










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista de Salud Pública
Print version ISSN 0124-0064
Rev. salud pública vol.11 no.6 Bogotá Nov./Dec. 2009
Maria Jacirema Ferreira Gonçalves1, Antonio Carlos Ponce de Leon2 and Maria Lúcia Fernandes Penna2
1 Escola de Enfermagem de Manaus. Universidade Federal do Amazonas. Brasil. jaciremagoncalves@ufam.edu.br
2 Instituto de Medicina Social/ Universidade do Estado do Rio de Janeiro
Received 24th April 2009/Sent for Modification 10th October 2009/Accepted 4th November 2009
ABSTRACT
Objective Evaluating the association between TB and AIDS and estimating the determinant effects and factors for TB incidence rates in Brazilian metropolitan regions from 2001 to 2003.
Methods A Poisson longitudinal multilevel model was fitted to the annual TB case number by municipality and year, including the population as an offset variable, and AIDS incidence by metropolitan region, percentage low-income households, demographic density and TB cure rate by municipality and Brazilian geographic area as independent variables.
Results All variables were found to be significantly associated with tuberculosis (except for cure rate %): low income, demographic density, AIDS and Brazilian area. Interaction between AIDS and low income was significant and modified the effect of AIDS on TB incidence. Empty model and full model variance reduction percentages from first to third levels were 40.2 %, 42.2 % and 77.3 %, respectively.
Conclusions AIDS has become an impressive morbidity factor due to tuberculosis; this has not been found in previous studies in Brazil. The interaction between income and AIDS and the metropolitan regions’ important contribution towards tuberculosis distribution were heterogeneously manifest amongst large Brazilian areas.
Key Words: Tuberculosis, socioeconomic factor, statistical model, AIDS (source: MeSH, NLM).
RESUMEN
Objetivo Evaluar la asociación entre las tasas de incidencia de tuberculosis y HIV y estimar los efectos y factores determinantes de la incidencia de tuberculosis en las regiones metropolitanas de Brasil, del 2001 al 2003.
Método Los casos de tuberculosis por municipio y año fueron adaptados al modelo Poisson multinivel, incluyendo la población como variable offset. Como variables independientes se utilizaron la tasa de incidencia de HIV por región metropolitana, las grandes regiones geográficas del Brasil, la proporción de casas con ingreso bajo, densidad geográfica y tasa de enfermos curados de tuberculosis por municipio.
Resultados Con excepción de la tasa de enfermos curados, todas las variables presentaron asociación significativa con la tuberculosis. La relación entre HIV e ingreso bajo es significativa y modifica el resultado de la incidencia de la tuberculosis. El porcentaje de disminución de la varianza entre el modelo vacío y el modelo lleno, del primer al tercer nivel fue respectivamente, 40,2 %, 42,2 % y 77,3 %.
Conclusiones HIV es un factor impactante de morbilidad por tuberculosis, no encontrado antes en otros estudios. La influencia entre renta y HIV, es una importante contribución de las regiones metropolitanas en la distribución de la tuberculosis, distribuida heterogéneamente en las grandes regiones del país.
Palabras Clave: Tuberculosis, factores socioeconómicos, modelos estadísticos, SIDA (fuente: DeCS, BIREME)
RESUMO
Objetivo Avaliar a associação entre as taxas de incidência de Tuberculose (TB) e AIDS e estimar os efeitos e fatores determinantes da incidência de tuberculose nas regiões metropolitanas do Brasil, de 2001 a 2003.
Métodos Os casos de tuberculose por município e ano foram ajustados em um modelo Poisson multinível, incluindo a população como variável offset. Como variáveis independentes utilizaram-se a taxa de incidência de AIDS por região metropolitana, as grandes regiões geográficas do Brasil, a proporção de domicílios com renda baixa, densidade demográfica e taxa de cura de tuberculose por município.
Resultados Com exceção de cura, todas as variáveis apresentaram associação significante com a tuberculose. O termo de interação entre AIDS e renda baixa é significante e modifica o efeito da incidência de tuberculose. O percentual de redução da variância entre o modelo vazio e o modelo cheio, do primeiro ao terceiro nível, foram respectivamente, 40,2 %, 42,2 % e 77,3 %.
Conclusões AIDS é um fator impactante da morbidade por tuberculose, anteriormente não encontrado em outros estudos. A interação entre renda e AIDS, e a importante contribuição das regiões metropolitanas na distribuição da tuberculose, distribui-se heterogeneamente nas grandes regiões do país.
Palavras Chave: Tuberculose, fatores socioeconômicos, modelos estadísticos, SIDA (fonte: DeCS, BIREME)
The worldwide tuberculosis (TB) case load is very high; Brazil is amongst the 22 countries concentrating 80 % of TB cases around the world. Estimates point to 50 million people currently being infected in Brazil,an annual average of around 80,000 cases being reported every year. Almost 60 % of these are sputum smear-positive, having a 45.2/100,000 inhabitants incidence rate in 2003 (1).
According to the Brazilian Institute of Geography and Statistics’ Demographic Census, Brazil has 169,799,170 inhabitants living on almost 8,500,000 km2. It consists of a federation of 26 states and a Federal District and has 5,561 municipalities. Brazil is also geographically divided into five major areas: the Northern, North-eastern, South-eastern, Southern and Central-Western regions.
Brazil is a middle-income country, having high social heterogeneity. There are highly industrialised and urbanised regions but also remote areas where subsistence agriculture and barter still exist. Every TB study must include socioeconomic factors. However, due to the country’s large variation, traditional socioeconomic indicators (such as income and educational level) acquire different meanings in different contexts, which may lead to bias.
It was decided to restrict this study to the 28 Brazilian metropolitan regions to avoid such possible bias; these are formed by 387 municipalities, housing 40 % of the country’s population. The metropolitan regions are responsible for 50 % of TB cases in Brazil, of which only Rio de Janeiro and São Paulo (the two largest Brazilian cities) together account for 28% of the total TB case load (2,3).
The emergence of acquired immune-deficiency syndrome (AIDS) epidemics has magnified the TB problem (4, 5), since AIDS patients also infected by the TB bacillus frequently developed the disease.
The TB incidence gradient decreased from North to South in the early 1980s (6) as the human immunodeficiency virus (HIV) became introduced into the country in the South and South-eastern regions in the higher socioeconomic strata (7). 307,240 AIDS cases were notified in Brazil from the beginning of the AIDS epidemic in 1980 to 2003, a higher concentration being reported in the Southeastern and South regions, these being the most developed ones (7). The metropolitan regions housed 70 % of AIDS cases (216,642 cases) during this period. TB/HIV co-infection is an increasingly serious problem. Reports pointed to coinfection rates in 2006 ranging from 25.9 % in Porto Alegre to 8.1 % in Rio de Janeiro and 2.5 % in São Luís (8).
Few studies in Brazil have approached the impact which AIDS has had on TB epidemiological behaviour or have queried the current AIDS-TB impact (9). Some studies have analysed the problem in just one municipality (10-12).
The impact of the AIDS epidemic on TB epidemiological behaviour in Brazil has never before been demonstrated by empirical data. The TB problem linked to the presence of AIDS in Brazil must still be assessed by identifying associations and contributing towards a better understanding of TB’s epidemiological behaviour in the country.
This study was aimed at evaluating the association between TB and AIDS incidence rates in Brazilian metropolitan regions and how the socioeconomic situation has affected such association, based on 2001 to 2003 TB data.
A multilevel model was used in this ecological, longitudinal study; it was based on Ministry of Health (MoH) Communicable Disease Information System TB notification data in Brazil from 2001 to 2003. AIDS rates in 2002 were collected on-line from MoH’s Unified Health System Information and Data Department. Social and demographic data were gathered from the 2000 Demographic Census (3).
Of the 229,683 cases of TB registered in Brazilian metropolitan regions, 70,759 were recorded in 2001, 80,316 in 2002 and 78,608 in 2003. To avoid bias caused by delay in notifications at federal level, these years were taken because the surveillance system became more trustworthy from 2001 onwards, and 2003 was the last year included. Multilevel multivariate regression was used. To build the model, the lowest (first level) analysis unit was year-municipality, municipalities at the second level and metropolitan regions at the third level. The dependent variable was the number of TB cases notified during every year by each municipality. The independent variables were time (2001, 2002 and 2003), municipal income strata (income1, income2, income3), municipal demographic density area (inhabitants per hectare - density), family head’s years of schooling (education), percentage of households having a piped water supply (water) in the municipalities, municipal percentage of TB patients who did not comply with the treatment amongst new cases where information on outcome was available (non-compliance), municipal cure percentage amongst new TB cases with information on treatment outcome (cure), defined as clinical discharge by the doctor after completing treatment, with or without confirmation by smear negative microscopy, geographic regions (North, Northeastern, South-eastern, South and Central-Western); and AIDS incidence rate in year 2002 by metropolitan region (AIDS).
Municipal socioeconomic strata were based on the percentage of low-income households (having less than two minimum wages monthly). The first stratum comprised 25 % of the richest municipalities (income1), meaning municipalities having less than 18.5 % low-income households, the second stratum was formed by 50 % of municipalities having an intermediate percentage of low-income households (18.5 % 25.5 %) (income2) and the third stratum included 25 % of the poorest municipalities, having more than 25.5 % low-income dwellings (income3).
New TB cases were modelled by Poisson longitudinal multilevel regression, with over-dispersion (extra-Poisson), using the logarithm of the yearly population as an offset variable. MLwiN 2.02 software was used for analysing the data (13). The model estimated independent variables’ fixed effects and included a random effect at second and third levels. It also included a random slope at municipal level. The estimates used the iterative generalised least squares (IGLS), and the linearization used the predictive quasi-likelihood (PQL), that maximizes the Likelihood Function (14). That was needed due to the non linearity of the Poisson model.
In order to evaluate the adequacy of the multilevel model to the data, an empty model (the intercept-only model) was fitted to screen distinct intercept variances for each level. It was also used as a baseline to compare the random effect variance reduction to the full model.
After adjusting the model, the diagnostic for validity of assumptions and estimates included the study of predictions and residuals, assessment of variances reductions of the random effects comparing empty and full models, interaction graph and statistical significance test of standard errors of the estimates using Wald test with a significance level of 0.05.
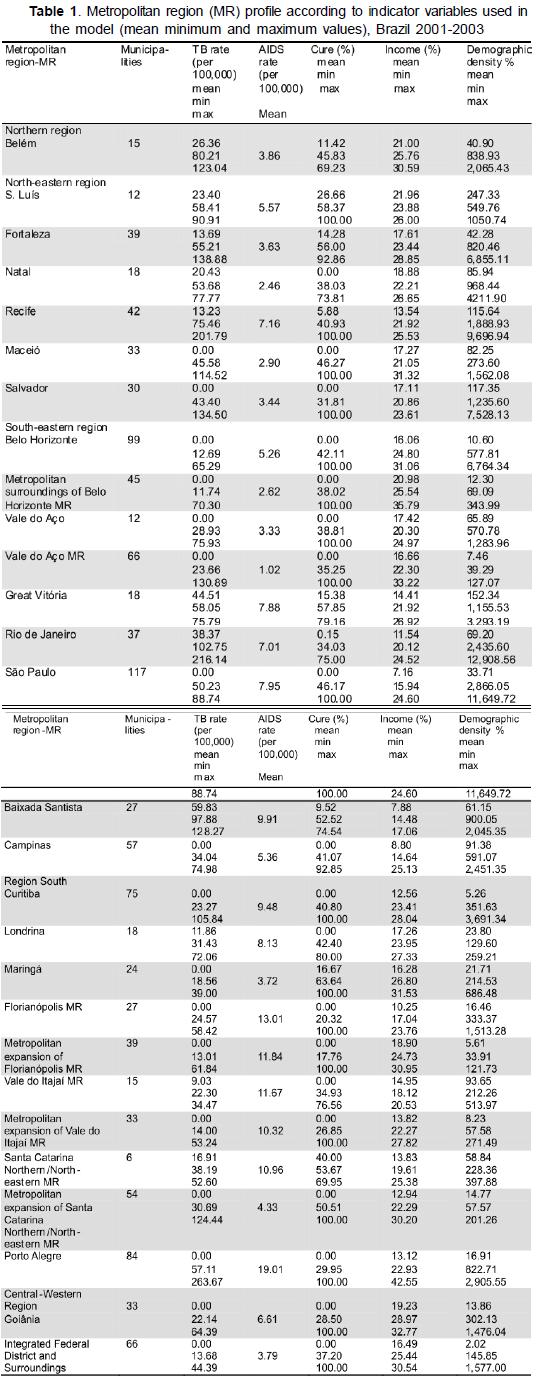
Table 1 shows the data from each metropolitan region. The empty model (with fixed intercept in years) estimated 0.11 random effect variance at first level, 0.87 at municipal level and 0.32 at metropolitan region level. All estimates were significant. No temporal trend was identified in yearly estimates.
The model’s results are shown in Table 2. An important variance reduction could be observed when comparing second and third levels’ random effects; the first level presented 0.06, the second 0.50 and the third 0.07, meaning that the model could explain part of the initial variance. This meant 40.2 %, 42.2 % and 77.3 % relative reduction, respectively.
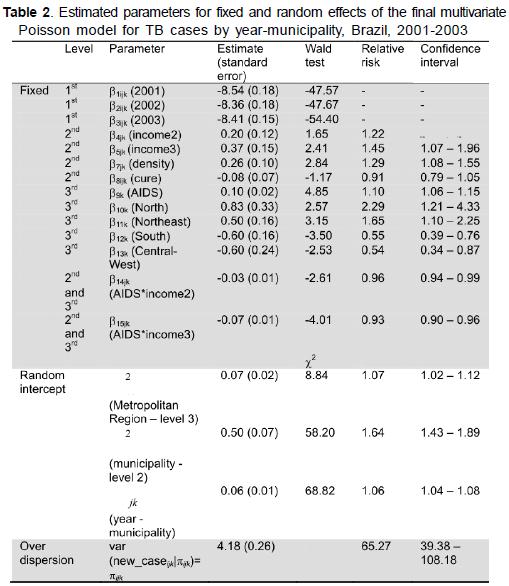
Residuals followed a normal distribution and did not correlate with predictors, meaning that the model fitted the data well. Non-significant term (cure) was kept in the model (due to its ability to reduce level variance) and its participation in the TB determination model as theoretically and previously defined.
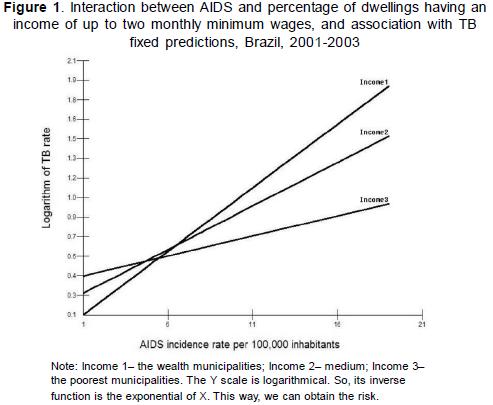
There is a cross variable level in this multilevel model (income and AIDS interaction). Figure 1 shows how income categories and AIDS rate were interposed in metropolitan regions. The model’s fixed predictions were plotted against the AIDS incidence rate, showing that the AIDS incidence rate’s influence on predicted TB cases was not uniform across income categories, pointing to the need for the interaction term, since there was a modification effect.
The data must be examined cautiously, considering the limitations of only having one ecological analysis using secondary data, which included hidden confounders and other interactions which were not measured or known. It was therefore carried out in line with a proper understanding of an ecological study.
There was no evidence of the impact of AIDS on TB transmission dynamics during the late 1990s. The present model produced empirical evidence of the influence of the AIDS epidemic on the TB incidence rate in Brazil which has not been published previously.
Variables included in the model complied with a theoretical model of TB social determination, as stated by several authors: the socioeconomic and demographic aspects and, in later years, AIDS, which has represented an important part of TB incidence and maintenance (15-17). Brazil does not have reliable data on HIV infection and the only reliable data available concerning HIV circulation is the AIDS reported incidence rate, which is a proxy variable of previous HIV transmission and past prevalence of infection. However, the AIDS development rate provides a better measurement of the possible influence of an HIV epidemic on TB transmission dynamics in the present context.
Multilevel analysis is not often used in epidemiological studies. However, studies using this approach have made important contributions to multilevel analysis (18-20). The main difference regarding multivariable regression techniques is the assumption that the smaller observation units’ (municipality by year in this paper) different levels of actual aggregation are relevant to the statistical modelling of data. In other words, incidence rate data variance by municipality by year can be divided into three: variance between each municipality’s yearly data, variance between different municipalities’ data in each metropolitan region and variance between metropolitan regions. These three components of total variance can be incorporated into the model (each being an analysis level), thereby avoiding the bias which would occur if the lack of independence of the data in each level were ignored (21).
As in any regression analysis, including independent variables in a model is intended to reduce random variance. A fraction of inside level variance in multilevel regression or a fraction of total variance in other regression models is explained by the independent variables. The present result showed that the model was capable of explaining 40.4 %, 42.2 % and 77.3 % of first, second and third level variance, respectively, meaning that the biggest variance reduction was that between metropolitan regions.
The multivariate Poisson model with random intercept choice was used due to the large amount of data taken on the few measurement occasions. It is worth pointing out that using different observation years in this paper must be treated as repeat measurement data, meaning that the same response variable was being measured at different times in a longitudinal study. The repeated measurement was included to provide more statistical information, and not to study the TB epidemiological pattern because it does not produce sensitive changes over a short period of time. As expected, no temporal trend was identified in the yearly estimates.
In the absence of income and AIDS incidence rate for forward entry model building, the percentage of low-income households showed a negative, significant association with TB incidence. However, when AIDS incidence rate was included it had negative association and made income positive, which is theoretically incoherent. Including an interaction term (income x AIDS), having a negative regression coefficient, made the regression coefficients of both income and AIDS positive, agreeing with the theoretical framework presented in the introduction.
Since using income as a continuous variable did not allow exploring this interaction, it was substituted by its categorisation into quartiles. Adjusting AIDS interaction and income allowed changes in effect and variance reduction to be evaluated. It can be noticed that the association between AIDS and TB was different in each income strata; such interaction showed a different aspect of the impact of AIDS on TB epidemiology to that described in Africa, for instance (17,22).
An important aspect of this interaction was that as AIDS had a greater influence on the areas without other TB risk factors, such as poverty (i.e. areas having a lower TB burden), the TB burden would tend to be asymptotically uniform throughout municipalities in the same metropolitan area. This meant that this interaction would disappear as TB transmission became homogeneous in a particular area.
TB cure percentage was not statistically significant in the model, probably because of the small variation in the low percentage of cure achieved by the municipalities. Non-cured cases provided disease dissemination and even spread resistant bacilli since there had been previous contact with medicines.
There was significant demographic density per area in each municipality, but it had a very small effect. TB was indeed associated with crowding which occurs more frequently in Brazil in metropolitan areas (23).
The importance of geographic regions in the model must be highlighted, since these areas presented a gradient having wide TB incidence rate variance. 2002 incidence rates for pulmonary TB in the Southern and Central- Western regions were 32.4 and 29.5 cases per 100,000 inhabitants, respectively. The Northern region had 47.6/100,000, the North-eastern one 45.1/ 100,000 and the South-eastern region 51.0/100,000. The presence of geographical regions in the model thus expressed TB epidemiological patterns in Brazil, having significant positive effects for the Northern and North-eastern regions and negative ones for the Southern and Central-Western ones in relation to the Southeast, meaning that the TB incidence rate in these regions was very similar to the Southeast (kept as base category in this analysis).
These findings revealed that the National Tuberculosis Control Program must be reinforced in Brazil, mainly by working more closely with the AIDS control program. Our results pointed to a future increase in TB incidence rates in municipalities having low TB incidence and high AIDS incidence. TB control must thus be reinforced not only in municipalities having high TB rates where the problem and its severity are already well-established but attention must also be paid to those areas where TB incidence rates may increase.
Brazil is a typical medium-income country where large metropolitan areas are still growing. Socioeconomic condition still remains as being an important determinant of TB incidence, independent of AIDS epidemics, although AIDS is clearly producing an impact on TB epidemiological dynamics in the country. Furthermore, new, especially designed studies are needed to deepen knowledge about TB patterns in Brazil as well as the influence of AIDS on TB to assure ongoing TB control in the future.
Acknowledgements. MJF Gonçalves was financed by Fundação de Amparo à Pesquisa do Estado do Amazonas (Fapeam–Process 008/2004).
1. Gonçalves MJF, Penna ML. Tuberculosis morbidity and effectiveness of the control program in Brazilian municipalities, 2001-2003. Rev Saude Publica. 2007; 41 Suppl 1:95-103. [ Links ]
2. Brasil. Ministério da Saúde. Fundação SEADE [Internet]. Anuário Estatístico do Brasil. Brasilia (DF): Ministério da Saúde; 2002; Available from: http://portal.saude.gov.br/saude/aplicações/anuario2002/index.cfm. Cited 2005 11/24. [ Links ]
3. IBGE. Instituto Brasileiro de Geografia e Estatística. Censo Demográfico 2000. Agregado por setores censitários dos resultados do universo. 2 ed.: Documentação do arquivo, Rio de Janeiro; 2003. [ Links ]
4. Ait-Khaled N, Enarson DA. Tuberculosis: a manual for medical students. Geneva/ Paris: World Health Organization / International Union Against Tuberculosis and Lung Disease; 2003. [ Links ]
5. Espinal MA. The global situation of MDR-TB. Tuberculosis. 2003; 83(1-3):44-51. [ Links ]
6. Penna MLF. Estratégias de controle da tuberculose: da descoberta do bacilo aos nossos dias. Cadernos do IMS. 1988; 2(2):117-46. [ Links ]
7. Fonseca MG, Szwarcwald CL, Bastos FI. A sociodemographic analysis of the AIDS epidemic in Brazil, 1989-1997. Rev Saude Publica. 2002; 36(6):678-85. [ Links ]
8. PHW. Public Health Watch. TB policy in Brazil: a civil society perspective. Program PH, editor. New York: Open Society Institute; 2006. [ Links ]
9. Laguardia J, Merchan-Hamann E. Risk factors for tuberculous disease in AIDS cases reported in Brazil, from 1980 to 2000. Rev Esp Salud Publica. 2003; 77(5):553-65. [ Links ]
10. Toledo ACC, Jr., Greco DB, Antunes CM. Risk factors for tuberculosis among human immunodeficiency virus-infected persons. A case-control study in Belo Horizonte, Minas Gerais, Brazil (1985-1996). Mem Inst Oswaldo Cruz. 2000; 95(4):437-43. [ Links ]
11. Antunes JL, Waldman EA. Tuberculosis in the twentieth century: time-series mortality in Sao Paulo, Brazil, 1900-97. Cad Saude Publica. 1999; 15(3):463-76. [ Links ]
12. Oliveira HB, Marin-Leon L, Cardoso JC. Differences in mortality profile of tuberculosis patients related to tuberculosis-AIDS co-morbidity. Rev Saúde Pública. 2004; 38 (4):503-10. [ Links ]
13. Rasbash J, Browne W, Healy M, Cameron B, Charlton C. MLwiN. Multilevel Models Project Institute of Education. Version 2.02. Centre for Multilevel Modelling. University of Bristol; 2005. [ Links ]
14. Goldstein H. Multilevel statistical models. 2. ed. London: Institute of Education, Multilevel Models Project; 1999. [ Links ]
15. Munch Z, Van Lill SW, Booysen CN, Zietsman HL, Enarson DA, Beyers N. Tuberculosis transmission patterns in a high-incidence area: a spatial analysis. Int J Tuberc Lung Dis. 2003; 7(3):271-7. [ Links ]
16. Pio A, Luelmo F, Kumaresan J, Spinaci S. National tuberculosis programme review: experience over the period 1990-95. Bull World Health Organ. 1997; 75(6):569-81. [ Links ]
17. Sonnenberg P, Glynn JR, Fielding K, Murray J, Godfrey-Faussett P, Shearer S. How soon after infection with HIV does the risk of tuberculosis start to increase? A retrospective cohort study in South African gold miners. J Infect Dis. 2005; 191(2):150-8. [ Links ]
18. Blakely TA, Woodward AJ. Ecological effects in multi-level studies. J Epidemiol Community Health. 2000; 54(5):367-74. [ Links ]
19. Werneck GL, Costa CH, Walker AM, David JR, Wand M, Maguire JH. Multilevel modelling of the incidence of visceral leishmaniasis in Teresina, Brazil. Epidemiol Infect. 2007; 135(2):195-201. [ Links ]
20. Diez-Roux AV. Multilevel analysis in public health research. Annual Revue Public Health. 2000; 21:171-92. [ Links ]
21. Kleimbaum DG, Kuppper LL, Muller KE, Nizam A. Applied regression analysis and other multivariable methods. 3 ed. Pacific Grove: Duxbury; 1998. [ Links ]
22. Dye C. Global epidemiology of tuberculosis. Lancet. 2006; 367(9514):938-40. [ Links ]
23. Vendramini SHF, Gazetta CL, Chiaravalotti Netto F, Cury MR, Meirelles EB, Kuyumjian FG, et al. Tuberculosis in a medium-sized city in the Southeast of Brazil: morbidity and mortality rates (1985 - 2003). J Bras Pneumol. 2005; 31(3):237-43. [ Links ]

