










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista de Salud Pública
Print version ISSN 0124-0064
Rev. salud pública vol.14 no.5 Bogotá Sept./Oct. 2012
Type of delivery and gestational age is not affected by pregnant Latin-American women engaging in vigorous exercise. A secondary analysis of data from a controlled randomized trial
El tipo de parto y la edad gestacional no se afectan por el ejercicio aeróbico vigoroso en mujeres gestantes latinas. Análisis secundario de un ensayo clínico
Diana C. Pinzón1, Katherine Zamora1, Jorge H. Martínez1, María E. Floréz-López2, Ana C. Aguilar de Plata3, Mildrey Mosquera3 y Robinson Ramírez-Vélez4
1 Programa de Fisioterapia. Fundación Universitaria María Cano. Extensión Cali, Colombia.
2 Facultad de Enfermería y Rehabilitación. Universidad de la Sabana. Chía, Colombia.
3 Grupo de Nutrición. Departamento de Ciencias Fisiológicas. Escuela de Ciencias Básicas. Universidad del Valle. Cali, Colombia.
4 Grupo GICAEDS. Facultad de Cultura Física, Deporte y Recreación. Universidad Santoo Tomás. Bogotá, Colombia. robin640@hotmail.com
Received 17 May 2011/Sent for Modification 23 February 2012/Accepted 18 May 2012
ABSTRACT
Objective There is controversy concerning whether exercise during pregnancy may increase preterm delivery risk and type of delivery. The effect of pregnant Latin-American women engaging in vigorous exercise during the second and third trimester was examined regarding type of delivery and gestational age.
Materials and Methods This was a secondary analysis of data from a controlled randomized trial for determining the influence of physical exercise on pregnant women's endothelial function. The study included 35 nulliparous women, gestational week 16-20 attending prenatal care at three tertiary hospitals in Colombia, who were randomly assigned to one of two groups. The experimental group engaged in aerobic exercise involving 55 % - 75 % maximum heart rate for 60 min, three times a week for 12 weeks. The control group engaged in their usual physical activity. Maternal weight, height, weight gain, blood pressure and type of delivery were recorded; gender, abdominal and head circumference (cm), weight (g), height (cm), vitality (Apgar score at 1 and 5 min) and gestational age at the time of delivery (in weeks, days) were recorded for the newborn.
Results There was no difference in type of delivery by the end of the 12-week program (p>0.05), nor regarding newborn anthropometric variables, Apgar score, or maternal variables concerning weight, height, relative weight gain, blood pressure or weeks of gestation (p>0.05).
Conclusion The potential public health benefits of vigorous exercise were enormous. This study supported existing guidelines indicating that Latin-American women may begin or maintain an on-going exercise program during pregnancy.
Trial registration: NCT00741312.
Key Words: Gestational age, exercise, pregnancy, clinical trial (source: MeSH, NLM).
RESUMEN
Objetivo Existe controversia acerca del efecto del ejercicio físico vigoroso (EFV) durante el embarazo por sus posibles consecuencias en el tipo de parto y la edad gestacional. El objetivo de este estudio fue evaluar el efecto del EFV durante el segundo y tercer trimestre, en mujeres gestantes latinas sobre el tipo de parto y la edad gestacional.
Materiales y Métodos Setrata de un análisis secundario de un ensayo clínico controlado en 35 gestantes, asignadas al azar en dos grupos. Grupo experimental (n=18): EFV entre el 55 % y 75 % de la FC max, por 60 min, 3 veces por sem. Por 12 sem. Grupo Control (n=17): actividad física cotidiana y control prenatal habitual. Se registraron en las maternas: peso, talla, ganancia de peso, presión arterial y tipo de parto. En el recién nacido se registró: género, perímetro cefálico y abdominal (cm), peso (g), talla (cm), semanas de gestación, vitalidad (score Apgar al 1 y 5 min), y semanas de gestación.
Resultados No se encontraron diferencias estadísticamente significativas respecto al tipo de parto (p>0,05). Tampoco en las variables antropométricas del recién nacido, ni en las variables maternas: peso, talla, ganancia de peso, presión arterial o semanas de gestación (p>0,05).
Conclusión Los beneficios potenciales en salud pública del efecto EFV durante la gestación son importantes y este estudio favorece que mujeres latinas puedan comenzar o mantener un programa de ejercicios durante el embarazo.
Trial registration: NCT00741312.
Palabras Clave: Edad gestacional, ejercicio, embarazo, ensayo clínico (fuente: DeCS, BIREME).
Several publications over the last decade have reported few negative effects on a healthy pregnant woman's pregnancy regarding her engaging in physical activity (1). Physical exercise during pregnancy could be beneficial to the maternal-fetal unit and prevent maternal disorders occurring, such as hypertension and gestational Diabetes mellitus (2,3). Recent American College of Obstetricians and Gynecologists' guidelines (4) promote vigorous exercise/training for pregnant women (including sedentary ones) due to for its overall health benefits, including decreased risk of gestational diabetes mellitus and improving well-being and quality of life (2).
The U.S. Department of Health and Human Services issued comprehensive guidelines on physical activity and pregnant women in 2008 (5). Healthy women (non-exercisers and moderate exercisers) should begin or continue moderate-intensity aerobic activity during pregnancy, accumulating at least 150 minutes per week (6). Physical activity may reduce the risk of maternal disorders during pregnancy; however, little data is available concerning pregnant Latin-American women's physical activity. For example, Latin-American women have two to four times the risk of developing gestational diabetes mellitus, chronic hypertension, preeclampsia and caesarean delivery compared to non-obese women and non-Latin white women (7).
Obstetricians are hesitant to advise sedentary women to initiate exercise during pregnancy, and nearly half counsel exercisers to reduce their current activity level (8). It has been speculated that obstetricians have not encouraged exercise during pregnancy, partly as a result of a paucity of data regarding fetal safety. Such lack of counseling may have emerged from pregnant Latin-American women's health benefits from exercise and pregnancy-specific benefits such as decreased risk of being overweight and obese, pre-eclampsia, gestational diabetes (9,10) and reduced depressive symptoms (2).
Relevant data from randomized controlled (1,3) trials and controlled pilot training studies (11) (sample size <15 women) and prospective reports on large population samples have suggested no association between vigorous exercise/training during pregnancy and pregnancy outcome (gestational age, risk of preterm delivery, intrauterine growth) (12) in previously physically-active (and thus fit) and usually middle-high-socioeconomic class women (7, 13,14).This randomized, controlled pilot trial was thus undertaken to examine the effect of vigorous exercise/training (during the second and third trimesters of pregnancy) on 35 pregnant Latin-American women regarding the type of delivery and gestational age.
METHOD
Design
This was a secondary analysis of data from a controlled randomized trial designed to determine the influence of physical exercise on endothelial function in pregnant women; its methods have been described in detail elsewhere (9,15). Interested women eligible for the present study were invited to a pre-test including semi-structured interview and assessment at the Cañaveralejo Hospital and Universidad del Valle Biochemistry Laboratory in Cali, Colombia. The first visit was between 12 and 20 weeks' gestation; secondary measures were recorded from a prenatal interview (in the aforementioned primary care centre) or from the clinical history (in the aforementioned hospital's Obstetrics Department by a nurse and a gynecologist). The study was approved by the local institutional review board, prior to initiation (Resolution-022/29-UV). All participants provided written informed consent before entering the study, in accordance with Declaration of Helsinki guidelines (last modified in 2004). A conservative approach was used to estimating sample size (trial registration: NCT00741312) (9, 15). Power calculations were made for primary outcome measures of gestational age, Apgar score, birth weight and length. It was determined that adequate power (>0.80) would be achieved with 24 pregnant women in the training group and 24 pregnant women in the control group. All power computations assumed that comparing baseline to 16-week scores would be tested at the 5 % significance level. All power computations allowed for 10 % dropout over a 26-week period.
Participants
The volunteers were randomly allocated to one of two groups, according to admission order, following a computer-generated randomization list. To guarantee concealment for randomization, each sequential number corresponded to a sealed opaque envelope containing the questionnaires and information regarding the randomization group: experimental group involving supervised vigorous exercise/training (controlled by a physical therapist and a medical doctor) and a control group involving the usual prenatal care. Pregnant women were included if they were nulliparous and had not participated in a structured exercise program beforehand, aged 16-30 years, having a live fetus in routine ultrasound scan, a normal pregnancy and 16 to 20 weeks' gestational age. They were excluded if they had a history of high blood pressure, chronic medical illnesses (cancer or renal, endocrinology, psychiatric, neurological, infectious and/or cardiovascular disease), persistent bleeding after week 12 of gestation, poorly-controlled thyroid disease, placenta praevia, an incompetent cervix, polyhydramnios, oligohydramnios, a history of miscarriage during the last twelve months and diseases which could interfere with participation [following ACSM 2000 (16) and ACOG 2002 recommendations (17)].
Intervention
Experimental group
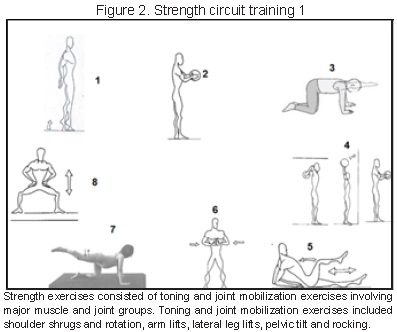
The program's vigorous exercise/training included a total of three (Monday, Wednesday, Friday) 60-minute weekly sessions from the start of the second trimester (weeks 16-20) to the end of the third trimester (weeks 32-36). Thus, an average of ≈32 training sessions was originally planned for each participant in the event of no preterm delivery. All subjects wore a heart-rate (HR) monitor (Polar Electro OY, Finland) during the training sessions to ensure that exercise intensity was light-to-moderate. Each session included regular vigorous exercise/training, involving walking (10 min), aerobic exercise (30 min) (Figure 1), stretching (10 min) (Figure 2) and relaxation exercise (10 min) for 12 weeks (15). All sessions were supervised by a physical therapist, doctor and a physical educator. The exercise-program followed ACSM (16) and ACOG (17) exercise prescription. Adherence to the exercise program was addressed by a physical therapy who supervised the presence of each woman for at least 75 % of the exercise sessions. All sessions were supervised by a qualified physical therapy specialist (working with groups of 3-5 subjects),accompanied by music and held in a spacious, well-lit room in favorable environmental conditions (≈900m altitude, 22-28°C, 50-60 % humidity) to maximize adherence to the training program and its efficacy.

Control group
This consisted of women who would not (usually) carry out any physical exercise during pregnancy and daily-living activities, who would engage in basic daily-living activities (bathing, dressing, eating, walking) without counseling by a physical therapist, 6 sessions, one month (18).
Outcome measure
The study investigators were informed when any woman was hospitalized for delivery and were present to follow-up labor and delivery and collect data. Research assistants having no knowledge of group assignment were designated to determine the following variables in all participants from the prenatal interview (in the aforementioned primary-care centre) or from the clinical history (in the aforementioned hospital obstetrics' department).
Maternal and delivery outcomes
Blood pressure was measured by the auscultatory method at the end of each stage of exercise, up to 6 min. following exercise and delivery, using a mercury column sphygmomanometer. Baseline variables were maternal age, body weight and body mass index (BMI), measured by standard methods (17). Gestational age at the time of delivery (in weeks, days) was recorded from a hospital's perinatal records.
Newborn outcomes
Data regarding condition after birth, Apgar score, etc, were recorded at both hospitals by the midwife or doctor following delivery, using the standard hospital form. The results of the classic Apgar (acronym for appearance (skin color), pulse (heart rate), grimace (reflex irritability), activity (muscle tone) and respiration) test (19) were obtained from the delivery room personnel reports (by nurses) at 1 and 5 min after a baby's complete birth (20). A score of one or two was given for each item, depending on whether it were absent or present(total score could thus range from 0 to 10) (20).
Data analysis
Variable distribution was initially evaluated to verify the two groups' comparability using the Kolmogorov-Smirnov test. A bivariate analysis compared qualitative variables using Yates' X2 test; quantitative data was analyzed using the Mann-Whitney U test. Multiple comparisons were adjusted for mass significance. Significance was established at 5% using SPSS software (v.14.0, SPSS Inc, Chicago, IL).
RESULTS
Participants
The study started in March 2008 and ended in November 2009; 419 of the 483 pregnant women initially eligible for participation were excluded (did not meet inclusion criteria (n=102), declined (n=8), no contact established (n=150) and other reasons (n=95). Therefore, 64 pregnant women were randomized, 33 to the experimental group and 31 to the control group. By the time of the second evaluation (16 weeks' post-intervention and delivery), 15 women discontinued in the experimental group and 14 in the control group (Figure 3). Table 1 gives the baseline characteristics.


Maternal and delivery outcomes
The women's weight gain was similar in both groups. There were no statistically significant differences between pre-exercise resting values and values after intervention (Table 2). There were no statistically significant differences regarding type of delivery between groups (p>0.05) (Table 3).


New born out comes
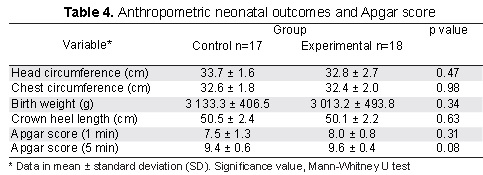
Neonatal results were similar in both groups (Table 4). Mean birth weight was 3,013.2 ± 493.8 grams and mean gestational age was 38.9 ± 2.2 weeks for the experimental group and 3,133.3 ± 406.5 g and 39.0 ± 1.8 weeks, respectively, for the control group (p>0.05). Most new born obtained ≥7 Apgar scores in the first minute in both groups, while all of them obtained ≥9 scores at the fifth minute (Table 4).
DISCUSSION
Secondary analysis of data from a controlled, randomized trial showed that supervised vigorous exercise/training performed during the second and third trimester of pregnancy did not affect the type of delivery and/or gestational age in pregnant Latin-American women. Supervised aerobic exercises, such as those performed by our experimental group, would thus be recommended for improving public health by major medical organizations (4,5,16,17). Other potential benefits of vigorous exercise/ training during pregnancy would include a decreased risk of insulin dependence in overweight women having gestational diabetes mellitus and also better posture, prevention of gestational lower back pain and diastasis recti and strengthening the pelvic floor (1,3,21,22).
Comparing studies, however, was hampered difficult by differences in several variables which could have affected delivery type and gestational age, such as age, BMI, gestational weight gain according to age, previous parity history, smoking habits and alcohol intake. Previous studies' crosssectional (23) or non-randomized (24) nature precluded a true cause-effect relationship from being established between exercise and type of delivery. Only one study (24) showed an association between physical activity and mode of delivery, suggesting a considerably increased risk of caesarean amongst sedentary pregnant women. A etiological mechanisms behind this reported association have yet to be elucidated.
The neonatal results from the present study confirmed the wellbeing of newborn infants born to mothers who initiated vigorous exercise/ training during their pregnancy. This kind of exercise could therefore be recommended for mothers willing to practice some form of physical activity during their pregnancy (25). Babies having suitable weight, gestational age and vitality at birth confirmed the trend reported in the pertinent literature that moderate, vigorous exercise/training has no influence on prematurity or the weight of a newborn infant (26). However, the adequacy of such exercise has to be assured, since engaging in physical activity which is rigorous in terms of its intensity, duration or frequency is associated with low neonatal birth weight (27-29).The results of this study showed that vigorous exercise/training during pregnancy by low-risk women who were previously sedentary was not detriment alto the health of the mother or the child. Clap et al., (30) observed similar results when studying women who engaged in physical activity and either continued or spontaneously stopped exercising (control group) during the first trimester of pregnancy. Regarding birth weight, many studies (1,3, 30) have shown that there is no increased risk of low birth weight for pregnant women who practice leisure-time physical activities. Among the studies which have analyzed vigorous exercise/training as a predictive factor for low birth weight, some (26-30) have shown a subtle association; however newborn mean weight was not inadequate in any of the groups studied. However, other studies (1,3,26-30) have identified some specific activities (e.g. doing laundry standing on one's feet for hours on end) but not regular physical activity in general, as risk factors for inadequate birth weight.
The same has been observed in studies in which the main outcome has been gestational age at delivery (1,3). Many articles either found no association or reported a protective effect for vigorous exercise/training during pregnancy related to premature birth (23-25). Again, some specific activities, like climbing stairs and occupational activities requiring standing for prolonged periods or causing fatigue and requiring agility, have been identified as being risk factors for premature birth (21, 23).
Some of the current study's limitations could be pointed out. The most important one would refer to the practical difficulty of maintaining high compliance with the supervised exercise program, plus the cost of transport three times per week. Around a third of the participants discontinued the program during pregnancy due to logistical and family constraints, including job restrictions, taking care of children and home affairs.
Vigorous exercise or training performed during the second and third trimester of pregnancy did not affect pregnant Latin-American women's delivery type and gestational age in this study. The research adds further evidence to support the overall health benefits of supervised, vigorous regular exercise for healthy pregnant women, involving very few (if any) complications.
Acknowledgements: This work was financed by Universidad del Valle (grant CI 1575). Robinson Ramírez-Vélez received a Ph.D. grant from (Instituto Colombiano para el Desarrollo de la Ciencia y la Tecnología "Francisco José de Caldas") (Colciencias/Icetex agreement 067/2002).
Competing interests: None declared.
REFERENCES
1. Barakat R,Stirling JR, Lucia A. Does exercise training during pregnancy affectgestational age? A randomised controlled trial. Br J Sports Med. 2008;42:674-8. [ Links ]
2. Robledo-Colonia AF, Sandoval-Restrepo N, Mosquera-Valderrama YF, Escobar-Hurtado C, Ramírez-Vélez R. Aerobic exercise training during pregnancy reduces depressive symptoms in nulliparous women: a randomised trial. J Physiother. 2012;58:9-15. [ Links ]
3. Barakat R, Ruiz JR, Stirling JR, Zakynthinaki M, Lucia A. Type of delivery is not affected by light resistance and toning exercise training during pregnancy: a randomized controlled trial. Am J Obstet Gynecol. 2009; 201:1-6. [ Links ]
4. Artal R, O'Toole M. Guidelines of the American College of Obstetricians and Gynecologists for exercise during pregnancy and the postpartum period. Br J Sports Med. 2003;37:6-12. [ Links ]
5. Physical Activity Guidelines Advisory Committee. Physical activity guidelines advisory committee report, 2008. Washington (DC): U.S. Department of Health and Human Services; 2008. [ Links ]
6. Kieffer EC, Carman WJ, Gillespie BW, Nolan GH, Worley SE, Guzman JR. Obesity and gestational diabetes among African-American women and Latinas in Detroit: Implications for disparities in women's health. J Am Med Womens Assoc. 2001;56:181-7 [ Links ]
7. Chasan-Taber L, Schmidt MD, Pekow P, Sternfeld B, Manson JE, Solomon CG, Braun B, Markenson G.J. Physical activity and gestational diabetes mellitus among Hispanic women. Womens Health (Larchmt). 2008; 17: 999-1008. [ Links ]
8. Clarke PE, Gross H. Women's behaviour, beliefs and information sources about physical exercise in pregnancy. Midwifery. 2004; 20: 133–41. [ Links ]
9. Ramírez-Vélez R, Aguilar de Plata AC, Mosquera M, Echeverri I, Ortega JG, Salazar B, Rey JJ, Hormiga C, López-Jaramillo P. Influence of regular aerobic exercise on Endothelium-Dependent Vasodilation and Cardio-respiratory Fitness in pregnant women. J Obstet Gynaecol Res. 2011;37: 1601-8. [ Links ]
10. Ramírez-Vélez R, Romero M, Echeverri I, Ortega JG, Mosquera M, Salazar B, et al. A factorialrandomized controlled trial to evaluate the effect of micronutrients supplementation and regular aerobic exercise on maternal endothelium-dependent vasodilatation and oxidative stress of the newborn. Trials. 2011; 12:60. [ Links ]
11. Klebanoff M, Shiono P, Carey J. The effects of physical activity during pregnancy onpreterm delivery and birth weight. Am J Obstet Gynecol. 1990;163:1450-6. [ Links ]
12. Teitelman AM, Welch LS, Hellenbrand KG, Bracken MB. Effect of maternal work activity on preterm birth and low birth weight. Am J Epidemiol. 1990; 131:104-13. [ Links ]
13. Ramírez-Vélez R, Aguilar de Plata AC, Duperly J, Lobelo F. Effect of Recommended Physical Activity Dose on Obstetrical, Neonatal and Maternal Metabolic Outcomes inPregnant Latina Women. Rev Col Med Fis Rehab. 2012;22 (Supl 1):62-63. [ Links ]
14. Horns PN, Ratcliffe LP, Leggett JC, Swanson MS. Pregnancy outcomes among active and sedentary primiparous women. J ObstetGynecol Neonatal Nurs.1996;25:49-54. [ Links ]
15. Ramírez-Vélez R, Aguilar AC, Mosquera M, García RG, Reyes LM, López-Jaramillo P. Clinicaltrial to assess the effect of physical exercise on endothelial function and insulin resistance in pregnant women. Trials. 2009; 10:104. [ Links ]
16. ACSM's Guidelines for Exercise Testing and Prescription. 6th edition. Philadelphia,PA: Lippincott Williams & Wilkins; 2000. [ Links ]
17. American College of Obstetricians and Gynecologists (ACOG). Exercise during pregnancy and the postpartum period. Committee Opinion 267. Obstet Gynecol. 2002;99:171-3. [ Links ]
18. Taylor HL,Jacobs DR Jr, Schucker B, Knudsen J, Leon AS, Debacker G. A questionnaire forthe assessment of leisure time physical activities. J Chronic Dis. 1978;31:741-55. [ Links ]
19. Apgar V. Aproposal for a new method of evaluation of the newborn infant. Curr Res Anesth Analg. 1953; 32:260-7. [ Links ]
20. Finster M, Wood M. The Apgar score has survived the test of time. Anesthesiology. 2005;102: 855-7. [ Links ]
21. Barakat R, Ruiz JR, Stirling JR, Zakynthinaki M, Lucia A. Type of delivery is not affectedby light resistance and toning exercise training during pregnancy: a randomized controlled trial. Am J Obstet Gynecol. 2009;201: 590.e1-6. [ Links ]
22. Clapp JF 3rd. The course of labor after endurance exercise during pregnancy. Am J Obstet Gynecol. 1990;163:1799-805. [ Links ]
23. Bungum TJ, Peaslee DL, Jackson AW, Perez MA. Exercise during pregnancy and type of delivery in nulliparae. J Obstet Gynecol Neonatal Nurs. 2000;29:258-64. [ Links ]
24. Hall DC, Kaufmann DA. Effects of aerobic and strength conditioning on pregnancyoutcomes. Am J Obstet Gynecol. 1987;157:1199-203. [ Links ]
25. Hatch MC, Shu XO, McLean DE, Levin B, Begg M, Reuss L, et al. Maternal exercise during pregnancy, physical fitness, and fetal growth. Am J Epidemiol. 1993;137:1105-14. [ Links ]
26. Factorsrelated to exercise over the course of pregnancy including women's beliefsabout the safety of exercise during pregnancy. Midwifery. 2009; 25: 430-8. [ Links ]
27. Cavalcante SR, Cecatti JG, Pereira RI, Baciuk EP, Bernardo AL, Silveira C. Water aerobics II: maternal body composition and perinatal outcomes after a program for low risk pregnant women. ReprodHealth. 2009; 6;6:1. [ Links ]
28. Ramírez-Vélez R. A 12-week exercise program performed during the second trimester does not prevent gestational diabetes in healthy pregnant women. [Critically Appraised Papers]. J Physiother. 58 (3);198-9. [ Links ]
29. Mosquera-Valderrama Y, Robledo-Colonia A, Ramírez-Vélez R. Ensayo clínico controlado de la influencia del entrenamiento aeróbico sobre la tolerancia al ejercicio y los síntomas depresivos en primigestantes colombianas. Rev Prog Gine y Obst. 2012;55 (8):385-92. [ Links ]
30. Clapp JF 3rd, Kim H, Burciu B, Lopez B. Beginning regular exercise in early pregnancy: effect on fetoplacental growth. Am J Obstet Gynecol. 2000;183:1484-8. [ Links ]
