










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista de Salud Pública
Print version ISSN 0124-0064
Rev. salud pública vol.12 no.3 Bogotá May/June 2010
Marta Carvalho-Loures1, Celmo Celeno-Porto2, Maria Alves-Barbosa3 and Lindomar Guedes Freire-Filha4
1 School of Enfermagem, Pontifícia Universidade Católica de Goiás, Brazil.louresmarta@hotmail.com.br
2 School of Medicine, of the Federal University of Goiás, Brazil.
3 School of Enfermagem, of the Federantal University of Goiás, Brazil.
4 Institute of Socio-environmental Studies of the Federal University of Goiás, Brazil
Received 2th February 2010/Sent for Modification 3th July 2010/Accepted 11th July 2010
ABSTRACT
Objectives Assessing the quality of life (QOL) of elderly women attending the University of the Third Age (UNATI) at the Federal University of Goiás in Brazil.
Methods This was a descriptive, observational study of 38 elderly women aged 60 or older. A socio-demographic information form and the WHOQOL-BREF and WHOQOLOLD questionnaires were applied for QOL assessment.
Results Most women were aged 60-69 (58.8 %). The WHOQOL-BREF QOL scores in the physical, psychological, social relationships and environmental domains bore no statistical relevance; however, the general QOL before (67.86±2.91) and after (60.71±8.71) attending UNATI had p=0.049 significance. As for the WHOQOL-OLD, only the sensorial functioning domain (before: 61.84±20.74; after: 71.38±17.66; p=0.014) and the death and dying domain were significant (before: 56.36±25.48; after: 67.27±25.35; p=0.001).
Conclusions The elderly women demonstrated typical socio-demographic characteristics and their concerns to stay healthy within possible income, socialisation and health delivery service patterns were considered good. The WHOQOL-BREF revealed that the general domain played a major role compared to other domains. The sensorial functioning and the death and dying domains on the WHOQOL-OLD characterised this particular population's anxieties, wishes and gender needs.
Key Words: Quality of life, women, aged (source: MeSH, NLM).
RESUMEN
Objetivos El objetivo de este estudio fue avaluar mujeres ancianas que frecuentan la Universidad Abierta a la Tercera Edad (UNATI), en la Universidad Estadual de Goiás/ Brasil, con relación a la calidad de vida (CV).
Métodos Estudio observacional de tipo descriptivo con 38 mujeres ancianas, con edad igual o superior a 60 aà±os. Fue aplicado un cuestionario socio-demográfico y evaluación de la CV instrumentada por Whoqol-Bref y Whoqol-Old
Resultados La edad de mayor frecuencia fue de 60 a 69 aà±os (58,8 %). Los puntajes de CV de Whoqo-Bref de los dominios Físico, Psicológico, Relación Social y Medio Ambiente no tuvieron relevancia estadística. Sin embargo, la CV antes (67,86 ± 2,91) y después (60,71 ± 8,71) de la participación en la UNATI presentó diferencias significativas (p=0,049). En el Whogo-Bref, sólo los dominios Funcionamiento Sensorial (antes: 61,84 ± 20,74; después: 71,38 ± 17,66; p 0,014) y Muerte y Muriendo (antes: 56,36 ± 25,48; después: 67,27 ± 25,35; p 0,001), fueron significantes.
Conclusiones Las ancianas presentan características socio-demográficas propias, y se considera bueno los cuidados para mantener la salud dentro de los patrones posibles de rendimiento, socialización y oferta de los servicios de salud. Whogol-Bref reveló que el dominio General tuvo papel preponderante con respecto a los demás dominios. En el Whogol-Old, los dominios Funcionamiento Sensorial y, Muerte y Muriendo, caracterizan a la población en sus ansiedades, sus deseos y en las necesidades del género.
Palabra Clave: Calidad de vida, mujeres, edad (fuente: DeCS, BIREME).
By integrating one of the sectors of society which seeks aging with quality, universities are creating activities fostering the socialisation of those individuals pertaining to this age-band. The programme called the University of the Third Age in Goiás is an example of this.
The first University of the Third Age, which aimed at teaching and researching, was created in 1973 in Toulouse, France, according to Peixoto (1). The Brazilian Social Service of Commerce (SESC) promoted programmes aimed at the elderly's wellbeing in 1964 on establishing a so-called pensioners group, thereby favouring a decrease in feelings of isolation, loneliness and uselessness.
The first Universities of the Third Age were established in Brazil to regain the experiential and cultural values accruing with age during an individual's life, thus showing that aging can be accompanied by quality of life (QOL) patterns. Two universities in Goià¢nia have currently turned their efforts towards such patterns: the Catholic University in 1992 and the State University of Goiás in 2000. Both institutions have developed extension programmes offering third age students an improvement in their QOL.
The World Health Organisation (WHO) (2) considers that the three following aspects which were identified by a group of experts from different cultures are important when discussing QOL: subjectivity, multidimensionality and the presence of positive (e.g. mobility) and negative dimensions (e.g. pain and loneliness). These aspects must be measurable regarding QOL at any given place on the planet. Based on such assumptions, QOL can be defined as being, "an individual's perception of her/his position in life within the context of the culture and value systems in which they live and in relation to their goals, expectations, patterns and worries." (3)
The WHO developed a multicenter study during the 1990s to asses QOL from a transcultural perspective. This study gave rise to the World Health Organisation Quality of Life-100 (WHOQOL-100), the final version of which consisted of 100 questions and was developed and tested with the collaboration of 15 centres (4). Brazil was one of the collaborating research centres, developing the Portuguese version of the instrument. It had good psychometric performance, having satisfactory characteristics regarding "[...] internal consistency, discriminating validity, criterion validity, concurrent validity and testretest reliability." (5)
The WHOQOL-BREF, an abridged version of WHOQOL-100, is regarded as being more suitable for use in assistance practice and research in which assessment must be repeated several times or when more than one instrument is used (6). Derived from the former instrument, it contains 26 questions which showed better psychometric performance. It presents two questions about QOL in general and 24 questions (one for each existing facet in the WHOQOL- 100) divided into four domains (5).
Concerned with the QOL of the elderly and their caretakers, the WHO created the WHOQOL-OLD from the WHOQOL-100 instrument (7) and, by following the same methodological route, performed a specific assessment for the elderly (8). The WHOQOL-OLD was also aimed at performing a transcultural study, comparing healthy aging and ill aging.
The present study aimed at assessing QOL for elderly women who attended the University of the Third Age in Goiás by applying the socio-demographic and the WHOQOL-OLD and WHOQOL-BREF questionnaires.
Ethical aspects, type of study and location
The study was carried out in accordance with the ethical principles described in CNS/MS Resolution 196/96 (9) and was accepted by the Federal University of Goiás' Research Ethics Committee (protocol CEPMHA/HC/UFG CAAE 165/07). It was a descriptive, cross-sectional study of the population of elderly women enrolled in a course entitled, "University Open to the Third Age" (UNATI) run by the State University of Goiás (UEG) in Goià¢nia, GO. An informed consent was signed by all the participants prior to their being included in the study.
Inclusion criteria, data collection and instruments
Women aged 60 and above who accepted an invitation to participate and answered the questionnaires were included in the study. The sample consisted of 38 females enrolled at the Unati/UEG. The study was carried out during one year and socio-demographic information forms and the World Health Organization Quality of Life BREF (WHOQOL-BREF) and OLD (WHOQOLOLD) instruments were applied. The WHOQOL-BREF is applied when more than one instrument is involved and upon the need to repeat the assessment at different time intervals. It has four domains: 1-physical, 2-psychological, 3- social relationships and 4-environmental.
Created by the WHO Quality of Life Group (10), WHOQOL-OLD is a specific instrument for assessing QOL. WHOQOL-OLD contains questions assessing six domains: 1-sensorial functioning, 2-autonomy, 3-past, present and future activities, 4-social participation, 5-death and dying and 6-intimacy.
Statistical analysis
The data from the questionnaires were entered in a Excel 2003 databank and analysed with SPSS 17.0 statistical software. The descriptive socio-demographic analysis involved presenting tables containing absolute values and percentages. Descartes' Rule of Signs tests were used for determining statistical significance for results regarding the instrument's items assessing QOL prior to and following the period being studied. Wilcoxon's test was used to investigate any difference between domains and between facets at different moments prior to and after the QOL questionnaire being applied.
Cronbach's Alpha coefficient test was used to measure the internal consistency of the questions forming the WHOQOL-BREF and WHOQOL-OLD's domains, values ranging from zero to one (1.0), thus showing the proportionality relationship between the items being assessed. A 95 % confidence level was considered in the tests and a p<0.05 result was considered to be significant.
Descriptive socio-demographic analysis
The socio-demographic characteristics of the elderly women who attended Unati/UEG in Goià¢nia during the one-year study period are shown in Table 1.
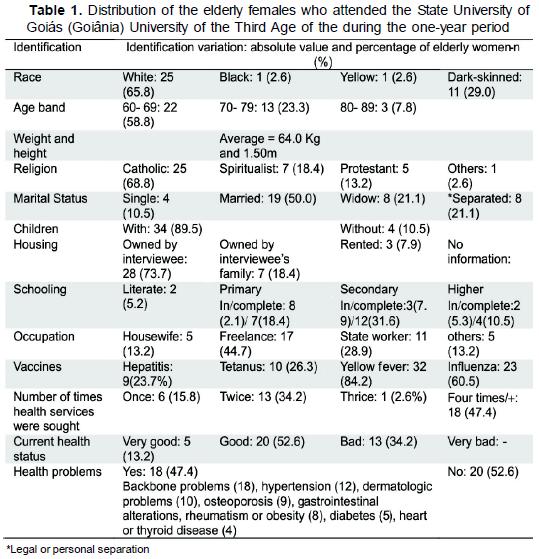
The females evaluated in this study were in the 60 to 69 year-old age band with a predominance of Catholic white women. Regarding the type of vaccines received, yellow fever (84.2 %), followed by influenza (60.5 %), were those mentioned most frequently. The women had sought health services four or five times (47.4 %) and at least twice (34.2 %) a year. As for the type of health problem, 47.4 % mentioned compromised health, with backbone-related problems cited as being the most frequent.
WHOQOL-BREF
Table 2 shows median data (M) and standard deviation (SD) assessed by WHOQOL-BREF used with the elderly women attending Unati/UEG. The medians in the domains ranged from 67.86±2.91 to 58.33±18.00 before and between 57.73±12.00 and 70.72 ± 13.41, afterwards. The lowest median was found in domain 2, before, and in domain 3, on the instrument being applied a second time. The highest score was found in QOL in general (67.86±2.91), before, and in domain 4 (70.72±13.41) following the first application of the QOL evaluation instrument. Differences were found in increased median score regarding the application period (before and afterwards) in domains 2 and 4. However, these differences were not statistically significant (0.184 and 0.100, respectively).
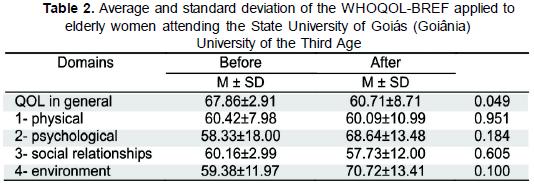
In the QOL general domain, the questions, "How would you assess your quality of life?" and, "How satisfied are you with your life?" were the items which had sthe highest average (0.049 statistical significance).
Despite non-statistically significant values occurring, 0.039 statistical significance was found in individual assessment of the environmental domain, 71.6 % of the women being, "extremely secure in their daily lives," 86.8 % claiming that, "their physical environment is rather healthy," (0.011), and 47.4 % reporting, "average financial means to meet their needs" (0.031).
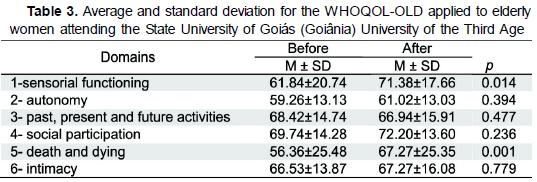
WHOQOL-OLD
Table 3 shows median data (M) and standard deviation (SD) for the WHOQOLOLD instrument which presented medians in the domains ranging between 56.36±25.48 and 69.74±14.28 before, and between 61.02±13.03 and 71.38±17.66 after attendance at Unati/UEG. The lowest median found in the QOL study was found in domain 5, before, and in domain 2, afterwards. There was a significant difference in the increase of the median regarding questionnaire application period (before and afterwards) in domains 1 (p 0.014) and 5 (p 0.001). The highest median found in the QOL assessment instrument results was in domain 4, when it was applied before and after the participants' attendance at the university. It was noted that there was an increase in median score in domains 2, 4 and 6 regarding the QOL assessment instrument; however, this was not a statistically significant increase.
Cronbach's reliability coefficient of the WHOQOL-BREF and WHOQOLOLD
Table 4 shows that WHOQOL-BREF and WHOQOL-OLD were assessed regarding their internal consistencies. The instruments' facets were analysed individually and Cronbach's Alpha coefficient was obtained for 26 and 24 WHOQOL items, respectively.
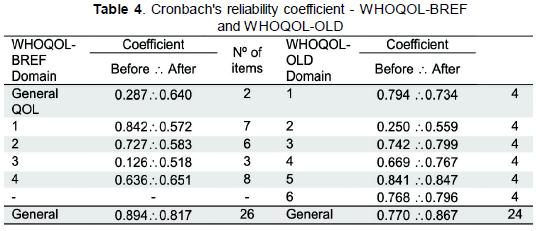
The coefficient for the WHOQOL-BREF module indicated that all the domains and set of items had satisfactory reliability, ranging from 0.126 (3- social relationships domain) to 0.894 (general). Cronbach's reliability coefficients in the WHOQOL-OLD module assumed values ranging from 0.250 (2- autonomy domain) to 0.867 (general).
Cronbach's Alpha coefficient ranges from zero to one (1.0) and the higher the value the more internal consistency is found (i.e. the higher the proportionality relationship in the assessed items indicates homogeneity in measuring the same phenomenon). The social relationships domain showed low coefficient in relation to other α , demonstrating that QOL for the phenomenon assessed in elderly women was not homogeneous between the items investigated by WHOQOL-BREF. Such description can also be inferred in the autonomy domain, great heterogeneity being shown in WHOQOL-OLD for the four items analysed for this population.
Mass vaccination campaigns among more susceptible populations, such as children and the elderly, ensure an acceptable percentage regarding the spread of such diseases as poliomyelitis, tetanus, measles, diphtheria, yellow fever, flu and more recently the so-called swine flu (H1N1 vaccine). The population being studied reported anti-yellow fever and anti-influenza vaccines as being the most sought after by the elderly females in these campaigns. This was probably due to the campaigns implemented by the Ministry of Health against the outbreak of yellow fever and that against flu in Brazil, recommended yearly for 60-year-olds and above.
Elderly women's attendance at health services pointed towards better monitoring of health which could be associated with 52.6 % of the elderly females who described their current health status as being good. It can thus be inferred that the choices related to personal health corroborated with better QOL, despite the identification of bone disorders, chronic degenerative diseases, skin diseases, gastrointestinal disorders and obesity.
No studies were found in the literature about the QOL of the elderly population attending UNATI/UEG (Goiânia). Overall socio-demographic analysis of this population revealed their concern with their health and an improvement of their QOL. The reports of participation in government-instituted campaigns for preventing diseases, as well as the search for specific treatments, are proof of this gender group's aims to reach other age-bands with continuing QOL.
The scope of the WHOQOL-BREF encompasses levels of satisfaction with sleep and sexual life. It is an instrument which assesses general QOL in which issues regarding health condition and physical functioning, such as financial resources, the environment, safety, leisure and entertainment, are directly related (12). Analysing the gender of the population being studied and personal satisfaction within general aspects (QOL in general; see Table 2) showed that the reports by elderly females were relevant and had taken on a major role regarding other domains focusing on physical and psychological issues, social relationships and the environment. Despite the fact that the study did not present statistically significant values in the environmental domain, it should be stressed that QOL depends on the daily construction of people's lives (facets eight, nine and twelve within this domain presented statistically relevant significance). It is worth pointing out that their choices for improving QOL and change of habits not observed before were probably reinforced when they opted to attend the UNATI/UEG for one year (i.e. so reported by this population in the present study).
Concern for the elderly's QOL led the WHO (7,8) to create the WHOQOLOLD, nowadays used by institutions and researchers for compiling data on elderly populations. Applying the WHOQOL-OLD instrument (10) has provided the community with hitherto unknown information regarding elderly women's behaviour. Two domains which stood out in this gender group were sensory functioning and death and dying. Great value was attributed to sensorial functioning, thus demonstrating this population's concern with all aspects related to losing their senses. However, the aspect which stood out the most was found in the items regarding death and dying which showed relevant significance (0.006 difference) in homogeneity of items.
Achieving statistically significant data in only two domains regarding elderly females' QOL through this instrument may be explained by the fact that the population may behave differently in accordance with their anxieties, needs and age-band. This experience regarding target behaviour reinforces the idea that QOL is identified with the importance given to that which brings selfsatisfaction.
Regarding WHOQOL-BREF and WHOQOL-OLD reliability for the assessed population, Cronbach's Alpha values were obtained within the interval proposed for this test. However, some authors (13) have suggested that an above 0.7, but no higher than 0.9, should be considered, as a very high value may mean item redundancy. The present analysis revealed that 57.7 % of the values obtained were within this interval (0.7 to 0.9). However, it was considered that values higher than 0.5 would be within the expected limits and that, therefore, they would demonstrate homogeneity of the items assessed in the domains thus increasing WHOQOL-BREF and WHOQOL-OLD reliability reading elderly women to 88.46 %.
The elderly women aged between 60 and 89 who attended the Unati/UEG presented their own socio-demographic characteristics during the one-year assessment prior to or after having gained access to a university geared towards this type of clientele. It was observed that their desire to keep their health within achievable patterns of income, socialisation and the delivery of health services was considered good.
Analysis of WHOQOL-BREF behaviour revealed that the general domain on QOL played a major role compared to the other domains encompassing physical, psychological and personal relationships and environmental issues. WHOQOL-OLD analysis showed that the sensory functioning and death and dying domains characterised the population regarding their anxieties, wishes and gender-related needs. Cronbach's α coefficient had satisfactory reliability in both WHOQOL-BREF and WHOQOL-OLD, showing assessed item homogeneity for the elderly women who attended the Unati/UEG.
Acknowledgements: We would like to thank Mrs Débora de Sousa Santos for her collaboration in applying the instruments and Mr Carlos Miranda Adorno for the Spanish version of the abstract.
1. Peixoto C. De volta às aulas ou de como ser estudante aos 60 anos. In: Veras RP. Terceira idade: desafios para o terceiro milênio. Rio de Janeiro: Relume-Dumará; 1997. [ Links ]
2. Organização Mundial da Saúde Internet . Available at http:www.opas.org.br. Consulted in Aug 2007. [ Links ]
3. Fleck MPA, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Aplicação da versão em português do instrumento de avaliação da qualidade de vida da Organização Mundial da Saúde WHOQOL-100. Rev. Saúde Publica 1999; 33(2):198-205. [ Links ]
4. Fleck MPA, Leal OF, Louzada S, Xavier M, Chachamovich E, Vieira G, et al. Desenvolvimento da versão em português do instrumento de avaliação da qualidade de vida da OMS WHOQOL-100. Rev Bras Psiquiatr. 1999; 21(1):19-28. [ Links ]
5. Fleck MPA, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Aplicação da versão em português do instrumento de avaliação da qualidade de vida da Organização Mundial da Saúde WHOQOL-bref. Rev Saúde Pública 2000; 34(2):178-183. [ Links ]
6. Whoqol Group. What quality of life? World Health Forum, Switzerland 1996; 17(4):354-356. [ Links ]
7. Fleck MPA, Chachanovich E, Trentini C. Projeto WHOQOL-OLD: métodos e resultados de grupos focais no Brasil. Rev Saúde Pública 2003; 37 (6):793-799. [ Links ]
8. Power MJ, Quinn K, Schmidt S. Development of the Whoqol-Old module. Qual Life Res, Virginia, 2005; 14(10):2197-2214. [ Links ]
9. Ministério da Saúde. Conselho Nacional de Saúde. Manual operacional para comitês de ética em pesquisa. Brasília: Ed. MS; 2002. [ Links ]
10. Whoqol Group. The World Health Organization Quality of Life Assessment (WHOQOL): Development and general psychometric properties. Soc Sci Med. 1998; 46:1569- 1585. [ Links ]
11. Ministério da Saúde. Fundação Nacional de Saúde. Informe Técnico - Campanha Nacioanl do Idoso - 2002. Brasília: MS; 2002 Internet . Available at http://www.funasa.gov.br. Consulted in jul 2010. [ Links ]
12. Zanei SSV. Análise dos instrumentos de avaliação de qualidade de vida Whoqol-Bref e SF- 36: confiabilidade, visibilidade e concordância entre pacientes de Unidade de Terapia Intensiva e seus familiares. São Paulo, 2006. Internet . Available at http:www.teses.usp.br/teses. Consulted in jul 2010. [ Links ]
13. Mcdoweel I, Newll C. Measuring health: a guide to rating scales and questionnaires. 2nd Edition. New York: Oxford; 1996. [ Links ]

