denollet & Pedersen, 2009). Anxiety is common in people with CVD, and reported by between 5 and 10% of patients (Alarcón & Ramírez, 2006). Studies in relation to this emotion are not very conclusive, perhaps because the results vary according to the disorder or according to whether the anxiety is considered chronic (Kubzansky, Davidson, & Rozanski, 2005). It has been reported that persistent anxiety is associated to cardiovascular events in the two years following the cardiovascular event (Moser et al., 2011), and the recommendation is that it should be included in the primary assessment of patients with heart disease (Celano, Suarez, Mastromauro, Januzzi, & Huffman, 2013). It is worth noting that CVD with levels of subsyndromal anxiety has not been systematically studied (Kubzansky et al., 2005).
The evidence on emotional factors in relation to the prognosis of CVD patients suggests that this association is given as dose-response, whereby risk is associated to the level of emotional severity (Kubzansky et al., 2005; Smith & Blumenthal, 2011). Similarly, the impact of the intervention of emotional factors seems to be associated to the nature and the chronicity of the disorders, be they structural or symptomatic aspects (Kubzansky & Thurston, 2007). These results would seem to confirm that the relationship between emotions and CVD prognosis is not given by clinical entities but rather by the frequency and intensity of the emotions. As such, the study of emotional factors in patients with CVD would not adjust to traditional epidemiological models, but rather suggests the need to approach it using dimensional models of emotions (Clark, 2005; Posner, Russell, & Peterson, 2005).
The studies point out that patients with CVD often present joint symptoms of depression and anxiety, and anger-hostility (Denollet & Pedersen, 2009), and that this co-occurrence is not exclusive to patients with CVD (American Psychiatric Association, 2013). It is thought that around 55% of patients with a main diagnosis of one of these disorders, has at least one additional diagnosis in these categories and that this rate increases to 76% when considering diagnoses throughout life (Brown & Barlow, 2009). This coincides with advances made in the field of behavioural genetics and temperament which highlight that there are no clear differences between emotions and indicate dimensional models for the study of affective phenomena (Posner et al., 2005).
Dimensional models of emotions assume that there is an intercorrelation between them, meaning that we seldom experience only one (Posner et al., 2005). It has been pointed out that there are two bio-behavioural dimensions referring to the affective structure: positive and negative affectivity (Clark, 2005; Watson, Clark, & Carey, 1988). The dimension of negative affect refers to a subjective malaise and represents the common factor between several negative emotional states, such as fear, sadness, anger, dissatisfaction, and guilt (Watson, Clark, & Stasik, 2011). It is worth pointing out that the negative affect's weak correlation to the positive affect, may mean that they are independent dimensions. (Watson, Clark, & Tellegen, 1988). As such, the affective structure implies two different levels: one higher level reflecting the influence of general affect and a lower one referring to the differentiated effect of specific negative emotions (Watson & Clark, 1992). This structure was initially verified in the English-speaking world, but is currently being tested in cultures such as the Japanese (Watson, Clark, & Tellegen, 1984), Spanish (Sandín et al., 1999) and Latin American (Moriondo, Palma, Medrano, & Murillo, 2011; Robles & Páez, 2003). However, these studies have involved the healthy population.
The link between negative affect and CVD is beginning to be mentioned in some studies, but these have focused on the incidence of the disease rather than on patient prognosis. Also, the topic is approached in the discussion of the results, rather than by the verification of affect as a high order factor. In this respect, it has been reported that there is a negative relationship between blood flow in the brachial artery, which can be considered a marker of arteriosclerosis, and the trait of anger in men. The authors point out that these results consolidate the inverse relationship between negative affect and cardiovascular health and imply that these connections are evident in the continuum of the disease (Schott, Kamarck, Matthews, Brockwell, & Sutton-Tyrrell, 2009).
The above points to the need to verify the existence of the latent factor of negative affect in patients with CVD, in order to empirically support a line of work which has begun to be mentioned in studies and that allows us to understand the synergic effect that this common factor may be having on patient prognosis after the cardiac event (Torquato Jr, de Souza, Iosifescu, & Fraguas, 2012). Thus, the purpose of this study was to answer the following question: Is there a common factor between the symptoms of depression, anxiety and anger traits of patients with ischemic cardiopathy?
METHOD
Population and sample
The reference population included patients with ischemic cardiopathy who had had acute coronary syndrome over the previous month. Time-delimited purposive sampling was carried out, involving all patients that fulfilled the inclusion criteria for six months from the beginning of the study. The patients were contacted in two places, a hospital institution offering cardiology services to those who had been admitted for the cardiac event, and a rehabilitation unit in which patients who had been referred after the event were evaluated.
The inclusion criteria were as follows: (a) the patient had to be over 18 years of age, (b) the cardiac event must have happened a maximum of 30 days prior to the initial assessment, and (c) they must have already had at least one session in the cardiovascular rehabilitation program (if applicable). Patients with some disability that prevented the correct solution to the psychological tests were excluded (exclusion criteria).
The sample was made up of 168 patients aged between 21 and 91 with a mean age of 64 (S.D. = 11.1). Some 66.7% were men and 64.3% were married or lived with a partner. With respect to their cardiovascular health, 42.9% (72) of the patients had suffered severe myocardium infarct previously (See Table 1).
Table 1 Descriptive statistics for 168patients with ischemic cardiopathy
| N (%) | M (S.D.) | |
| Age | 63.7 (11.15) | |
| Men | 112 (66.7) | |
| Married or with a partner | 108 (64.3) | |
| Socioeconomic stratum | ||
| Low | 63 (37.5) | |
| Medium | 67 (39.9) | |
| High | 23 (13.7) | |
| High School or less | 51 (30.4) | |
| Severe myocardium infarct | 72 (42.9) | |
| Interventions | ||
| Angioplasty | 18 (10.7) | |
| Bypass | 100 (59.5) | |
| Rehabilitation | 62 (54.4) |
N: number of people, M: mean, S.D.: standard deviation
Evaluation instruments
State-Trait Depression Inventory (ST-DEP). This inventory is made up often items, five for dysthymia and five for euthymia as overall propensity. The test's levels of internal consistency in the general Spanish population oscillate between 0.71 and 0.92, revealing levels which are acceptable through excellent (Spielberger, Buela-Casal, & Agudelo, 2008). In the Colombian population, Cronbach'sAlphas that oscillate between acceptable and good (0.71 and 0.86) have been reported for the general population (Agudelo, Gómez, & López, 2014). In terms of validity, the factorial analysis found the two factors through promax rotation in the Spanish (Spielberger et al., 2008) and Colombian versions (Agudelo et al., 2014). In this study, the scale reached good reliability (α = 0.86).
State-Trait Anxiety Inventory (STAI). The STAI trait scale is a 20-item self-report inventory (Spielberger, Gorsuch, Lushene, & Seisdedos, 1999). The alpha coefficient of the American version oscillates between 0.83 and 0.92 (Spielberger, Gorsuch, & Lushene, 1970). In the Spanish version, the KR20 indices for the anxiety trait oscillate between 0.84 and 0.87 (Spielberger et al., 1999). The levels obtained by these internal consistency indices reveal levels that range from good to excellent in both versions. It is worth noting that the Cronbach's Alpha obtained in this study showed the same trend at reaching a value of 0.85.
State-Trait Anger Expression Inventory (STAXI 2). The STAXI 2 trait scale is a 10-item self-report inventory with two subscales, temperament and angry reaction, which configure the anger trait. It is considered a reliable test, with acceptable test-retest correlations of 0.71, and a good Cronbach's Alpha of 0.82 (Miguel-Tobal, Casado, Cano-Vindel, & Spielberger, 2001). In Colombia, an exploratory factorial analysis found eight factors, two of which correspond to the two subscales of the anger trait, although some subscale items did not load in the two factors mentioned. The analysis also reported alphas higher than 0.79 for both factors, revealing an acceptable level for all subscales (Garcia-Padilla, Lara-Vargas, & Albarracín-Rodríguez, 2016). The Cronbach's Alpha in this study reached a good level: 0.89.
Procedure
All patients with an ischemic cardiopathy diagnosis confirmed by coronariography and admitted to hospital with acute coronary syndrome or who had been referred to a cardiac rehabilitation unit following a cardiac event were invited to take part in the study. Those who accepted the invitation and that fulfilled the inclusion criteria signed the informed consent form and completed the assessment protocol. The assessment took around 40 minutes. It is worth noting that this study was approved by the ethics committees at the two institutions where the research was carried out and by the ethics committee at Universidad de los Andes.
Statistical analysis
The statistical analyses initially consisted of obtaining the scores for each of the administered subscales and scales, and their reliability indices. Exploratory factorial analyses (EFA) were carried out to verify the existence of factorial components proposed by Spielberger in each of the tests. The EFA were interpreted after verifying the value of the Kaiser-Mayer-Olikin (KMO) measure of sampling adequacy and Bartlett's sphericity test. A significant Bartlett's test indicates that the data are intercorrelated meaning that applying an EFA is suitable. This coincides with the analysis of the value of the KMO measure of sampling adequacy where a value above 0.7 indicates a satisfactory interrelation between the items (Perez & Medrano, 2010).
Subsequently, a confirmatory factor analysis (CFA) was carried out to confirm the existence of a latent factor that grouped the variance shared among the scores for depression, anxiety, and anger-hostility. In the CFA, variables were created that represent the total subscale through parcelling, as has been recommended in cases where the number of subjects is not high, or when there are problems of non-normality of indicators. This method generates indicators of greater reliability given that the variables are constructed based on a high degree of communality, there is less probability of violations in the distributions, and there are fewer parameters to estimate (Little, Rhemtulla, Gibson, & Schoemann, 2013). To scale the latent variable the variance of the latent variable was fixed at one. The advantage of this method is that it allows for the factorial load of all the indicators to be freely estimated (Byrne, 2012; Kline, 2010). MLR (Maximum Robust Likelihood) was used due to the fact that some of the data did not distribute normally.
To assess the model of adjustment, the following indices were evaluated: X2, CFI (Comparative Fit Index), TLI (Tucker-Lewis Index), RMSEA (Root Mean Square Error of Approximation), and SRMSR (Standardised Root-Mean-Square Residual) bearing in mind that X2 was not to be significant, the indices CFI and TLI had to be higher than 0.95, RMSEA and SRMSR lower than 0.05 for a good fit (Kline, 2010). The analyses were carried out in SPSS version 23.0 and in MPlus version 7 (Muthén & Muthén, 2010).
RESULTS
Exploratory factorial analysis
The EFA of the depression trait scale produced values that meant that it was possible to interpret the factorial analysis, KMO = 0.80, Bartlett X2 (45) = 619.82, p < 0.01. The explained variance was of 57.5% and two factors were obtained, that corresponded to the dysthymia and euthymia scales, through a promax rotation (See Table 2).
Table 2 Exploratory factor analysis of the depression trait subscale
| Factor | Items | Communality | Explained variance |
| Dysthymia | 2 | .863 | 39.45 |
| 6 | .666 | ||
| 7 | .460 | ||
| 8 | .872 | ||
| 9 | .741 | ||
| Euthymia | 1 | .786 | 18.05 |
| 3 | .821 | ||
| 4 | .839 | ||
| 5 | .689 | ||
| 10 | .702 |
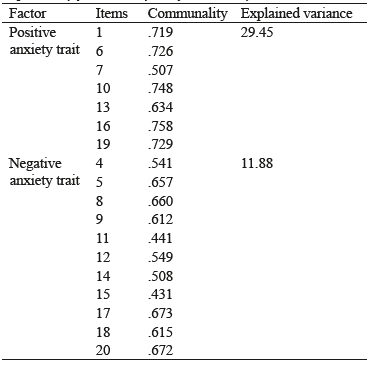
The EFA with the items belonging to the anxiety trait scale initially produced a five-factor solution. By forcing the solution to a maximum of two factors, the explained variance was found to be of 53.05%. The communalities of the items were affected by forcing the solution, and so were eliminated from the factor analysis sequentially beginning by those of less value. Finally, a two-factor model was obtained in an exploratory factor analysis which gave a KMO of 0.86 and Bartlett test of X1 (55) = 555.66, p < 0.001. The explained variance was of 41.3% (See Table 3).
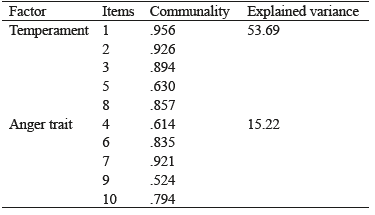
Finally, with respect to the EFA of the anger trait test, the KMO value was of 0.88 and the Bartlett sphericity test was of X1 (45) =1118.12, p < 0.01. The explained variance was of 67.8% and two factors were obtained using promax rotation. The factors found corresponded to the STAXI-2 subscales of temperament and angry reaction (See Table 4).
Confirmatory factor analysis
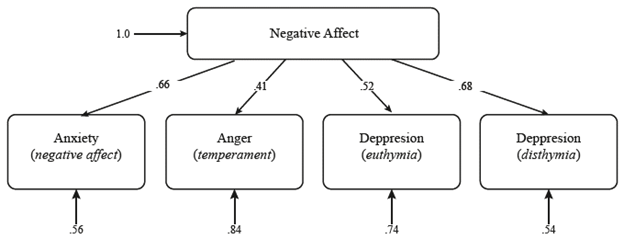
Following the verification of the factorial structure of the scales, they were all scaled in the same range of scores in order to apply CFA to verify the existence of the latent factor of negative affect. Following the verification of the factorial structure of the scales, it was proceeded to scale all of them in the same range of scores to apply a CFA aimed at verifying the existence of the latent factor of negative affect. Different models were used for the CFA constructed based on the subscales found with the exploratory factor analysis. The first model included the six subscales of each one of the tests. As the model did not fit correctly, new models were evaluated that did not include the anger reaction (model 2) and temperament (model 3) scales. Following this, the positive anxiety component was eliminated (model 4). The final model reveals that negative affect is the latent factor that includes the indicators for temperament and anger, the negative factor of anxiety and both depression components (euthymia and dysthymia). The final model presented an acceptable fit, X2 = 3.42, p > 0.05; CFI > 0.95, TLI > 0.95, RMSEA > 0.05, SRMS < 0.05 (See Table 5).
Table 5 CFA adjustment indices for the negative affect model
| X2 (sig) | d.f. | Akaike | TLI | CFI | SRMR | RMSEA | RMSEA IC 90% | |
| Model 1 | 169.60 (0.00) | 9 | 1755.75 | 0.025 | 0.385 | 0.106 | 0.317 | 0.277-0.360 |
| Model 2 | 39.94 (0.00) | 5 | 1315.35 | 0.613 | 0.807 | 0.061 | 0.199 | 0.144-0.258 |
| Model 3 | 71.76 (0.00) | 5 | 1312.97 | 0.262 | 0.631 | 0.087 | 0.275 | 0.220-0.333 |
| Model 4 | 3.42 (0.18) | 2 | 1062.80 | 0.955 | 0.985 | 0.043 | 0.063 | 0.000-0.175 |
Note: d.f.: degrees of freedom, TLI: Tucker-Lewis Index, CFI: Comparative Fit Index, SRMR: Standardised root-Mean-Square Residual, RMSEA: Root Mean Square Error of Approximation.
Figure 1 illustrates the diagram of the final model for positive and negative affect which shows the standardised coefficients between the summary indicators and the latent variable (negative affect) that oscillate between 0.41 and 0.68.
DISCUSSION
This study found that the negative affect is the common factor between depression, anxiety and anger traits. It also verified the factorial structure of the trait scales of the tests created by Spielberger to measure depression (Spielberger, Buela-Casal & Agudelo, 2008), anxiety (Spielberger, Gorsuch & Lushene, 1970), and anger (Miguel-Tobal, Casado, Cano-Vindel, & Spielberger, 2001). The results for the factorial structure of both depression and anger are consistent with the findings reported in studies on the validation of Spielberger's tests in Spanish (Miguel-Tobal et al., 2001; Spielberger et al., 2008). However, in the case of anxiety, the factorial structure did not reveal the existence of just one factor as described in the manual for its validation in Spanish (Spielberger et al., 1999) but rather that the structure corresponded to the direct and inverse STAI scores, and to the subscales of positive anxiety trait and negative anxiety trait in other studies (Fonseca-Pedrero, Paino, Sierra-Baigrie, Lemos-Giráldez, & Muñiz, 2012). Previous studies have shown one- and two-factor factorial structures, although the number of factors was forced or items with communality below 0.4 were kept (Fonseca-Pedrero et al., 2012; Vera-Villarroel et al., 2008).
The existence of negative affect as a latent factor had been reported in the clinical population in original studies by Watson and Clark in relation to depression and anxiety, and in subsequent studies in the same line (Clark & Watson, 1988; Simms, Grös, Watson, & O'Hara, 2008; Watson & Clark, 1992; Watson & Walker, 1996). The assessment of the relationship of depression and anxiety with the anger trait had already been shown in healthy population (Bleil, Gianaros, Jennings, Flory, & Manuck, 2008). For the population with CVD, there are no data of other studies that have shown the existence of the construct, although high levels of comorbidity between anxiety and depression have been reported (Polikandrioti & Olympios, 2014; Watkins et al., 2013).
In the confirmatory factor analysis for the verification of the existence of negative affect, it was found that both components of the depression trait of the ST-DEP test loaded for this factor. This may be explained by the fact that the test focuses on the affective component of depression rather than its physiological or cognitive symptoms (Spielberger et al., 2008). These results are not inconsistent with the fact that depression would be made up by high negative affect (dysthymia) and a low positive affect (euthymia) (Boehm & Kubzansky, 2012). However, it does allow us to infer that the negative affect factor found here, would include both aspects of affectivity in depression, as well as the emotional discomfort of anxiety and anger. It is worth noting that these results are consistent with the study by Bleil et al. (2008), who found that negative affect explained 92.5% of the depression variance in the common factor found among these three emotions. In addition, it is possible that the distinction of depression into positive and negative affect may not be so useful in populations with CVD. A study involving patients that were going to be subjected to heart bypass surgery found a high level of overlapping between depression and anxiety. An additional factor was found for depression, which was denominated low positive affect, and one for anxiety, denominated somatic anxiety. However, neither of the two were better than the random in discriminating between the two disorders (Tully & Penninx, 2012).
The results of this study reveal the reasons behind why the chronic experience of depression symptoms seem to have a stronger and more consistent impact on atherosclerosis than a depressive episode. They explain why the gradient found between the magnitude of anger or depression and the risk of CVD is a dose-response relationship (Brunner et al., 2014). They also go in the same direction as studies carried out by Schott et al. (2009) on the relationship between the anger trait and major atherosclerotic risk or the results that point out that negative affect, measured as symptoms of depression, anxiety and anger are associated with higher blood pressure in healthy adults (Sanchez&Gonzalez, May, Koutnik, & Fincham, 2015). As such, identifying forms of discomfort, even at subsyndromal levels may provide an important pathway towards early intervention.
Negative affect may influence CVD through physiological and behavioural pathways. Physiological mechanisms include excessive activity of the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis (HPA), leading to platelet activation, an exaggeration of cardiovascular reactivity and systemic inflammation (Chauvet-Gelinier & Bonin, 2017; McEwen, Nasveld, Palmer, & Anderson, 2012). Behavioural mechanisms could also be given through association with unhealthy habits such as smoking, excessive drinking, sedentary lifestyles, and non-compliance with medical interventions (Karaslavova, Dyakova, Todorova, & Tufkova, 2009; Penninx, 2017; Reddy, Dunbar, Morgan, & O'Neil, 2008). Also, negative affect may help us understand why chronic emotions are enough to motivate potentially risky behaviour to alleviate discomfort in the short term. However, when such behaviours become habits, they only provide temporary relief and are not able to reduce cognitions or modify the negative affect. As such, the risk of CDV can be understood as being based on low levels of chronic stress (Kubzansky et al., 2005).
Finally, the results of this study are in line with the idea that emotional alterations are prevalent in almost all types of psychopathology (Bloch, Moran, & Kring, 2010; Werner & Gross, 2010). A dimensional model in the understanding of emotions in patients with CVD responds to the call to assess the potential efficiency of psychotherapy and the cost-effectiveness of carrying out a transdiagnostic assessment that points to the common factor between anxiety and depression (Tully & Penninx, 2012).
In sum, this study confirms the existence of negative affect as a latent factor of depression, anxiety and anger traits. And the development of studies focusing on this point rather than on discrete emotions, have the potential to respond to the call made subsequently for intervention studies involving this population which highlight that cardiovascular risk may be the result of an association of typical depressive symptoms with other conditions that have not so far been considered (Rafanelli, Sirri, Grandi, & Fava, 2013).
REFERENCES
Agudelo, D. M., Gómez, Y., & López, P. L. (2014). Propiedades psicométricas del Inventario de Depresión Estado/Rasgo (IDER) con una muestra de población general colombiana. Avances en Psicología Latinoamericana, 32(1), 71-84. doi:10.12804/apl32.1.2014.05. [ Links ]
Alarcón, R., & Ramírez, E. (2006). Medicina psicosomática en enfermedad cardiovascular: consideraciones clínicas. Revista Colombiana de Psiquiatria, 35, 112-124. [ Links ]
American Heart Association. (2010). Risk factors and Coronary Artery Disease. Recuperado de http://www.american-heart.org/presenter.jhtml?identifier=4726. [ Links ]
American Psychiatric Association. (2013). Diagnostic andStatistical Manual of Mental Disorders, Fifth Edition ( DSM 5 ). Arlington, VA: American Psychiatric Association. [ Links ]
Bleil, M. E., Gianaros, P. J., Jennings, J. R., Flory, J. D., & Manuck, S. B. (2008). Trait negative affect: toward an integrated model of understanding psychological risk for impairment in cardiac autonomic function. Psychosomatic Medicine, 70(3), 328-337. [ Links ]
Bloch, L., Moran, E. K., & Kring, A. M. (2010). On the need for conceptual and definitional clarity in emotion regulation research on psychopathology. En A. M. King & D. M. Sloan (Eds.), Emotion Regulation and Psychopathology. A Transdiagnostic Approach to Etiology and Treatment (pp. 88-104). New Yourk: The Guilford Press. [ Links ]
Boehm, J. K., & Kubzansky, L. D. (2012). The heart's content: The association between positive psychological well-being and cardiovascular health. Psychological Bulletin, 138(4), 655-691. doi: 10.1037/a0027448. [ Links ]
Brown, T. A., & Barlow, D. H. (2009). A proposal for a dimensional classification system based on the shared features of the DSM-IV anxiety and mood disorders: implications for assessment and treatment. Psychological assessment, 21(3), 256. [ Links ]
Brunner, E. J., Shipley, M. J., Britton, A. R., Stansfeld, S. A., Heuschmann, P. U., Rudd, A. G.,... Kivimaki, M. (2014). Depressive disorder, coronary heart disease, and stroke: doseresponse and reverse causation effects in the Whitehall II cohort study. European journal of preventive cardiology, 21(3), 340-346. doi:10.1177/2047487314520785. [ Links ]
Byrne, B. M. (2012). Structural Equation Modeling with M-Plus. New York: Routledge. [ Links ]
Celano, C. M., Suarez, L., Mastromauro, C., Januzzi, J. L., & Huffman, J. C. (2013). Feasibility and Utility of Screening for Depression and Anxiety Disorders in Patients With Cardiovascular Disease. Circulation: Cardiovascular Quality and Outcomes,6, 498-504. doi: https://doi.org/10.1161/CIRCOUTCOMES.111.000049. [ Links ]
Chauvet-Gelinier, J. C., & Bonin, B. (2017). Stress, anxiety and depression in heart disease patients: A major challenge for cardiac rehabilitation. Annals of Physical and Rehabilitation Medicine, 60(1), 6-12. doi: https://doi.org/10.1016/j.rehab.2016.09.002. [ Links ]
Chida, Y., & Steptoe, A. (2009). The association of anger and hostility with future coronary heart disease: a meta-analytic review of prospective evidence. Journal of the American College of Cardiology, 53(11), 936-946. doi:10.1016/j.jacc.2008.11.044. [ Links ]
Clark, L. A. (2005). Temperament as a unifying basis for personality and psychopathology. Journal of Abnormal Psychology, 114(4), 505-521. doi:10.1037/0021-843X.114.4.505. [ Links ]
Clark, L. A., & Watson, D. (1988). Mood and the mundane: Relations between daily life events and self-reported mood. Journal of Personality and Social Psychology, 54(2), 296-308. doi:10.1037/0022-3514.54.2.296. [ Links ]
Denollet, J., & Pedersen, S. S. (2009). Anger, depression, and anxiety in cardiac patients: the complexity of individual differences in psychological risk. Journal of the American College of Cardiology , 53(11), 947-949. doi:10.1016/j.jacc.2008.12.006. [ Links ]
Fonseca-Pedrero, E., Paino, M., Sierra-Baigrie, S., Lemos-Giráldez, S., & Muñiz, J. (2012). Propiedades psicométricas del Cuestionario de ansiedad estado-rasgo (STAI) en universitarios. Behavioral Psychology-Psicología Conductual, 20(3), 547-561. [ Links ]
Garcia-Padilla, A. K., Lara-Vargas, E. J., & Albarracín-Rodríguez, A. P. (2016). Análisis Psicométrico del Staxi-2 Y Ml-Staxi en Adultos del Área Metropolitana de Bucaramanga. Cuadernos Hispanoamericanos de Psicología, 16(2), 33-44. [ Links ]
Guyton, A. C., & Hall, J. E. (2006). Fisiologia médica. España: Elsevier. [ Links ]
Karaslavova, E., Dyakova, M., Todorova, D., & Tufkova, S. (2009). Psychosomatic correlates of coronary heart disease during the socio-economic crisis of post-communist Bulgaria. Central European Journal of Medicine, 4(1), 91-97. doi:10.2478/s11536-008-0078-y. [ Links ]
Kline, R. (2010). Principles and practice of structural equation modeling. New York: The Guilford Press. [ Links ]
Kubzansky, L. D., Davidson, K. W., & Rozanski, A. (2005). The clinical impact of negative psychological states: expanding the spectrum of risk for coronary artery disease. Psychosomatic Medicine , 67(Supplement 1), S10-S14. doi:10.1097/01.psy.0000164012.88829.41. [ Links ]
Kubzansky, L. D., & Kawachi, I. (2000). Going to the heart of the matter:do negative emotions cause coronary heart disease? Journal of Psychosomatic Research, 48(4-5), 323-337. doi:10.1016/S0022-3999(99)00091-4. [ Links ]
Kubzansky, L. D., & Thurston, R. C. (2007). Emotional vitality and incident coronary heart disease: benefits of healthy psychological functioning. Archives of General Psychiatry, 64(12), 1393-1401. doi:10.1001/archpsyc.64.12.1393. [ Links ]
Lanas, F., Avezum, A., Bautista, L. E., Diaz, R., Luna, M., Islam, S., & Yusuf, S. (2007). Risk factors for acute myocardial infarction in Latin America. Circulation, 115(9), 1067-1074. doi:10.1161/CIRCULATIONAHA.106.633552. [ Links ]
Lichtman, J. H., Froelicher, E. S., Blumenthal, J. A., Carney, R. M., Doering, L. V., Frasure-Smith, N.,... Wulsin, L. (2014). Depression as a Risk Factor for Poor Prognosis Among Patients With Acute Coronary Syndrome: Systematic Review and Recommendations: A Scientific Statement From the American Heart Association. Circulation, 129(12), 1350-1369. doi:10.1161/CIR.0000000000000019. [ Links ]
Little, T. D., Rhemtulla, M., Gibson, K., & Schoemann, A. M. (2013). Why the items versus parcels controversy needn't be one. Psychological Methods, 18(3), 285-300. doi:10.1037/a0033266. [ Links ]
McEwen, B. S., Nasveld, P., Palmer, M., & Anderson, R. (2012). Allostatic Load. A Review of the Literature. Australia: Department of Veteran's Affairs. [ Links ]
Miguel-Tobal, J. J., Casado, M. I., Cano-Vindel, A., & Spiel-berger, C. D. (2001). Manual del Inventario de Expresión de Ira Estado-Rasgo (STAXI-2). Madrid: TEA Ediciones. [ Links ]
Ministerio de Salud y Protección Social. (2016). Análisis de Situación de Salud. Colombia. Bogotá: Imprenta Nacional de Colombia. [ Links ]
Moriondo, M., Palma, P., Medrano, L., & Murillo, P. (2011). Adaptación de la Escala de Afectividad Positiva y Negativa (PANAS) a la población de Adultos de la ciudad de Córdoba: Análisis Psicométricos Preliminares. Universitas Psychological, 11(1), 187-196. [ Links ]
Moser, D. K., McKinley, S., Riegel, B., Doering, L. V., Meischke, H., Pelter, M.,... Dracup, K. (2011). Relationship of Persistent Symptoms of Anxiety to Morbidity and Mortality Outcomes in Patients With Coronary Heart Disease. Psychosomatic Medicine , 73(9), 803-809. doi:10.1097/PSY.0b013e3182364992. [ Links ]
Muthén, L. K., & Muthén, B. O. (2010). Mplus User's Guide: Statistical Analysis with Latent Variables: User's Guide. Los Angeles: Muthén & Muthén. [ Links ]
Penninx, B. W. J. H. (2017). Depression and cardiovascular disease: Epidemiological evidence on their linking mechanisms. Neuroscience & Biobehavioral Reviews, 74(Parte B), 277-286. doi:https://doi.org/10.1016/j.neubio-rev.2016.07.003. [ Links ]
Perez, E. R., & Medrano, L. (2010). Análisis factorial exploratorio: bases conceptuales y metodológicas. Revista Argentina de Ciencias del Comportamiento, 2, 58-66. [ Links ]
Polikandrioti, M., & Olympios, C. (2014). Anxiety and coronary artery disease. Archives of Hellenic Medicine, 31(4), 403-411. [ Links ]
Posner, J., Russell, J. A., & Peterson, B. S. (2005). The circumplex model of affect: An integrative approach to affective neuroscience, cognitive development, and psychopathology. Development and psychopathology, 17(03), 715-734. doi:10.1017/S0954579405050340. [ Links ]
Rafanelli, C., Sirri, L., Grandi, S., & Fava, G. A. (2013). Is Depression the Wrong Treatment Target for Improving Outcome in Coronary Artery Disease? Psychotherapy andpsychosomatics, 82(5), 285-291. doi:10.1159/000351586. [ Links ]
Reddy, P., Dunbar, J. A., Morgan, M. A. J., & O'Neil, A. (2008). Coronary heart disease and depression: getting evidence into clinical practice. Stress and health, 24(3), 223-230. doi:10.1002/smi.1201. [ Links ]
Robles, R., & Páez, F. (2003). Estudio sobre la traducción al español y las propiedades psicométricas de las escalas de afecto positivo y negativo (PANAS). Salud mental, 26(1), 69-75. [ Links ]
Sanchez-Gonzalez, M. A., May, R. W., Koutnik, A. P., & Fincham, F. D. (2015). Impact of negative affectivity and trait forgiveness on aortic blood pressure and coronary circulation. Psychophysiology, 52, 296-303. doi:10.1111/psyp.12325. [ Links ]
Sandín, B., Chorot, P., Lostao, L., Joiner, T. E., Santed, M. A., & Valiente, R. M. (1999). Escala PANAS de afecto positivo y negativo: validación factorial y convergencia transcultural. Psicothema, 11(1), 37-51. [ Links ]
Schott, L. L., Kamarck, T. W., Matthews, K. A., Brockwell, S. E., & Sutton-Tyrrell, K. (2009). Is brachial artery flow-mediated dilation associated with negative affect? International Journal of Behavioral Medicine, 16(3), 241-247. doi:10.1007/s12529-009-9038-4. [ Links ]
Simms, L. J., Grös, D. F., Watson, D., & O'Hara, M. W. (2008). Parsing the general and specific components of depression and anxiety with bifactor modeling. Depression and Anxiety, 25(7), E34-E46. doi:10.1002/da.20432. [ Links ]
Smith, P. J., & Blumenthal, J. A. (2011). Aspectos psiquiátricos y conductuales de la enfermedad cardiovascular: epidemiología, mecanismos y tratamiento. Revista Española de Cardiología, 64(10), 924-933. doi:10.1016/j.recesp.2011.06.003. [ Links ]
Spielberger, C. D., Buela-Casal, G., & Agudelo, D. M. (2008). IDER, inventario de depresión estado-rasgo: Manual. Madrid: TEA Ediciones. [ Links ]
Spielberger, C. D., Gorsuch, R. L., & Lushene, R. E. (1970). Handbook of STAI. Palo Alto: CA: Consulting Psychologist Press [Adaptación al español: Seisdedos, N.(1988) Barcelona: TEA Ediciones]. [ Links ]
Spielberger, C. D., Gorsuch, R. L., Lushene, R. E., & Seisdedos, N. (1999). STAI: Cuestionario de ansiedad estado-rasgo. Madrid: TEA Ediciones . [ Links ]
Torquato Jr, M. A. A., de Souza, B. P. F., Iosifescu, D. V., & Fraguas, R. (2012). Anger, Hostility and Other Forms of Negative Affect: Relation to Cardiovascular Disease. En M. Atiq (Ed.), Recent Advances in Cardiovascular Risk Factors (pp. 415-436). Sao Paulo, Brasil: INTECH Open Access Publisher. [ Links ]
Tully, P. J., & Penninx, B. W. (2012). Depression and Anxiety Among Coronary Heart Disease Patients: Can Affect Dimensions and Theory Inform Diagnostic Disorder-Based Screening? Journal of clinical psychology, 68(4), 448-461. doi:10.1002/jclp.21828. [ Links ]
Vera-Villarroel, P., Buela-Casal, G., Celis-Atenas, K., Córdova-Rubio, N., Encina-Olea, N., & Spielberger, C. D. (2008). Chilean experimental version of the State-Trait Depression Questionnaire (ST-DEP): Trait sub-scale (T-DEP). International Journal of Clinical and Health Psychology, 8(2), 563-575. [ Links ]
Watkins, L. L., Koch, G. G., Sherwood, A., Blumenthal, J. A., Davidson, J. R. T., O'Connor, C., & Sketch, M. H. (2013). Association of Anxiety and Depression With All-Cause. Mortality in Individuals With Coronary Heart Disease. Journal of the American Heart Association, 2(2), e000068. doi:10.1161/JAHA.112.000068. [ Links ]
Watson, D., & Clark, L. A. (1992). Affects separable and inseparable: On the hierarchical arrangement of the negative affects. Journal of Personality and Social Psychology , 62(3), 489 - 505. doi:10.1037/0022-3514.62.3.489. [ Links ]
Watson, D., Clark, L. A., & Carey, G. (1988). Positive and negative affectivity and their relation to anxiety and depressive disorders. Journal of Abnormal Psychology, 97(3), 346. doi:10.1037/0021-843X.97.3.346. [ Links ]
Watson, D., Clark, L. A., & Stasik, S. (2011). Emotions and the emotional disorders: a quantitative hierrarchical perspective. International Journal of clinical and Health Psychology, 11(3), 429 - 442. Recuperado de http://www.redalyc.org/html/337/33719289001/. [ Links ]
Watson, D., Clark, L. A., & Tellegen, A. (1984). Cross-cultural convergence in the structure of mood: A Japanese replication and a comparison with US findings. Journal of Personality and Social Psychology , 47(1), 127-144. doi:10.1037/0022-3514.47.1.127. [ Links ]
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: the PANAS scales. Journal of Personality and Social Psychology , 54(6), 1063-1070. doi:10.1037/0022-3514.54.6.1063. [ Links ]
Watson, D., & Walker, L. M. K. (1996). The long-term stability and predictive validity of trait measures of affect. Journal of Personality and Social Psychology , 70(3), 567-577. [ Links ]
Werner, K., & Gross, J. J. (2010). Emotion Regulation and Psychopathology. En A. M. Kring & D. M. Sloan (Eds.), Emotion Regulation and Psychopathology. A Transdiagnostic Approach to Etiology and Treatment (pp. 13-37). New York: The Guilford Press . [ Links ]
WHO. (2011). Global atlas on cardiovascular disease prevention and control 2011 (S. Mendis, P. Puska, & B. Norrving Eds.). France: WHO Press. [ Links ]
Yusuf, S., Hawken, S., Ôunpuu, S., Dans, T., Avezum, A., Lanas, F.,... Varigos, J. (2004). Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. The Lancet, 364(9438), 937-952. doi:10.1016/S0140-6736(04)17018-9. [ Links ]
Referencia: Lemos, M. & Agudelo-Vélez, D.M. (2018). El afecto negativo como factor emocional de orden superior en pacientes cardiovasculares. Acta colombiana de Psicología, 21(2), 78-87. doi: http://www.dx.doi.org/10.14718/ACP.2018.21.2.4
Received: July 23, 2017; Revised: November 17, 2017; Accepted: November 23, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
