










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista de Salud Pública
Print version ISSN 0124-0064
Rev. salud pública vol.14 no.6 Bogotá Nov./Dec. 2012
The impact of under-recording on cervical cancer-related mortality rates in Colombia: an equity analysis involving comparison by provenance
Impacto del sub-registro en la mortalidad por cáncer cervical por procedencia, en Colombia. Un análisis de equidad
Johanna Aponte-González, Carlos Rincón and Javier Eslava-Schmalbach
Clinical Research Institute, Universidad Nacional de Colombia. Bogotá. jaaponteg@unal.edu.co; cjrinconr@bt.unal.edu.co; jheslavas@unal.edu.co
Received 30th April 2012/Sent for Modification 13th June 2012/Accepted 18th July 2012
ABSTRACT
Objective Comparing cervical cancer mortality rates in Colombian departments, as well as in urban and rural areas and examining the potential causes of any differences.
Methodology This was an ecologic study. Mortality due to cervical cancer was estimated from data collected between 2005 and 2008 by the Colombian National Statistics Bureau (DANE).This included overall mortality in Colombia, mortality by department and mortality by rural and urban area. DANE provided theunder-recording indicator for mortality by departments and the unmet basic needs index. Spearman correlation coefficient was estimated for average mortality by department, unmet basic needs and under-recording variables.
Results The overall annual mortality rate from 2005 to 2008 due to cervical cancer in Colombia ranged from 10 to 11.1 per 100,000 females. Mortality reported in urban areas was higher than in rural areas (10.3-11.7 cf 7.6-8.7). The lowest average mortality was reported from the Chocó department (4.7) and the highest from Meta (18.2). An inverse correlation was found between average mortality by department and unmet basic needs. The under-reporting' indicator had an inverse correlation with mortality, meaning that departments having recording issues also reported lower mortality rates.
Conclusions Health systems must adopt strategies designed to improve information systems for supporting decision-making and optimise the use of health resources, particularly for vulnerable populations and populations having unmet basic needs. Comparing mortality amongst departments and areas will not lead to reliable conclusions in such under-recording conditions.
Key Words: Uterine cervical neoplasm, mortality, needs assessment, disease notification (source: MeSH, NLM).
RESUMEN
Objetivo Comparar las tasas de mortalidad por cáncer de cuello uterino en los departamentos de Colombia, tanto en las zonas urbanas como en las zonas rurales y examinar las posibles causas de las diferencias.
Métodos Este fue un estudio ecológico. La mortalidad causada por cáncer de cuello uterino fue estimada a partir de los datos recolectados entre los años2005 y 2008 por el Departamento Administrativo Nacional de Estadística (DANE).La mortalidad global en Colombia, la mortalidad por departamento y la mortalidad por zonas rurales y urbanas fueron incluidas en estas cifras. El DANE proporcionó el indicador del sub registro de la mortalidad por departamentos y el índice de las necesidades básicas insatisfechas (NBI). El coeficiente de correlación de Spearman fue estimada por mortalidad promedio por departamento, NBI y las variables de sub registro.
Resultados La tasa anual de mortalidad global desde el año 2005 hasta el año 2008, causado por cáncer de cuello uterino en Colombia, osciló entre 10 hasta 11,1 por 100.000 mujeres. La mortalidad registrada en las zonas urbanos tenía una tasa más alta que en los zonas rurales (10.3-11.7 cf 7.6-8.7). La tasa más baja de mortalidad promedio fue registrada en el departamento de Chocó (4.7) y la más alta del departamento de Meta (18.2). Se encontró una correlación inversa entre la mortalidad promedio por departamento y las NBI. El indicador del sub registro tenía una correlación inversa con la mortalidad, significando que los departamentos que tienen problemas relacionadas con el registro también registraron tasas más bajas de mortalidad.
Conclusiones Los sistemas de salud deben adoptar estrategias encaminadas a mejorar los sistemas de información para apoyar a la toma de decisiones y optimizar el uso de los recursos sanitarios, particularmente para las poblaciones vulnerables y las poblaciones con necesidades básicas insatisfechas. Al comparar la mortalidad entre los departamentos y las zonas no conducirá a conclusiones confiables en tales condiciones de registro.
Palabras Clave: Neoplasia cervical uterino, mortalidad, evaluación de las necesidades, notificación de enfermedades (fuente: DeCS, BIREME).
According to the International Agency for Research on Cancer (IARC), the data for 2008 shows that cervical cancer (CC) is the third most common cancer in women; 530,000 new cases were estimated for 2008, 85 % of them being attributed to developing countries. High-risk regions included Africa, South Asia and Central and South America; by contrast, North America, Australia and New Zealand were low risk regions (1). Where in lies the difference?
Enough evidence supports sexually-transmitted infection caused by certain types of human papilloma virus HPV), those classified as high risk, as being the main cause of CC (1,2). Consequently, differences in HPV transmission profiles, either due to sexual behavior or to the virus types prevalent in a set population, might provide a first explanation for the differences between developed and developing countries (i.e. sexual behavior favoring HPV infection transmission might increase cancer incidence).
A second explanation would be concerned with the differences regarding CC prevention regarding limitations on screening program coverage and quality, together with barriers against women participating in them. It is known that screening program have reduced CC incidence in developed countries by up to 80 %; however, a similar reduction has not been observed in developing countries (3,4). Colombia has had a national screening-based prevention program since 1990, no observable drop in mortality from CC having been recorded (5).
The IARC has also highlighted differences throughout the regions of the world in terms of mortality/incidence ratio. Whereas this ratio is around 0.3 in the most developed regions, it increases to 0.55 in the least developed, reaching 0.71 in Africa (6). The higher number of deaths due to CC may have resulted from differences in healthcare, either because of failure to make a timely diagnosis, limited access to treatment, or even low-quality treatment.
In view of the above, it may be stated that equity problems may be involved in the high incidence and mortality rates that still prevail in developing countries; 5,500 new cases occur every year in Colombia and 2,045 cervical cancer-related deaths were reported in 2008 (7). Consequently, this work was aimed at identifying inequity issues contributing towards CC mortality rates in Colombia by comparing cervical cancer mortality amongst Colombian departments as well as in urban and rural areas, and then examining potential causes of differences.
This was an ecological study. Records regarding CC deaths were obtained, using C 539 classification according to CIE 10 (malignant uterine cervix tumor, not otherwise specified) discriminated by age-group, department and area of residence (rural or urban) reported by the Colombian National Statistics Bureau (DANE) for 2005 to 2008. Access was obtained to the 2005 population census and demographic forecast for 2006-2008 in Colombia (DANE). Based on 2005 population distribution reported by area for each department, the population estimated in DANE's demographic forecasts for each department was distributed into rural and urban areas for 2005-2008. Under-recording and unmet basic needs (UBN) (2005) indicators were obtained from DANE.
This information was used to estimate the CC mortality rate for every 100,000 women older than 15 for 2005, 2006, 2007 and 2008. The results were broken down by rural and urban area of residence and by department.
The mean CC mortality rate was estimated per year for Colombia and by area of residence; its pattern was described by means of a theme map. Correlation with the unmet basic needs indicator and the under-recording indicator and between these two variables was assessed using Spearman's rank correlation coefficient. PAHO SIGE pi 1.0 and STATA 10.1 software were used for statistical analysis.
RESULTS
Colombia's annual CC-related mortality rate due ranged from 10 to 11.1 for every 100,000 women older than 15 from2005 to 2008. The rural mortality rate ranged from7.6 to 8.8and 10.3 to 11.7 in the urban area. Figure 1 shows the average annual CC mortality rate by department on the theme map.
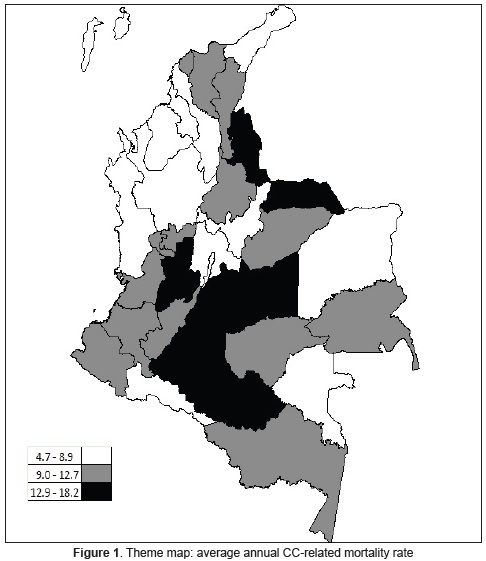
The mean annual CC mortality rate by department ranged from 4.7 (Chocó) to 18.2 (Meta). The departments having the lowest average annual mortality rates were Chocó, Vichada and Boyacá (rates ranging from 4.7 to 8.9); Bolívar, Cundinamarca and Amazonas were the departments having intermediate rates (9 to 12.7) whilst Cesar, Arauca and Meta had the highest average annual CC-related mortality rates (12.9-18.2). Complete data is shown in Table 1.
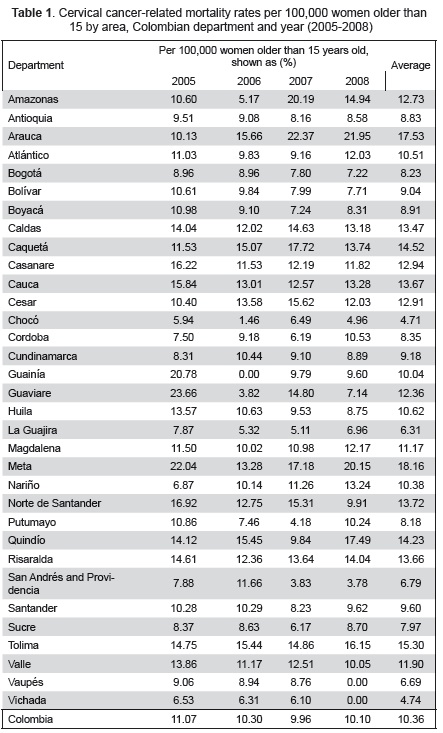
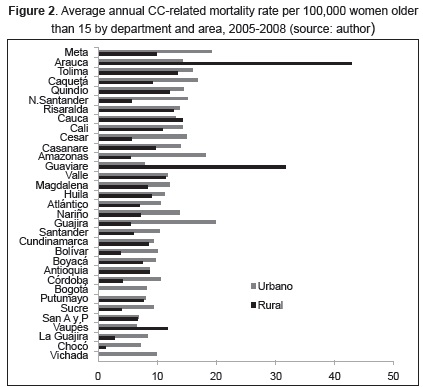
Figure 2 shows average annual mortality rates by department and area. Only four (Vaupés, La Guajira, Cauca and Arauca) of Colombia's 33 departments had higher rural area rates than urban area ones. When comparing the percentage of women living in rural as opposed to urban areas by department, the Guainía, Amazonas, Vichada, Nariño, La Guajira, Córdoba and Chocó departments were worth noting as more than 40 % of their female population lived in rural areas, their mortality rate being 5.8 to 15 deaths less than in urban areas. Interestingly, no CC-related deaths were reported in the rural area of Vichada during the study period, particularly as 53 % of the female population older than 15 live in this department's rural area. This may have suggested a high percentage of deaths being under-recorded in these departments.
A linear correlation was found when comparing average CC mortality rate to the UBN index for 2005, Spearman rank correlation coefficient being -0.4420 (p=0.01). However, correlation was in verse, contrary to what had been expected.
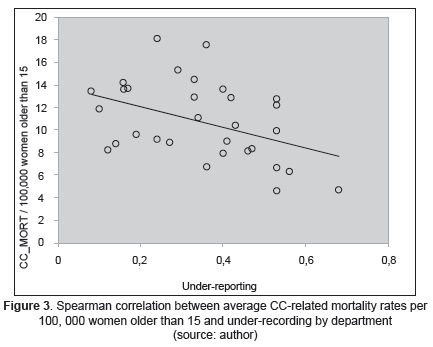
There was a correlation between the under-recording' indicator and mortality (-0.4256; p=0.0135); such inverse correlation meant that departments experiencing greater problems related to recording epidemiological variables also reported lower mortality.
There was a correlation between the under-recording indicator and UBN (Spearman rho=0.8818; p<0.0001). Figure 3 shows the under-recording indicator by department compared to mortality incidence rates by department.
DISCUSSION
This study showed that Colombian CC-related mortality figures gave it a mid-position amongst Latin-American countries. Al though Argentina, Chile and Uruguay reported mortality rates in 2008 which were below the rates obtained in Colombia (8.9, 8.5 and 9.2 per 100,000 inhabitants, respectively), Brazil, Ecuador, Venezuela and Peru reported higher mortality rates (11.4, 12.4, 13.2 and 14.6 per 100,000 inhabitants, respectively). However, compared to European or North-American countries, it was clear that the Colombian CC-related mortality rate was notably high (i.e. 3.2 in Canada and 2.4 per 100,000 in the USA). Switzerland has reported the lowest rate in the world (1.9 per 100,000 inhabitants) (8). In view of the above, Colombia, like all other Latin-American countries, may improve its CC rate by working on lowering the number of deaths from this disease, even more so when considering that the under-reporting found in this study could suggest that mortality records were actually higher.
The Caquetá, Tolima, Arauca and Meta departments reported high mortality incidence, suggesting the need to pay special attention to cervical cancer prevention program and treatment service quality and accessibility in these departments.
Rural areas had lower mortality rates than urban areas; an opposing result was to be expected when health service access was considered for women in urban areas as they should have had easier access to screening and even to treatment. The same was true when comparing the departments' UBN index and their mortality rates, this being contrary to what was expected.
A study in the Antioquia department using 2000-2007 data had already analyzed the relationship between social indicators and mortality due to both CC and breast cancer. It only included Antioquia municipalities and found that CC mortality increased with higher UBN levels and the higher the misery and poverty levels were (9).This result was consistent with the world wide picture where developing countries have reported the highest mortality. However, the results obtained in the present study using data from the whole of Colombia were not consistent with such analysis.
It is worth noting that it has been shown that it is not easy to demonstrate the absence of a relationship between CC prevention program performance in Colombia and CC-related mortality. This was shown by a case-control study in 2010 according to which patient screening charts (participation in the program and follow-up of negative results) showed no definitive correlation with the risk of developing invasive cancer in two of the four departments analyzed. In the departments where no correlation was found, Pap smear quality had been classified as poor.
The authors noted that greater or lower participation in the screening program would have had no effect on the number of CC cases if the cytology test was not good quality to start with (10).
A second aspect which might have explained the results obtained here concerns the sexual behavior of women and men in Colombia's regions and departments. A direct association has been demonstrated between the probability of a woman becoming infected by high-risk HPV types and the number of new sexual partners. It has also been found that although in there is an association between schooling level around the world and the risk of developing cancer (the lower the schooling the higher the risk), no association has been observed between schooling level and the risk of HPV infection. Thus the relationship between cancer risk and schooling level appears not to be mediated by higher infection prevalence in less-educated women, but rather by the early age at which these women begin their sexual activity. Apparently, the latter finding might change HPV potential for causing cancer (11).
The Colombian Demographics and Health Survey (ENDS) for 2010 found that women having a lower educational level and economic status usually started their sexual activity at a younger age. On average, it was found that age for initiating such activity was 17.5 in rural areas compared to 18.1 in urban areas (3). Caquetá, Chocó and Amazonas (where mortality incidence in this study was low)also had the lowest age for initiating sexual activity in Colombia.
Condoms are used to a larger extent in urban areas than rural ones (7.6 % of the women surveyed cf 5.4 %, respectively) (3).
The results obtained in this study appear not to have been logically influenced by these factors. Apart from differences regarding aspects such as the age of sexual initiation and condom use, they were not sufficiently significant to have an effect on CC-related mortality.
The statistically significant and inverse correlation between the under-recording indicator and mortality due to CC suggested that there were problems regarding recording deaths from CC in the departments and that therein lay the reason for this study's results being contrary to what had been expected. This could explain why departments having better recording systems accumulated the highest mortality rates. It would also explain why departments like Chocó and Vichada, having a high proportion of rural inhabitants, had such a low number of deaths from cervical cancer when their records were compared to their own urban areas. The positive correlation between under-recording and BUN reinforced this theory. This study identified a serious problem regarding a lack of adequate information systems in places where vulnerable populations live. This made it difficult to focus on strategies designed to address health problems which have been under-recorded, contributed further to problems of inequity in providing healthcare services and undermined the possibility of addressing system deficiencies through a rational, evidence-based approach. Healthcare systems need to adopt strategies for improving information systems designed to facilitate decision-making with a view to optimizing the use of healthcare resources, in particular for vulnerable populations or populations having issues regarding unmet basic needs.
Further studies should be carried out with close follow-up of recording systems to identify weaknesses and possible solutions. Statistical management of under-recording and data adjustment is also suggested for further analysis since this did not come within the scope of this study
Acknowledgements: We would like to thank the Universidad Nacional de Colombia's Medicine Faculty's. Research Office which sponsored this project.
REFERENCES
1. Sanclemente G, Gill DK. Human papillomavirus molecular biology and pathogenesis. J Eur Acad Dermatol Venereol. 2002;16(3):231-40. [ Links ]
2. Muñoz N. Human papillomavirus and cancer: the epidemiological evidence. J Clin Virol. 2000;19(1-2):1-5. [ Links ]
3. Profamilia. Encuesta Nacional de DemografíaSalud 2010 [Internet]. Available from: http://www.profamilia.org.co/encuestas/Profamilia/Profamilia/index.php?option=com_content&view=article&id=62&Itemid=9. Cited September 2011. [ Links ]
4. Lewis MJ. A situational analysis of cervical cancer in Latin America and the Caribbean. PAHO; 2004. [ Links ]
5. Murillo R. [Cervical cancer control in Colombia: achievements and challenges of cytology based programs]. Biomedica. 2008;28(4):467-70. [ Links ]
6. IARC. Cervical Cancer Incidence and Mortality Worldwide in 2008 [Internet]. Available from: http://globocan.iarc.fr/factsheets/cancers/cervix.asp. Cited April 2012 [ Links ]
7. Instituto Nacional de Cancerología. Todo sobre el cáncer de cuello uterino. Información institucional [Internet]. Available from: http://www.incancerologia.gov.co Cited June 2010. [ Links ]
8. GLOBOCAN 2008. Cancer Incidence, Mortality and Prevalence Worlwide 2008. Cervical Cancer Mortality [Internet]. Available from: http://globocan.iarc.fr/. Cited January 2012. [ Links ]
9. Baena A, Almonte M, Valencia ML, Martínez S, Quintero K, Sánchez GI. [Trends and social indicators of both mortality breast cancer and cervical cancer in Antioquia, Colombia, 2000-2007]. Salud Publica Mex. 2011;53(6):486-92. [ Links ]
10. Murillo R, Wiesner C, Cendales R, Piñeros M, Tovar S. Comprehensive evaluation of cervical cancer screening programs: the case of Colombia. Salud Publica Mex. 2011;53(6):469-77. [ Links ]
11. Johnson AM, Mercer CH, Beddows S, de Silva N, Desai S, Howell-Jones R, et al. Epidemiology of, and behavioural risk factors for, sexually transmitted human papillomavirus infection in men and women in Britain. Sex Transm Infect. 2012;88(3):212-7. [ Links ]
