











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
On April 7, 2021, the European Medicines Agency (EMA) Safety Committee stated a review of cases of thrombosis associated with thrombocytopenia and, in some cases, he morrhage in people who received the ChAdOx1 nCoV-19 vaccine (Vaxzevria, formerly COVID-19 AstraZeneca vaccine) and concluded that these events should be included as infre quent side effects of Vaxzevria.
On April 20, 2021, the EMA’s Pharmacovigilance Risk As sessment Committee (PRAC) concluded that a warning about “unusual blood clots with low blood platelets” should be added to the product information for the COVID-19 Janssen vaccine. The PRAC also concluded that these events should be included as infrequent side effects of the vaccine.
These cases of thrombosis with thrombocytopenia included venous thrombosis events at unusual sites, such as cerebral venous sinus thrombosis (VST) and splanchnic vein throm bosis (SVT), as well as arterial thrombosis. Most of the cases reported so far have occurred in women under 60 years of age, within two weeks after the first dose. There is limited information about the second dose.
Healthcare professionals should be alert to signs and symp toms of thrombosis in unusual sites such as cerebral venous sinus, splanchnic veins, multi-site arterial thrombosis, or usual venous thrombosis or pulmonary thromboembolism associated with thrombocytopenia, in order to seek timely diagnosis and treatment, according to the recommendations presented in this document.
Health care professionals should inform vaccine recipients that they should seek medical attention if they experience any of the following symptoms:
Neurologic: sudden onset of severe or persistent worse ning headaches, blurred vision, focal neurologic manifes tations, or seizures
Persistent abdominal pain, nausea, vomiting
Dyspnea, precordial pain, tachycardia, or arrhythmias
Edema, redness in an extremity, or pallor and coldness in a limb; pain or functional limitation.
Petechiae and ecchymosis away from the vaccination site
In terms of mechanism, it is believed that the vaccine may trigger an immune response leading to an atypical heparin-induced thrombocytopenia-like disorder mediated by anti bodies directed against platelet factor 4 (PF4)1. At this time, it is not possible to identify specific risk factors.
After using the Bradford-Hill criteria, the EMA found seve ral arguments to support that a causal relationship between vaccination with Vaxzevria and adverse events is at least a reasonable possibility2,3. There are enough alarm signals to consider those episodes, occurring mainly in women under 55 years of age and with a time of onset within two weeks after vaccination, could be associated with the biologic. Aty pical heparin-induced thrombocytopenia (aHIT) is the most plausible disorder given the similarities observed in the sero logic profile and clinical presentation of the affected patients. It is considered extremely likely that the syndrome, which resembles aHIT, is related to a severe autoantibody against PF4 with high binding affinity. It was hypothesized that the antibody itself is changing the structure of PF4, similar to what has been shown for aHIT. Greinacher et al 1 found high titers of anti-PF4 antibody in all patients with serological stu dies, supporting this hypothesis. The same authors sugges ted naming this disorder as vaccine-induced prothrombotic immune thrombocytopenia and, based on this, an algorithm was proposed by the German Society for Thrombosis and Hemostasis Research (GTH) (4.
Subsequently, the name of the entity has been changed to Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT) (5,6. In addition, the scientific advisory board at COVID-19 in Ontario7 and the British Society of Haematology published guidelines for thrombosis syndrome and thrombocytopenia after coronavirus vaccination, including a classification of ca ses8. However, there is no consensus regarding the case defi nition, since not all specific presentations of thromboembolic events have been defined. Therefore, the EMA report recom mended that the definition should not be limited to those cases of cerebral VST with thrombocytopenia and could be broadened to include all thrombotic events2.
The importance of immediate specialized medical treatment is emphasized. By recognizing the signs of blood clots and low blood platelets and treating them early, health profes sionals can help recovery and avoid complications in those affected. Thrombosis in combination with thrombocytopenia requires specialized clinical management. Healthcare profes sionals should consult applicable guidance and consult spe cialists (e.g., hematologists, coagulation specialists) to diag nose and treat this condition.
Given the current timing of the pandemic and the morbidity and mortality impact of SARS CoV2/COVID-19 infection, the positive effects of vaccination outweigh the risks. However, under the precautionary principle, we should keep close sur veillance of the evidence, and strengthen the processes of pharmacovigilance, identification, and timely management of cases, as well as community literacy programs and stan dardization of clinical practice.
Health professionals and vaccine recipients should be aware of the possibility of very rare cases of thrombosis associated with thrombocytopenia occurring within two weeks of vacci nation. However, COVID-19 is associated with a relevant risk of thrombotic events associated with infection and a high risk of hospitalization and death, so the overall benefits of these vaccines far outweigh the risk of adverse events from the vaccines.
For all of the above, the panel of experts of the Colombian Consensus for the diagnosis and management of persons with suspected vaccine-induced immune thrombotic throm bocytopenia generates recommendations within the fra mework of a person-centered care model, which guarantees clear and transparent information to persons regarding the risks and benefits of vaccination, as well as guidelines that allow them to suspect, detect and manage these thrombotic conditions promptly.
Methodology
We developed evidence-based and evidence-informed re commendations following the Manual for the Development of Clinical Practice Guidelines and the methodology proposed by NICE for generating guidelines in response to health and social care emergencies, agreed with clinical experts. From the EMA reports published up to April 7, 2021, about the occurrence of VITT, in April 2021 the work team performed a free search in Google Scholar in the first ten pages of results with free terms including “vaccine,” “AstraZeneca,” “Janssen,” “Johnson & Johnson”, “thromboembolic”, “events,” from which relevant documents were selected. Subsequently and in a complementary manner, we consulted the web pages of governmental agencies, national and international scientific societies, and guideline development sites, which allowed the narrative synthesis of information of clinical interest on cases of patients with VITT, which revealed the absence of sufficient information regarding pathophysiological mecha nisms, diagnostic standards, and specific management.
With the available information and the clinical expertise of the working group, the members of the Knowledge Mana gement and Transfer Network (RGTC for its Spanish initials) listed below, formulated, reviewed, and endorsed the recom mendations contained in this document:
Global Institute of Clinical Excellence
Colombian Association of Hematology and Oncology
Latin American Cooperative Group of Hemostasis and Thrombosis
Colombian Association of Neurology
Colombian Association of Internal Medicine
Colombian Association of Critical Medicine
Colombian Association of Gastroenterology
Colombian Association of Pneumology and Thoracic Surgery
National University of Colombia
Colombian Association of Nephrology and Arterial Hy pertension
Simon Bolivar University
Colombian Society of Family Medicine
Colombian Association of Emergency Medicine Specialists
Los Andes University
Colombian Society of Cardiology and Cardiovascular Sur gery Association
Colombian Association of Organ Transplantation
Colombian Association of Infectology
Sanitas University Foundation
Colombian Association of Scientific Societies
University Foundation of Health Sciences
Part of the recommendations we consulted are derived from evidence of similar conditions such as heparin-induced thrombocytopenia. Therefore, we would like to clarify that:
This document is considered a living document that will be updated as new evidence emerges, and recommenda tions may change over time. However, patient manage ment should be individualized to specific circumstances.
Under person-centered care guidelines, all necessary, clear, and truthful information regarding the risks and the benefits of vaccination should be provided.
A literacy plan should be included for the community and for emergency, specialized and primary care teams to identify and manage cases on time.
These recommendations should be included in the phar macovigilance guidelines.
Recommendations
The following are the recommendations endorsed by RGTC, including guidelines for diagnosis, approach to special con ditions such as venous sinus thrombosis and splanchnic thrombosis, and treatment recommendations.
Diagnosis
Even though we found insufficient data to support a com monly agreed diagnostic strategy or a standard case defini tion for VITT, characteristic findings in patients are:
Reduced platelet count.
Venous or arterial thrombotic events occurring within a typical risk window (i.e., 4-28 days post-vaccination)
Thrombotic complications including, but not limited to VST, and even thrombotic events at multiple sites.
High titers of anti-PF4 antibodies which may be reques ted, when available, after Hematology expert evaluation.
Exclusion of other etiologies of venous thrombosis and thrombocytopenia.
The need for and characterization of the most appropriate functional tests remains to be established.
When to suspect VITT?
VITT should be suspected in persons who previously received vaccination against SARS CoV2 between 4 and 28 days.
Flu-like symptoms such as: arthralgias, osteomyalgias, and mild to moderate headache in the first 2 to 3 days of vaccine administration are common side effects of all currently avai lable vaccines and are not a cause for concern.
The following manifestations should arouse suspicion, and lead to evaluation for thrombosis and thrombocytopenia8,9,10:
Neurologic symptoms: sudden onset of severe headache; or persistent, progressive, worsening headache, blurred
vision, focal neurologic manifestations, seizures
Persistent abdominal pain, nausea, vomiting
Dyspnea, precordial pain, tachycardia, or arrhythmias
Edema, redness in an extremity; or pallor and coldness in a limb; pain or functional limitation.
Petechiae and ecchymosis away from the vaccination site.
As a good practice tip, always rule out SARS-CoV2/ COVID-19 infection through SARS CoV2 rt-PCR testing.
VITT Case Definitions
The Expert Panel of the British Society of Haematology8 has proposed case definitions adapted as described below. It is essential to point out that there is no unanimity among the scientific societies of other countries in recommending these definitions.
Definite case
Usually occur between 5 and 28 days after vaccination (it should be noted that most cases report onset of symp toms in the first 16 days after vaccine administration).
Rapidly progressive thrombosis (with a high preponde rance of cerebral VST, but splanchnic thrombosis, pulmo nary embolism, and arterial ischemia may also occur).
Typical laboratory findings:
platelet count <150 x109/ L,
very raised D-dimer levels (> 4000ng/mL, above the level expected for venous thromboembolism),
many develop low fibrinogen levels.
Antibodies to platelet factor 4 have similarities to hepa rin-induced thrombocytopenia (HIT), but in the absence of patient exposure to heparin treatment. Antibodies are detected by ELISA assay (when available) but not usually by other HIT assay methods.
Emphasize that other common causes of thrombosis and thrombocytopenia such as: atypical hemolytic ure mic syndrome, thrombotic thrombocytopenic purpura, antiphospholipid syndromes, hematologic malignancies, heparin-induced thrombocytopenia, paroxysmal noctur nal hemoglobinuria have been ruled out.
Verify that the patient has not received previous heparin therapy.
Suspected cases can be classified as follows:
Possible case
Any patient presenting with acute thrombosis or new onset thrombocytopenia within 28 days of receiving the SARS CoV2 vaccine. Based on further evaluation, possible cases are reclassified as unlikely or probable.
Unlikely case
Thrombocytopenia without thrombosis with D dimer at or near normal and normal fibrinogen
Thrombosis with normal platelet count, with D-dimer <2000 ng/mL and normal fibrinogen
Intermediate or high probability of heparin-induced thrombocytopenia.
Likely case
The patient has not received heparins or has a low proba bility of HIT.
D-dimer > 4000 ng/mL (or D-dimer 2000-4000 ng/mL with strong clinical suspicion)
Diagnostic approach
The RGTC has agreed on the following recommendations for the diagnostic approach5,7-9,11-13:
If there is clinical suspicion or a possible case, we suggest requesting the following laboratory tests:
Hemogram and manual platelet count in a citrated tube, reticulocyte count, peripheral blood smear (in search of differential diagnoses).
D-dimer
Fibrinogen
Prothrombin time and activated partial thromboplas tin time.
According to the clinical presentation, consider RT-PCR test for SARS-CoV2 to diagnose COVID-19.
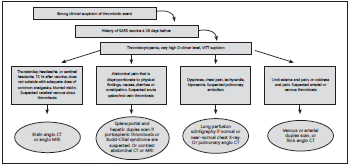
In case of clinical suspicion of thrombotic phenomena, consider, according to previously established guidelines, the request for confirmatory diagnostic imaging (Fig. 1), and the concept of the corresponding specialties (e.g., Internal Medicine, Hematology, Neurology, or Gastroen terology):
Cerebral VST: computed axial tomography (CT) with angiography in arterial and venous phase, or cerebral magnetic resonance angiography with venography.
Splanchnic venous thrombosis (SVT): ultrasound with Doppler (for the diagnosis of portal venous thrombo sis and Budd-Chiari syndrome), or CT angiography, or magnetic resonance venography (diagnosis of all types of SVT and differential diagnoses).
Pulmonary thromboembolism: pulmonary scintigra phy (when there is normal or near-normal chest X-ray), or CT angiography.
Deep venous or arterial thrombosis: venous or arte rial Doppler or CT angiography depending on the cli nical condition.
In patients with previous exposure to heparin, consider differential diagnosis with heparin-induced thrombo cytopenia (HIT). The 4T score is used 14. Prior exposure to heparin makes it more likely that it is the cause, but the treatment of VITT and HIT is similar.
In probable cases (acute thrombosis, thrombocytopenia, and high D-dimer elevation between 4 and 28 days after receiving the vaccine):
Request concept of Internal Medicine, or Hematology.
Request evaluation by Neurology, Gastroenterology, or General Surgery depending on the location of the thrombosis.
When available, consider ELISA test to detect anti bodies against platelet factor 4 or save serum sam ple for further processing. Those who test positive should have a confirmatory HIPA (heparin-induced platelet activation) or SRA (serotonin-release assay) test. Ideally, a modified test (no heparin, free PF4 FP4) should be available for atypical cases. This is impor tant because patients who do not have antibodies by ELISA can be treated with heparin.
Addressing specific conditions
Since some of the thrombotic manifestations of VITT can be diffi cult to diagnose, some diagnostic clues are summarized below.
Cerebral venous sinus thromboses (VST)
Cerebral VST is an uncommon form of cerebrovascular attack (CVA)15. Unlike arterial stroke, which is more prevalent in the elderly, VST generally affects young people. Eighty percent of cases occur under 50 years of age, and 75% in women16,17.
Risk factors for VST are associated with acquired and inhe rited events, including central nervous system events such as neoplasms and intracranial infections, procedures such as surgery and lumbar puncture, and systemic risk factors for thrombotic events, e.g., nephrotic, vasculitis, oral contracep tives, pregnancy and puerperium18. Oral contraceptive use is by far the most common risk factor, and is associated with an approximately 6-fold increased risk for VST19,20.
Cerebral venous sinus thrombosis, along with other paradoxi cal thromboembolic events, occurs in other immune thrombo cytopenic states such as immune thrombocytopenia and HIT. Although viral infections rarely cause VST, SARS CoV2/ COVID-19 infection is associated with stroke involving arterial and venous vessels, producing stroke directly with thrombosis in situ or indi rectly through systemic inflammation and endotheliopathy.
The diagnosis of VST is often delayed by about seven days from the onset of clinical manifestations. The most frequent symptoms are headache (89%), seizures (39%), paresis (37%), papilledema (28%), and mental status changes (22%), with specificities depending on the sinus involved. Large sinu ses are the most frequently affected, such as the superior longitudinal and lateral (transverse) sinus, The pain is usua lly bilateral, global, anterior or posterior of mild onset with progression to a severe picture, or of subacute course that increases with Valsalva maneuvers. The type of headache of vascular origin is called thunderclap headache, characteri zed by sudden pain of greater severity in the first minute, intensity greater than 7/10 on the analogous functional scale, of rapid recovery or may be manifested by mild dull pain. Another pain is sentinel headache, characterized by the se cond peak of pain 3 to 14 days after the initial one, moderate to severe, with symptoms and signs of focalization of other neurological áreas21. On physical examination, papilledema, involvement of the lateral rectus muscles, increased tone and reflexes, as well as changes in heart rate, blood pressure, and respiratory rate, up to profound compromise of conscious ness are characteristic.
The manifestations according to the main venous sinuses in volved are:
The superior sagittal sinus drains most of the cerebral cortex. The clinical manifestation is the characteristic hea dache of endocranial hypertension in 70% of cases. Pa tients usually present with focal neurological symptoms, seizures, and papillary edema. The lateral sinus drains blood from the sagittal sinus, cerebellum, brainstem, and posterior cerebral hemispheres. Isolated occlusion is rare; patients usually have thrombosis of multiple sinuses or cerebral veins. Manifestations are similar to those of su perior sagittal sinus. The cavernous sinuses lie on either side of the sella turcica. They drain blood from the or bits and from the anterior part of the base of the brain. Patients usually present with headache, chemosis, prop tosis, red-eye, and painful ophthalmoplegia. The presen tation may be more insidious, with only sixth-pair palsy, mild chemosis, and proptosis.
If VST is suspected, a computed tomography (CT) scan with angiography in arterial and venous phase or cerebral magnetic resonance angiography should be performed.
Splanchnic venous thrombosis (SVT)
The concept of SVT includes mesenteric venous thrombosis, portal vein thrombosis, splenic vein thrombosis, and Budd- Chiari syndrome. Thrombosis may co-occur in several of these beds22,23. The clinical manifestations of acute SVT are nonspe cific and sometimes present without causing acute symptoms. The most common symptom is abdominal pain in about half of the patients, followed by gastrointestinal tract bleeding and ascites. Pain disproportionate to the findings on physical examination is usually striking. Other symptoms include nau sea, vomiting, anorexia, diarrhea or constipation, and fever. In addition, each site of thrombosis may manifest differentially. The manifestations of sub-acute and chronic SVT may be di fferent, but they are of less interest for VITT diagnosis.
Acute mesenteric venous thrombosis is manifested by signi ficant abdominal pain and may be associated with diarrhea, nausea, vomiting, and lower gastrointestinal tract bleeding. When the proximal venous arches are involved, abdominal pain is more severe and spread to the dorsum, and ileus oc curs due to ischemia. Intestinal infarction occurs in one third of patients and should be suspected when there is hema tochezia, ascites, metabolic acidosis, acute renal injury, or respiratory failure. Acute portal vein thrombosis may be ma nifested by abdominal pain of sudden onset, with fever, nau sea, vomiting, and diarrhea. Acute splenic venous thrombo sis presents with abdominal pain, gastrointestinal bleeding, and nausea. Acute Budd-Chiari syndrome is manifested by abdominal pain, ascites, hepatomegaly, and hepatic necro-inflammation, leading to liver failure in severe cases.
Treatment
Since this is a newly described syndrome, whose disease mechanisms remain to be elucidated, all recommendations are based on extrapolations from previously known condi tions, such as HIT and non-heparin-dependent autoimmune thrombocytopenic thrombocytopenias, and analysis of clini cal features in reported cases.
In patients presenting with new-onset thrombocytopenia and documented thrombosis between 4 and 28 days post-vaccination, several international societies have generated documents that include treatment recommendations similar to that for severe HIT4,8-10. This treatment should be initia ted promptly in the presence of a high clinical suspicion of VITT, even in the absence of a report of antibodies to PF4. Recommended treatment includes intravenous human im munoglobulin (IVIG), and anticoagulation without heparin. Anticoagulation is selected according to the patient’s clinical status; direct oral anticoagulants (with a preference for factor Xa inhibitors), parenteral direct thrombin inhibitors (argatro ban or bivalirudin), and fondaparinux have been mentioned among the options. Greater caution is required for the use of anticoagulation when platelets are less than 50 x 109/L or when there is severe bleeding. However, VITT is associated with fibrinogen consumption and bleeding, which should not absolutely contraindicate anticoagulation, particularly if the platelet count is greater than 20 x 109/L and rising after initia tion of IVIG9,10. While so far there is no evidence that heparin products worsen immune thrombotic thrombocytopenia, the syndrome’s similarities to HIT suggest avoiding unfractiona ted or low-molecular-weight heparin.
Also based on similarities with HIT, it is recommended to avoid platelet transfusions. However, risk/benefit assessment in individual patients with severe bleeding and need for sur gical intervention may favor platelet transfusion, following initiation of IVIG, non-heparin anticoagulation and fibrino gen replacement (if deficient).
Based on the publications reviewed4,7-13 and experience with other entities with similar presentations, the RGTC reached consensus on a management algorithm (Fig. 2) and the fo llowing treatment recommendations:
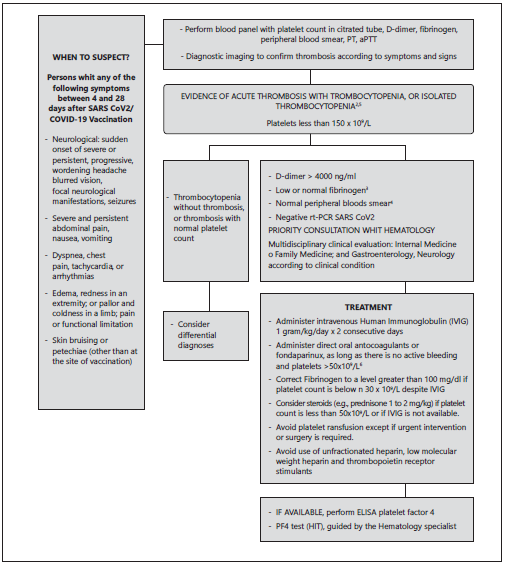
Notes: 1. Also refered to as vaccine-induced immune thrombotic thrombocytopenia (VITT). 2. A patient presenting whith thrombosis ans a normal platelet count after vaccination requires ongoing evaluation for the development of thrombocytopenia/VITT. 3. Low fibrinogen and extremely high D-dimer levels suggest the diagnosis of diseminated intravascular coagulation, which is included in the VITT syndrome. 4. Microangiopathy with red cell fragmentation and hemolysis has not been a feature of thereported cases. 5. Patients who develop isolated thrombocytopenia may be in the early stage of VITT, but in the continued absence of thrombosis should be considered Immune trombocytopenic purpura associated whith vaccination, which is not included in the VITT syndrome. 6. In the presence of documented thrombosis, the use of anticoagulants is indicated. Caution should be used whit platelet counts below 50k/uL or in patients with active bleeding.
Modified from: Scully M, Singh D, Lown R, et.al. Pathologic Antibodies to Platelet Factor 4 after ChAdOx1 nCoV-19 Vaccination. Science Briefs of the Ontario COVID-19 Science Advisory Table. 2021 Mar;1(17) online ahead of print, 2021 Apr 16. N Eng J Med 2021;10.1056/NEIMoa2105385. Pai M, Grill A, Ivers et.al. Vaccine induced prothombotic immune thrombocytopenia VPIT followin AstraZeneca https://doi.org/10.47326/ocsat.2021.02.17.1.0. American Society of Hematology. Vaccine-induced Immune Trhombotic Thrombocytopenia: Frecuently Asked Questions. (Version 1.1; last updated April 19, 2021). https://www.hematology.org/covid-19/vaccine-induced-immune-thrombotic-thrombocytopenia. British Society of Haematology. Guidance produced by the Expert Haematology Panel (EPH) focussed on Vaccine induced Thrombosis and Thrombocytopenia (VITT). Version 1.3.7 April 2021 https://b-s-h.org.uk/media/19530/guidance-version-13-on-mngmt-of-thrombosis-whith-thrombocytopenia-occurring after-c-19-vaccine_20210407.pdf . file:///C:/Users/nyomayusa/Downloads/ISTH%20VITT%20Guidance%202.pdf
Figure 2 Algorithm for the diagnosis and management of Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT)1
In likely or definite cases of VITT, we recommend to ini tiate in-patient treatment as a priority while awaiting confirmation of the diagnosis.
Administer IVIG at a dose of 1 gram/kg/day for two con secutive days.
In patients with thrombosis in connection with VITT, we suggest to initiate anticoagulant therapy without delay.
-Consider platelet count, age, comorbidities, and blee ding risk to individualize the appropriate anticoagu lant type and dose.
-In particular cases, consider using adjusted doses of anticoagulants.
-Apply greater caution for the use of anticoagulation when platelets are less than 50 x 109/L or when there is severe bleeding. Even though, decreased fibrino gen and bleeding do not absolutely contraindicate anticoagulation, mainly if the platelet count is greater than 20 x 109/L and rising after initiation of IVIG.
-In all cases, the platelet count and overall clinical course should be assessed daily or more frequently to define appropriate management changes.
Even with thrombocytopenia, these patients require an ticoagulation, ideally with the accompaniment of a he matologist in the multidisciplinary management team. If not available, the patient should be urgently referred to a third or fourth-level institution.
We recommend anticoagulants (other than heparin) such as those used to treat heparin-induced thrombocytopenia. These include direct anticoagulants and fondaparinux.
We recommend following the general recommendations to start therapy with direct oral anticoagulants, without using heparins in the first days, considerations related to the risk of bleeding due to the association with thrombocytopenia:
-Prefer low anticoagulant doses until the platelet cou nt is in a safe range (greater than 50 x 109/ L), e.g., rivaroxaban 10 mg PO once a day, or apixaban 2.5 mg PO every 12 hours.
-Take into account the availability of anticoagulation reversal agents.
If fondaparinux is preferred, consider weight adjusted dosing.
We recommend NOT to use unfractionated heparin, low molecular weight heparin, or vitamin K antago nists. Avoid use of heparin in catheters.
We suggest NOT to use rutinary platelet transfusion. It should be reserved for life-threatening bleeding or before invasive procedures. In such a case, this should preferably be done after initiating IVIG, anticoagulation without he parin, and fibrinogen replacement (when deficient).
Avoid use of thrombopoietin receptor stimulants (el trombopag/ romiplostim).
Consider steroids (e.g., prednisone 1 to 2 mg/kg) if the pla telet count is less than 50 x 109/L or if IVIG is not available.
Correct fibrinogen to levels greater than 100 mg/dl if pla telet count remains less than 30 x 109 / L despite IVIG and steroid therapy.
The use of plasma exchange (when available) could be considered, if agreed in a medical board.

