











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Introduction
Traumatic events involve confrontation with interpersonal violence, natural disasters, sudden loss, war, serious illness, and other disturbing events. In other words, traumatic events are situations representing a danger or any threat to physical integrity and can be single, type one, when they are occasional, or type two, when they are repeated and/ or cumulative (Perrotta, 2019). In addition to the above, a traumatic experience can occur at any age, childhood, adolescence, and adulthood. Thus, psychological trauma is a stressor that exceeds an individual's coping resources, meaning, that it surpasses the person's ability to deal with the event and triggers physical and psychological responses (Pole et al., 2016).
The types of traumatic events that can be experienced are varied, however it should be noted that man-made traumas are different from natural disasters. How survivors of natural trauma respond to the experience often depends on the degree of devastation, the magnitude of individual and community losses, and the time it takes to re-establish daily-life activities at the individual and collective level. In terms of intentional trauma, the survivor's subsequent reactions often depend on the intentionality of the perpetrator (U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Substance Abuse Treatment, 2014).
Thus, traumatic experiences have been related to physical and mental health problems, such as internalizing and externalizing symptoms. For example, feelings of emptiness and despair, hostility and derealization, depression, anxiety, irritability, emotional dysregulation problems, loss of coherence in self-representation, substance use, etc. (Kucharska, 2017; Perrotta, 2019). The most common diagnosis associated with trauma are post-traumatic stress disorder (PTSD), characterized by the presence of avoidance symptoms, negative alterations in cognition, intrusions, and arousal (Ford et al., 2012), or complex post-traumatic stress disorder (c-PTSD) characterized by the presence of re-experiencing, avoidance and hyperarousal (Courtois, 2004).
Traumatic events have a high incidence in the general population. The World Mental Health Surveys conducted with adult population have shown that among 70 000 participants from 24 high and low-income countries, 70.4% of respondents had experienced at least one type of traumatic event at some point in their lives (Kessler et al., 2017). In countries such as the United States of North America, it occurs in 50%, in Mexico in 68%, in Chile in approximately 40% (Medina-Mora et al., 2005; Perkonigg et al., 2000); however, studies about trauma in Ecuador are quite scarce.
Among the studies carried out in the Ecuadorian context is that of Valdez et al. (2016), carried out with women, which found a prevalence of PTSD of 4.6%, and the types of abuse experienced were: psychological, 53.9%; physical, 38.0%; sexual, patrimonial, 35.3%; domestic violence, 76.0%; and other types of violence, 24.0%. Another study conducted by Eckhardt et al. (2018) with Ecuadorian university students found that the prevalence of potentially traumatic experiences is very high, but that the low prevalence of dissociation suggested a high resilience in the study population. The authors suggested carrying out studies in populations with less access to resources.
Studies on trauma in prison settings have mostly been carried out in North America and Europe. These studies have shown a higher frequency of traumatic experiences as well as the presence of a greater number of mental disorders in incarcerated people than in the general population (Fazel et al., 2016; Prins, 2014). In Latin America, there is little research related to trauma in prison contexts. A study conducted in a female prison in Mexico found that traumatic experiences such as sexual and physical abuse are a key contributing factor to behavioral problems in adolescence and later delinquency, substance abuse, and crime in adulthood (Mejia et al., 2015). However, in the Ecuadorian prison context, studies on trauma are scarse.
The literature review explains that experiencing a single traumatic event is detrimental to mental health. However, recent research has found that exposure to multiple traumatic events increases the risk of psychopathology in both the general population and the prison population (Brown et al., 2014; Fink, & Galea, 2015; Schalinski et al., 2016), but with a higher prevalence of multiple traumas in the prison population (Baranyi et al., 2018; Karatzias et al., 2018).
General population samples tend to report relatively less exposure to trauma and a similarly lower incidence of PTSD (Breslau, 2002). In contrast, prison samples tend to have a greater history of traumatic experiences occurring at a younger age and lasting a longer period (Facer-Irwin et al., 2019; Foy et al., 2012; Wolff & Shi, 2012), higher rates of PTSD (Goff et al., 2007), other types of symptoms and psychopathological disorders (Green et al., 2016; Wolff & Shi, 2010).
Regarding the age of occurrence of traumatic events, episodes that occur at an early age have more significant effects on the development of mental health problems in the general population and prison population (Chapman et al., 2007). But with a higher prevalence in the prison population (Wolff & Shi, 2012). In this sense, Read et al. (2014) point out that the functioning of the brain changes after exposure to trauma during childhood and these biological factors can lead to physical and mental health problems in adulthood. Traumatic events such as interpersonal violence (assault, physical abuse, sexual abuse, kidnapping and / or stalking, and a relative friend being killed or committing suicide) can be a risk factor for revictimization in adulthood (Giarratano et al., 2020). In addition, it increases the risk of suffering mental health problems (Wolff & Shi, 2012).
Although public health strategies are aimed to prevent or reduce mental health problems at the individual, family, community, and social levels, unfortunately, attention given specifically to psychological trauma is a very limited area (Magruder et al., 2017). In this sense, if the approach to psychological trauma in the general population is not entirely adequate, the situation in the prison population is even more scarce and it is necessary to consider that, in this population, the history of traumatic events, particularly events occurring at an early age are more frequent (Cabeldue et al., 2019) and have a greater impact at the psychopathological level than in the general population (Foy et al., 2012; Wolff & Shi, 2012). In this sense, two questions have been raised for this study:
Are there differences between the prison population and the general population regarding the types of traumatic experiences, age of occurrence of traumatic events, PTSD and the number of traumas experienced? Are there differences between the prison population and the general population's psychopathological symptoms considering the number of traumas and the age of occurrence of traumatic events?
Method
Participants
For the prison population, the following inclusion criteria were established: (a) being able to read and write, (b) not being in pre-trial detention. In the case of the general population, the inclusion criteria were (a) being able to read and write, (b) residing in the same city where the prison is located. Taking these criteria into consideration, two groups were formed; the first was made up of 99 incarcerated individuals (49 men, 50 women), and the second, of 84 individuals from the general population (43 men, 41 women).
Instruments
Sociodemographic characteristics questionnaire A short questionnaire created ad hoc by the study's first author was used. Personal information such as gender, marital status, socio-economic status, educational background, and nationality was collected.
Traumatic Experiences Questionnaire (TQ)
The Spanish version of the questionnaire was used (Davidson & Smith, 1990). It is a self-administered screening instrument that assesses traumatic experiences and post-traumatic stress disorder. It consists of three parts: The first part is a list of traumatic experiences: 18 items to which one has to answer whether or not one has suffered traumatic experiences at some point in life and, if so, at what age and for how long. In this study, only 16 items were taken into account because two types of traumatic experiences do not apply to the context. The second part consists of 9 items assessing the characteristics of this event to see if it meets the requirements specified in diagnostic criterion A.
Finally, the third part consists of 18 items exploring the symptoms appearing in criteria B-D. The items are dichotomous (yes or no). It also consists of two additional items that are not part of the Scale, but provide information about health care. The alpha coefficient is .99 for the full scale, .97 for the frequency of traumatic events subscale, and .98 for the severity subscale (Bobes et al., 2000). In the Ecuadorian population, the alpha coefficient is .87 for the full scale (Molina-Coloma et al., 2022).
Symptom Checklist-90-Revised (SCL-90-R)
The Spanish version of González de Rivera et al. (2002) was used as a self-report instrument to measure 90 psychological symptoms, as well as psychological distress. The SCL-90-R sub-scales: Somatization, Obsessive Compulsive, Interpersonal Sensitivity, Depression, Anxiety, Hostility, Phobic Anxiety, Paranoid Ideation, and Psychoticism (Ruiz-Martínez et al., 2020). Each item has five response categories: not at all (0), little (1), somewhat (2), very (3), severe (4).
It also presents three general indices: Index of General Symptoms (IGS), Total Positive Symptoms (TPS) and Distress Index (ISD). González de Rivera et al. (2002) indicate that this instrument has a high internal consistency, with values ranging between . 81 and .90, and test-retest reliability coefficients between .78 and .90. In the Ecuadorian population, the alpha coefficient was .95 (Molina Coloma et al., 2018).
Procedure
The research design complied with the ethical standards and the code of behavior of the American Psychological Association (APA, 2017) which implied responsibility and respect for the dignity of the person. An informed consent was given to each of the participants from both populations, with the purpose of the research, expected duration, and procedures, their right to decline to participate and to withdraw from the research once participation has begun, any prospective research benefits; confidentiality; whom to contact for questions about the research and research participants' rights with a minimum level of risk (Aarons, 2017).
To recruit participants from the prison population, the first author of this paper requested permission from the penitentiary. After obtaining the permit, the aim of the study and the place where it would be carried out was explained to them.
To recruit participants from the general population, an announcement was made at the city hall of Ambato in Ecuador, explaining the objective and type of study, the parameters of participation, and the location where the evaluation would be carried out. Written informed consent was obtained from all participants (general prison population). The assessment was then conducted individually in a semi-structured interview and the instruments were administered in a one-and-a-half-hour session by the first author of the study.
Statistical analysis
The analyzes were carried out with the Statistical Package for the Social Sciences -SPSS- (version 24.0). The chi-square test was performed to compare the prison and general population groups in terms of types of traumatic experiences, number of traumas, age of occurrence of the traumatic event and PTSD. The Student's t-test was performed for the comparisons between a single trauma and multiple traumas with psychopathological symptoms. Additionally, this test was carried out to compare the age groups of occurrence of the traumatic event and the psychopathological symptoms. Age categories were created to classify the traumas and the number of traumas into age groups for the analysis.
Results
Table 1 describes the sociodemographic variables. In general, there are significant differences in nationality, educational level, and socioeconomic status. Regarding age and marital status, the characteristics are similar in both study groups.
Table 1 Differences in sociodemographic characteristics between prison population and general population
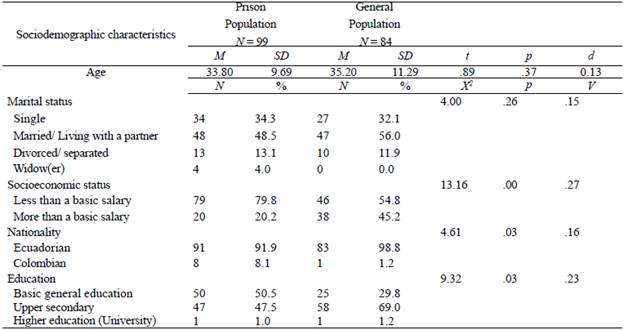
Note: M=Mean; SD=Standard deviation; d=Cohen's d
Table 2 shows that the prison population differs significantly from the general population in all types of traumatic events evaluated. Aggression (x2 = 53.51; p = .00; V = .54), physical abuse = 54.87; p = .00; V = .55), and other situations = 59.41; p = .00; V = .57) are the types of trauma with the largest effect sizes.
Table 2 Differences in traumatic experiences between prison population and general population
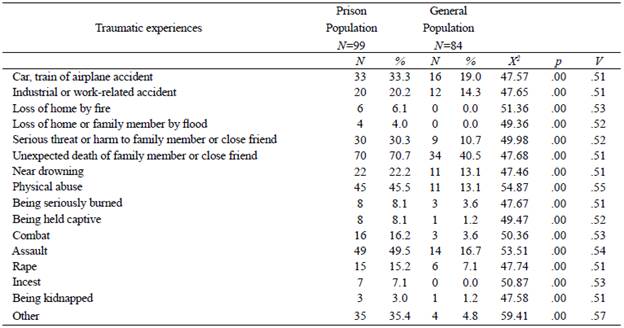
Note: X2=chi square; V=Cramer's V
Table 3 shows that there are significant differences between the two groups in the comparisons made. The presence of PTSD in the prison population is higher (26.3%) than in the general population (4.8%).
Table 3 Differences in the age of occurrence of the traumatic event and the number and type of traumas between the prison population and the general population

Note: X2=chi square; V=Cramer's V
Regarding the age of occurrence of traumatic events, it should be noted that in the group of people in the prison population 56.6% have been re-victimized while 41.7% of the general population has not experienced any trauma. On the other hand, 85.9% of the prison population has experienced multiple traumas throughout their lives, compared to the group of the general population which has experienced multiple traumas in a 40.5%.
In table 4, regarding the comparison between the number of traumas with psychopathological symptoms, in those who have experienced a single trauma, the differences between the two groups can only be observed in paranoid ideation (X2= 2.27; p = .03; V= .07). On the other hand, differences in the presence of multiple traumas can be observed in all symptoms except interpersonal sensitivity.
Table 4 Comparison between number of traumas and psychological symptoms in the prison population and the general population
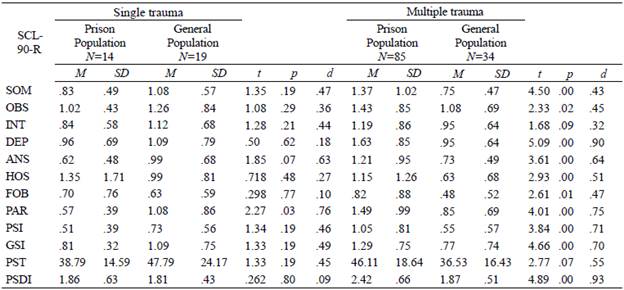
Note: M=Mean; SD=Standard deviation; d=Cohen's d
Those symptoms with large difference size are depression (t = 5.09; p =.00; d =.09), PSDI (t = 4.89; p =.00; d =.09), global severity index (t = 4.66; p =.00; d =.07), paranoid ideation (t = 4.01; p =.00; d =.08), and psychoticism (t = 3.84; p =.00; d =.07).
In table 5, the comparison of both groups in traumatic events that occurred at ages below 18 years old, significant differences were observed in all symptoms except interpersonal sensitivity. The effect size stood out in anxiety (t = 4.31; p = .00; d = 1.84) and somatization (t = 3.58; p = .00; d = 1.52).
Table 5 Comparison between the prison population and the general population in the age of occurrence of traumatic events and psychopathological symptoms.
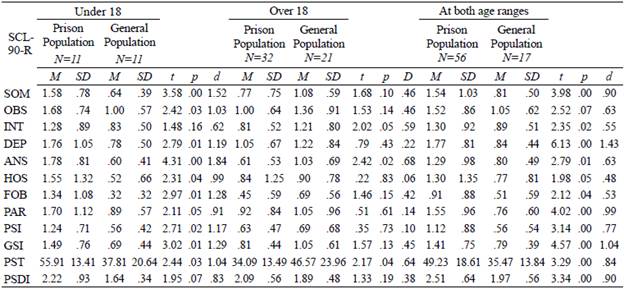
Note: M=Mean; SD=Standard deviation; d=Cohen's d
In the comparison of the two groups in terms of traumatic events that occurred at ages above 18 years old, significant differences were observed in two symptoms. The effect size stood out in interpersonal sensitivity (t = 2.02; p = .00; d = 0.59), anxiety (t = 2.42; p = .00; d = .68) and PTSD (t=2.17; p = .00; d = .64). Regarding the difference between groups in revictimization, the differences were significant in all symptoms. Particularly, the effect size was large in depression (t = 6.13; p = .00; d = 1.43), and in the global severity index (t = 4.57; p = .00; d = 1.04).
Discussion
In response to the research questions, there are differences between the prison population and the general population in terms of types of traumatic experiences, age of occurrence of traumatic events, PTSD and the number of traumas experienced. There are also differences regarding psychopathological symptoms between the prison population and the general population, considering the number of traumas and the age of occurrence and traumatic events.
The results of this study show that traumatic experiences, whether accidental, natural, or intentional, can be present in the everyday life of any individual. Thus, our results allow us to demonstrate how higher levels of vulnerability in the social life can promote lower levels of mental health among populations. Thus, in this research, it has been found that it is the group in prison that presents a higher prevalence related to intentional traumatic events, such as, for example, abuse or physical aggression, i.e., symptoms of greater severity in comparison with the general population that has reported experiencing accidental situations (accidental trauma), such as, for example, work or traffic accidents (Gunter et al., 2012; Komarovskaya et al., 2011; Salina et al., 2017)
Therefore, and following the line of argument, it is interesting to find that it was also the prison groups that had the higher levels of PTSD and psychopathological symptoms. Furthermore, this population presented higher levels of symptomatology, PTSD and psychopathological symptoms when they had experienced multiple traumatic events, which is consistent with previous studies (Abate et al., 2017; Baranyi et al., 2018; Karatzias et al., 2018). The latter may be explained by the age at which the traumatic event occurred (before the child was 18 years old). To this end, in the present study the group of people in prison who also referred to having suffered multiple traumas throughout life starting in childhood, have also been revictimized with a higher percentage of PTSD than that found in the general population (Facer-Irwin et al., 2019; Foy et al., 2012; Wolff & Shi, 2012). Considering the ages of occurrence of the traumatic event, it has also been shown that the general population has higher scores on traumatic experiences occurring at ages above 18 years, particularly on interpersonal sensitivity, anxiety and overall positive symptomatology.
Specifically, these results show an invisible reality about the mental health situation regarding the effects of trauma on the prison population. In this sense, these results can be explained, on the one hand, by the fact that reactions after trauma are affected by their own experiences, availability of support, access to a psychological care service, coping skills, and other individual characteristics; and on the other hand, because incarcerated persons may have a higher vulnerability to be laid open to potentially traumatic events, due to their own social, economic, and family situation, characterized by instability that may contribute to easy exposure to violent events (Añaños-Bedriñana, & Jiménez-Bautista, 2016).
Moreover, the vulnerability to which incarcerated individuals are exposed can occur both before and during their stay in prison. However, further research is required to better understand the nature of trauma. The results found in this work need to be extended in the future, for example, by identifying risk factors that are associated with situations that can be potentially traumatic and that are related to a greater presence of psychopathological symptoms. It is also important to analyze the relationship between trauma and criminal behavior, particularly multiple traumas, traumatic events at ages below 18 years, and intentional traumas, in order to identify their influence on criminal activity.
This study had some limitations, on the one hand, the use of retrospective information, which is always determined by the examinee's memory. On the other hand, the sample that was part of this study was small, which limits the generalisability of the results. An understanding of trauma exposure, and intentional trauma care and its association with mental health problems may facilitate the implementation of effective trauma-focused assessments in specific mental health care settings in the general population and, to a greater extent, in prison settings. In addition, it should be noted that both exposures to traumatic events and mental health problems are considered risk factors for criminal behavior, as has been demonstrated in the prison population (Dierkhising, 2013; Fox et al., 2015). In this sense, this study has practical implications, for example, for improving mental health levels in both the general population and the prison population and preventing criminal recidivism (Liu et al, 2021).

