











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Primary pulmonary coccidiodomycosis is usually a self limited illnes, the presenting as acute respirtaory failure is distinctly uncommon, and has been most frecuently associated with underlying inmunosupresive conditions, particulary steroid therapy and massive exposure to C immitis. The highest risk of coccidioidomycosis after solid organ transplant occurs in the first year posttransplant, accounting for as many as 70% of cases in one series, in areas of high endemicity, the risk of symptomatic posttransplant coccidioidomycosis is increased with history of prior infection, positive serology before transplant, or antirejection therapy, the dissemination is more common in transplant patients occurring in up to 75% of cases, mortality is reported to be from 30 % to 63 %.
Case description
A 59 year-old male post trasplant liver recipient presented to the emergency department complaining of abdominal pain, nausea, diarrhea and fever. The initial physical exam revealed his blood pressure was 100/62 mm Hg, heart rate of 125/min, temperature 100 °F, respiratory rate 27/min, and oxygen saturation 88 % on room air and 92% on 40% venti-mask, the heart exam revealed tachycardia but regular rhythm, a normal S1 and S2 and no murmurs, gallops or rubs. On auscultation of the lung fields, breath sounds were diminished without the presence of adventitious sounds. The abdomen was benign without organomegaly, extremities were normal with absence of clubbing or edema. The patient appeared in discomfort.
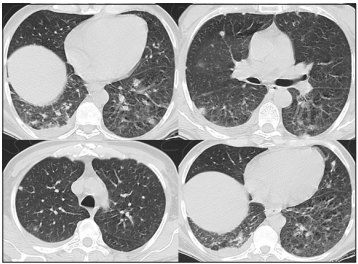
The white blood cell count was 5.5 (reference range 5.0 - 12.0 x 103), with 95% of neutrophils, the hemoglobin was 11.3 gr (reference range 13 - 15.7 gr/dl in men), the platelets count was 76 (reference range 150-450 K/ul). The serum creatinine was 0.94 mg/dl (reference range 0.6-1.2mg/dl), serum sodium was 127 mmol/L (reference range 135-145 mmol/L), serum potassium was 4.3 mmol/L (reference range 3.5-4.5 mmol/L). Serum albumine was 2.8 (reference range 3.4 to 5.4 g/dL) Total Bilirrubin 1.26 (reference range 1 to 1.2 mg/dL ) ALT 34 AST 29.50 (reference ranges for both 8-40 U/L). Arterial blood gas análisis reported pH 7.46 (7.35-7.45), paCO2 20.9 mmHg (reference range 35-45 mmHg), HCO3 14.4 mmol/L (reference range 22.2-28 mmol/L). Chest CT imaging revealed consolidation areas, multiple lung nodules and ground-glass areas (Figure 1).
Due to the suspicion of invasive fungal infection a bronchoalveolar lavage was requested, after bronchoscopy the patient condition worsened, needing mechaninal ventilation, vasopressor suport, transferred to the ICU due to severe respiratory failure, a chest X ray reveled lungs with bilateral difusse consolidation areas ( figure 2). The Arterial blood gas analysis reported pH: 7.06 PO2: 137 PCO2: 32 HCO3: 8.8 LACT: 8.76, Pa02/FiO2 ratio < 100. Upon admision to the critical care unit, the patient placed under mechanical ventilation pressure control mode and continue antibiotic therapy for adquirided comunity pneumonia in inmunocompromised patient, and amphotericn B was added, however the patient died 24 hours after his admission.

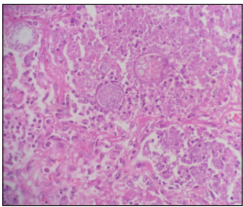
The bronchoalveolar lavage culture was negative for bacteria, but the fungus culture produced suspicious filamentous colonies, the cotton blue stain reveled thin and septate hyphae and arthroconidia. (figure 3 ). Post mortem macroscopic pieces shows a multiple nodular lesions in the lung and liver (figure 4), microscopic description has typical histologic features, granulomatous inflammation, large thick walled spherules contain variable sized daughter endospores. (figure 5).
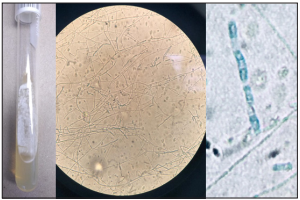
Figure 3 filamentous colonies, the cotton blue stain 40 x, reveled thin septate hyphae and arthroconidia.

Brief discusión
Acute respiratory distress syndrome (ARDS) is a respiratory process of acute onset, showing on X rays as bilateral pulmonary infiltrates and severe respiratory failure, disorders associated with ARDS include direct lesions of the pulmonary parenchyma and lesions indirectly affecting the lung occurs most often in the setting of pneumonia, sepsis, aspiration of gastric contents or severe trauma and is present in ~10% of all patients in intensive care units worldwide. Despite some improvements, mortality remains high at 30-40% in most studies1. Coccidiodomycosis is a unusual cause of acute respiratory distress syndrome.
Coccidiodomycosis is caused by the dimorfic fungi Coccidiodes immitis, is found in nature as a saprophytic filament (mould) that produces propagules (arthroconidia) which spread easily in the air, infection caused by Cocciodioides species occurs after inhalation of aerosolized arthroconidia, with the organism potentially becoming latent within resident and recruited pulmonary phagocytes and cells of the reticuloendothelial system, is endemic to areas of Southwestern United states, Northern Mexico and parts of Central and South America with particular presence in Argentina and Paraguay, are highly infectious to susceptible humans, presents variability of symptoms, 60-80% mild respiratory symptoms, 15 - 35% develop respiratory symptoms in 1 to 4 weeks, 5% will develop progressive symptoms, 1- 5 % disseminated forms, dissemination to any organ or tissue can occur, establishing secondary mycosis foci, the fungus can remain viable and latent at and cause clinical manifestation2),(3.
The present report describes a old man patient post trasplant liver recipient, no residing in the traditional areas of endemicity of C. Immitis, a immunocompromised host, with multiple risk factors for a disseminated disease such as age, gender, diabetes mellitus as concurrent immunosuppressing illness, use high-dose corticosteroid treatment and other immunosuppressant drugs tacrolimus and mycophenolate, and your previously labor activities to contact with contaminated dust, especially from uncultivated areas in endemic areas, his relatives comment in the past he works as a civil engineer as a construction operations supervisor in the northern región of Mexico, an endemic area of coccidiodomycosis, with the suspicion of exposure of airborne soil particles.
Coccidiodomycosis has been reported in solid organ trasplant (SOT) recipients since 1967, the diseases ocurrs in the first year after trasplant and the incidence of these patients in the endemic areas has been reported as 5 %4.
A recent coccidioidal infection or a positive serologic test result at the time of organ transplantation is associated with a rate of dissemination of 75% and a mortality of 30% to 63% without the use of antifungal prophylaxis5.
Coccidioidal disease in the immunocompromised host can result from primary infection or from reactivation of old infection. T-cell function deficiencies add the patient at risk for severe or disseminated infection. The receipt of anti-rejection medications or of tumor necrosis factor α inhibitors increases the risk of disseminated coccidioidal disease because of their effect on T-cell function6,7.
In solid organ transplantation is asocciated with reactivation of latent infection or primary infection in areas where it is a endemic. In the patient that we are presenting the suspicion is that the reactivation of latent coccidiodomycosis, is the most common probable cause form of the disease, which is the most frequent in transplanted patients, since the acquisition through the organ donor was ruled out.
Donor organs may be a source of transmissible agents, particularly viruses, has been a significant concern throughout the era of solid-organ transplantation, Although it is less common, the transmission of fungi9,10. In this case the results of postmortem coccidiodal serological tests for the donor were negative, the donor no residing in the traditional areas of endemicity of C. Immitis, none other recipients of the donor presented coccidiodomycosis manifestations over the time.
Primary pulmonary coccidiodomycosis is usually a self limited illnes, the presenting as acute respirtaory failure is distinctly uncommon, and has been most frecuently associated with underlying inmunosupresive conditions, particulary steroid therapy and massive exposure to C immitis, very rarely primary pneumonia is overwhelming and complicated by respiratory failure and the mortality of acute disseminated coccidioidomycosis is high, and the outcome may not be altered by antifungal therapy8.
The case that we are presenting add to the small list of reports documenting the ocasionally acute and agressive nature of the disseminated clinical form of coccidiodomycosis.

