










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista de Salud Pública
Print version ISSN 0124-0064
Rev. salud pública vol.17 no.1 Bogotá Jan./June 2015
https://doi.org/10.15446/rsap.v17n1.43536
http://dx.doi.org/10.15446/rsap.v17n1.43536
Revisión/Review
Efficacy of the prescription of physical activity in the obese child population
Eficacia de la prescripción de actividad fisica en población infantil con obesidad
Edgar D. Hernández-Álvarez1, María V. Valero-Bernal2 y Erica M. Mancera-Soto1
1 Department of Corporal Human Movement. Faculty of Medicine. National University of Colombia. Bogotá, Colombia. edhernandeza@unal.edu.co; emmanceras@unal.edu.co
2 Department of Public Health, Faculty of Medicine. National University of Colombia. Bogotá, Colombia. mvvalerober@unal.edu.co
Received 17th October 2014/Sent for Modification 15th November 2014/Accepted 9th December 2014
ABSTRACT
Objective To determine the effectiveness of prescribing physical activity to the population of overweight and obese children, in accordance with the levels of evidence.
Methods To find literature pertaining to the intervention of physical activity in overweight and obese children. four electronic databases were used: Pubmed, Embase, Cochrane and Lilacs. The search was conducted with a cut-off date of June 2012. Randomized controlled clinical trials of intervention programs involving physical activity for both overweight and obese children were selected. Two independent researchers reviewed and evaluated the quality of the studies, and extracted intervention and result data.
Results A total of 204 studies were identified. 19 randomized controlled studies which complied with inclusion and exclusion criteria were included. These studies evaluated the impact of physical activity among obese children and compared different types of intervention based on exercise and diet or both with the objective of reducing weight in obese children.
Conclusions It is necessary to conduct studies on obese children with bigger sample sizes to determine the effects of the treatment, and more importantly, to devise comprehensive programs that include a structured exercise program complemented by a dietary program. Likewise, the development of public health policies that allow for the development of national programs for weight and obesity control in Colombian children and adults should be developed, taking into account that the causes of obesity are multiple, including social, familiar, metabolic, and dietary aspects.
Key Words: Child, obesity, overweight, public policy, physical activity (source: MeSH, NLM).
RESUMEN
Objetivo Determinar la eficacia de la prescripción de actividad física en población infantil con sobrepeso y obesidad de acuerdo a los niveles de evidencia.
Métodos Para la búsqueda de la literatura de intervención en actividad física en niños con sobrepeso y obesidad se utilizaron 4 bases de datos electrónicas Pubmed, Embase, Cochrane y Lilacs la búsqueda se realizó con corte de junio de 2012. Se seleccionaron ensayos clínicos controlados aleatorizados de programas de intervención de actividad física en niños con sobrepeso y obesidad. Dos investigadores independientes revisaron y evaluaron la calidad de los estudios y extrajeron los datos de intervenciones y resultados.
Resultados Un total de 204 estudios fueron identificados. Se incluyeron 19 estudios aleatorizados y controlados que cumplieron con los criterios de inclusión y exclusión; los estudios evaluaban en impacto de la actividad fisca en niños obesos en diferentes tipos de intervención basados en ejercicio y dieta o combinados con el objetivo de reducir el peso en niños obesos.
Conclusiones Es necesario realizar investigaciones en niños obesos con tamaños de muestra más grandes para determinar el efecto del tratamiento, y lo más importante, tener programas integrales compuestos de un programa estructurado de ejercicios complementado con un programa dietario. Del mismo modo fomentar el desarrollo de políticas públicas que permitan el desarrollo de los programas nacionales para el control de peso y la obesidad en niños y adultos colombianos, teniendo en cuenta que los determinantes de la obesidad son múltiples, incluyendo una base socio-economica, familiar, metabólica, y la dieta.
Palabras Clave: Niños, obesidad, sobrepeso, política pública, actividad fisica (fuente: DeCS, BIREME).
Child obesity is considered a public health problem worldwide. According to the Pan American Health Organization (PAHO), the rates of overweight and obesity have increased disproportionately throughout the world, especially in the Americas, and with the greatest impact being on children (1). This increase ranges from 11 % to 21 % from the year 1990 to the year 2000 in the child population and in adolescents; in the Americas an increase is observed, with a rise of 24 % in Mexico, 14 % in Chile and 12 % in Peru. The global health risk report refers to the existence of causal chains in the development of non-communicable diseases related to overweight, obesity and physical inactivity (2-4).
It is widely considered that the condition of being overweight and obesity have a multi-causal origin and that varied determinants play a fundamental role: from lifestyles to the weakness of prevention and promotion programs, elements that could be related to, and interact in, the different populations to produce the disease load that is observed in the different regions of the world (5). Additionally, inadequate diet programs and high degree of sedentary lifestyles, among others, contribute greatly to this public health problem (6-9). It has been referenced that practice of regular physical activity is associated with reduced risk of cardiovascular disease and the benefits are greater if started early in life (10).
This research study focuses on determining the efficacy of prescribing physical activity in overweight and obese children under the age of 16, based on evidence levels through a systematic review in randomized clinical trials, through physical activity programs which took into account the following result variables: body mass index (BMI), BMI Z-score and % fat.
MATERIALS AND METHODS
Search strategy and selection criteria
A systematic search of the literature to the end of June of 2012 was undertaken using a highly sensitive search strategy as recommended by the Cochrane collaboration (12). An epidemiologist conducted a literature search on physical activity in overweight and obesess children. To identify the eligible studies, 4 databases were used electronically (Pubmed, Embase, Cochrane and Lilacs). The Mesh and Emtree search terms were related to the population (e.g. children and adolescents with the words child and adolescents) and the intervention (e.g. physical activity, conditioning or physical condition with the words physical activity, and physical condition). They was related with the term obesity, and with the research studies clinical trial, randomized clinical trial or controlled clinical trial.
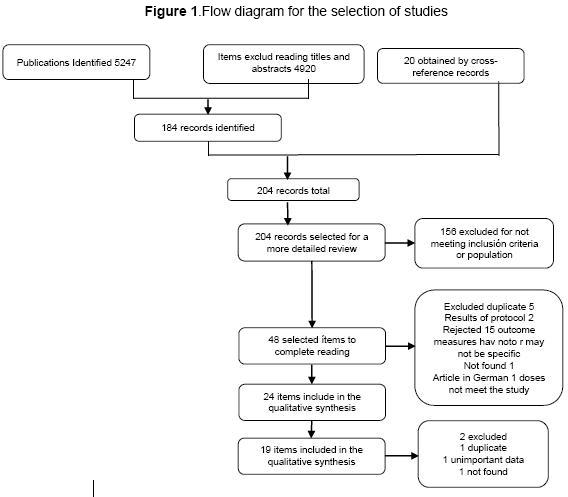
After the electronic search where the data metabase of the National University was used, 2 593 articles were found, distributed as follows: 2 498 in Pubmed, 3 in Cochrane, 12 in Embase, 42 in MEDLINE, and 57 in OVID. (Figure 1) illustrates the suggested selection process, with a final total of 204 references, since 20 records were obtained through cross-references. 156 were rejected given that they did not comply with these criteria or because they were duplicated, triplicated, or were community studies. With the 48 (32-53,54) articles selected, it was found that in the specific analysis, they did not comply with criteria, or were duplicated, leading to 19 definitive articles for quantitative analysis.
Study Selection
Randomized controlled clinical trials published in any language were selected. The target population of the systematic review is overweight and obese children under the age of 16 who are being treated with physical activity prescription programs. According to Tovar and collaborators, overweight and obesity are understood on the basis of three criteria: 1.
WHO-CDC overweight equal to p85 and lower that p95, obesity equal to or greater than p95; 2. International child population suggested by Cole and collaborators: overweight understood as BMI between breaking points for each age; 3. FITNESSGRAM according to body composition with excess fat with normal value of 25 % (11); The type of intervention centered on physical exercise or physical activity in children with overweight and obesity. These programs were based on the prescription of exercise or physical activity employing comparators of no exercise, diet or diet counseling with intervention with duration of no less than three months.
Types of outcome measurements: the studies included in the review must contain one of the primary result measurements as base measurements and post intervention. The self-reporting measurements of size and weight will not be taken for the study; the primary determined sizes were overweight and obesity estimates of participants of the study, with calculation of body mass index (BMI), BMI Z score and % fat.
Data extraction and quality assesment
For data evaluation of the revision, two independent researchers participated by revising and evaluating the quality of the studies, and extracting intervention data and results. The researchers evaluated the methodological quality of the studies included in the Cochrane revision manual (12), where risk bias is evaluated through 6 main criteria: randomness; concealment; blindness of staff, patients and result evaluations, incomplete result data and selective reporting of data. In the case of any differences between the researchers, these were resolved on the basis of consensus.
Analysis Plan
Three principal variables —BMI, Z score BMI and % fat— were registered as they appeared in the initial or basal measurement in each study and post intervention, both for the control group and the treatment. They were registered in terms of mean or mean differences. In those articles reporting the mean, the mean difference was calculated. Mean difference and its standard deviation were attained. In those studies where standard error or reliability interval was reported with non- standard deviation, this deviation was calculated using the formulas suggested in the Cochrane manual (12). With the analysis matrix developed as reported in continuous measurements, mean difference was calculated with a reliability interval of 95 % (95 % CI) using a randomized effects´ model in Revman5.1 (12). With this software the presence of homogeneity and heterogeneity was established. For this the statistics of I2, and Chi squared (Chi²) with its degrees of freedom and value P, were used. The magnitude of the effect of the measurement was established according to criteria suggested by Cohen in accord to size of effect, where 0.2 is a small effect size, >0.5 is a medium size effect, and >0,8 is a big size effect. For heterogeneity of studies Galbraith graphs with EPIDATA (13) were used to identify the studies contributing most to heterogeneity. Depending on what was obtained, an analysis by subgroups was conducted to observe how each group behaves with the studies that contribute with the greatest homogeneity, determining the magnitude of the effect in each.
RESULTS
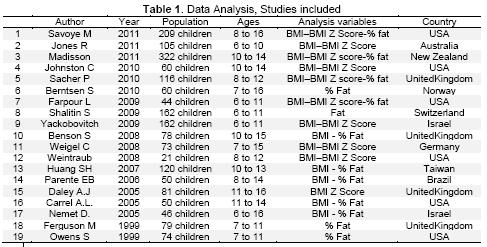
In the data analysis, 19 articles from different regions of the world were included, 6 of which were from the United States, 4 from the United Kingdom, 2 from Israel, and 1 from Norway, Switzerland, Germany, Australia, Taiwan, New Zealand and Brazil respectively (14-32). These comply with obesity inclusion criteria, age ranging from 5.5 to 16, with an average age of 10.53. The total population among all the studies was 1 406 children, 742 in intervention group, and 664 in control group (Table 1).
The analysis of the 19 studies included in the revision was conducted. Three major groups were found. In the first group, exercise versus no exercise, a total of 10 studies was included, based on a procedure focused on a treatment group with physical exercise.
The program had specific prescription criteria, versus a control group that did not do exercise (14,17-22,26,30,31). In the second group, exercise plus diet versus diet, 6 studies were included that focussed on a treatment group with a specific exercise program plus diet with a kilo-caloric balance versus a group which was only subject to diet control or kilo-caloric balance or diet counseling (15,24,25,27,29). In the third group, 3 studies were included focusing on a treatment group that had a specific exercise program versus a control group subject to diet or exercise counseling as the principal recommendation for weight control (16,23,32).
Quality Evaluation and Risk of Bias
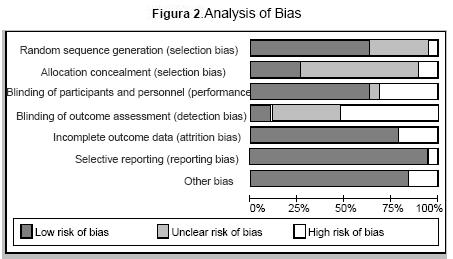
It is important to highlight that methodological weakness was found in all 19 studies given that some do not comply with quality criteria established in the evidence. The 19 studies are randomized clinical trials but they have problems related to sample sizes, given that they were small, affecting size effect measurement. In regard to evaluation criteria of bias it was found that 100 % of the studies conducted a randomness process having low risk, but 30 % within this 100 % refer to the fact that it was conducted but does not explain clearly the method or manner in which the procedure was followed. In the concealment process a significant deficiency was found; only 20 % report some concealment process, 40 % are not clear and the rest do not refer to it at all. With regard to staff and individual masking, the studies refer to performing it, but very few, only 10 %, refer to results masking. Another weakness regarding the quality of the studies found was that researchers refer to lost or imputed data, not referring to data management after their loss Figure 2.
Heterogeneity analysis
One of the problems presented in the articles was heterogeneity between the protocols used among them and between time spaces in which results were reported. In some cases comparators among protocols were not equal and the timing of outcome measures varies between three to six months or more. As the three subgroups were identified, heterogeneity among the studies was established. In order to do this, three basic procedures were used to determine statistical heterogeneity. The latter required establishing dispersion among the studies in the tree diagram, the relation among the reliable intervals of the studies in the different groups, and finally calculating heterogeneity indexes.
Results according to the BMI variable
15 of the 19 studies reported mean difference data at baseline and after treatment in this variable. It is important to note that there is good consistency among 10 of the 14 studies, which show a result in favor of the main treatment in each group. What was specifically found, however, was that in the first group (exercise plus diet versus diet), 6 studies showing high heterogeneity were included. This was because reliability intervals among the studies are dissimilar. Some overlap – not all, which allows for observing first hand that heterogeneity exists. Secondly, dispersion is observed among the studies, reporting an index of I2 of 85 % Chi² of 32.98 at 5 degrees of liberty with a P-value of 0.0001. Similarly, in the second and third groups (exercise versus no exercise), 6 studies were included. These showed heterogeneity I2 of 84 % Chi² of 36.98 at 5 degrees of liberty, P-value of 0.0001; in the third group (exercise versus counseling) 3 studies are included. In this case, heterogeneity was greater I2 of 84 % Chi² of 28.85 at 2 degrees of liberty P value 0.00001.
Results according to the BMI Z score variable
10 out of 19 studies reported mean difference data at baseline and after treatment. In this group there is less consistency among studies. Heterogeneity is also reported. In this variable, for all three groups, dispersion of studies is high in the tree diagram. In the first group of exercise plus diet versus diet, 4 studies were included, which reported heterogeneity I2 of 76 % Chi² of 12.75 at 3 degrees of liberty, P-value 0.00001, which indicates high heterogeneity among the studies. In the second group, exercise versus no exercise, 3 studies were included, reporting heterogeneity I2 of 96 % Chi² of 51.74 at 2 degrees of freedom; in the third group, exercise versus counseling, 3 studies were included. Heterogeneity in this case is greater, I2 of 83 % Chi² of 12.05 at 2 degrees of freedom, P-value 0.002.
Results according to percentage fat variable
13 out of 19 studies reported mean difference data at baseline and after treatment. It is found that only two of the subgroups contributed studies for analysis and it is observed that these have good consistency among them. 11 out of 12 show a result which supports the principal treatment in each group. The two groups in this variable are exercise plus diet versus diet, and exercise versus no exercise. In this variable, dispersion of the studies in the tree diagram is also found, as well as ample intervals which do not overlap, I2 of 94 % Chi² of 52.88 at 3 degrees of freedom, P- value 0.00001, which indicates high heterogeneity among the studies. The population in this group is of 211 for the experimental group and 175 for the control group. For the evaluation in the second group, exercise versus no exercise, 9 studies were included, reporting heterogeneity of I2 of 59 % Chi² of 19.30 at 8 degrees of freedom, P value 0.01, indicating average heterogeneity of the studies.
DISCUSSION
The studies show great consistency among them towards the intervention with physical exercise in each subgroup, and they shed important results from a clinical standpoint. Within these results, it is noteworthy that the most effective scheme to attain a reduction in obesity among obese and overweight children comes from the scheme based on exercise plus diet versus diet, indicating the need for an integral program composed of structured exercise with clear prescription variables: intensity, duration, frequency and time complemented by a diet with specific hypo-caloric dietary prescription.This combined with exercise favors a weight reduction among children. Discarding the studies that generated higher heterogeneity, a high effect above 0.8 is observed, which according to Cohen, explained by Cochrane's manual, generates the modification of BMI and % fat. In these groups working with an exercise intensity of between 65 to 70% of maximum VO2 or of cardiac frequency, with duration of 40 to 60 minutes three times per week, with an aerobic work routine and resistance with duration of over three months, is suggested.
The latter ought to be complemented with a hypo-caloric diet of 1500 to 1800 kilocalories. This study showed that the effect of exercise only programs was lower, at over 0.6 for the BMI variable, and 0.8 for % fat, but it must be understood that the programs are consistent, though they display high heterogeneity among them. It must be highlighted that programs based only on exercise of varying types and intensity do not have as much effect as the integral program. All of the above is correlated with the data shed by the systematic review and meta-analysis of McGovern's study (33), which demonstrates the effectiveness of the pediatric treatment for obesity, and conducts the analysis on 4 types of interventions for obese children: pharmacological treatment, physical activity, diet, and combined treatment. In this review it shows that the two most important treatments are the combined treatment with an effect of -1.01 and 0.7 respectively. It does, however, show that the pharmacological treatment has a short-term effect on BMI, whereas the physical exercise treatment has an effect on weight loss, particularly on adiposity but not on BMI. It shows that the combined treatment generates greater changes when the focus is on exercise and diet.
This specific program must consider a sub maximal intensity with a duration of over 40 minutes, which would allow the usage of lipids since it would work over the aerobic threshold, inducing hormonal liberation of cortisone, noradrenaline and the growth hormone. This would allow greater access to the usage of fatty acids, which is correlated by the findings obtained by Slentz (34) where with different exercise programs adults show the modification of lipoproteins with exercise programs that have different types of high or medium intensity.
Limitations of the study
We analyzed 19 randomized controlled trials and their level of evidence but it has limitations given that access to all selected articles was not achieved. Difficulties also stemmed from the diversity within programs and from the difference in methods employed; one of the major difficulties was the heterogeneity among the studies.*
Conflict of interest: None.
Acknowledgements: A token of gratitude to the DIB and to the National University for its financing (code QUIPU. 202010016842). A token of gratitude to the Central Library of the National University for its support. The protocol of this research study was revised and approved by the committee for the Master's Program in Clinical Epidemiology of the National University. The findings presented only represent the statements of the researcher and not those of the National University of Colombia.
REFERENCES
1. Report on Health in the World 2008: Primary Health Care, Now More Than Ever. World Health Organization. 2008; 154. [ Links ]
2. Enrique J. The Obesity epidemic in the Americas; Making healthy choices the easiest choices. Rev Panam Salud Publica. 2004; 15(4): 278 -284. [ Links ]
3. The WHO Multicentre Growth Reference Study (MGRS): rationale, planning, and implementation. International Nutrition Foundation for UN University Press. 2004;89. [ Links ]
4. Prevention and control of non-transmissible diseases: Worldwide strategy application. Report of the Secretariat. World Health Organization. 2008; 22. [ Links ]
5. Goran MI, Reynolds KD, Lindquist CH. Role of physical activity in the prevention of obesity in children. International Journal of Obesity. 1999; 23(3):18-33. [ Links ]
6. Worldwide Strategy on Meal Plans, Physical Activity and Health. In Geneva admdRyd, annexes SaludOAMdl. Resolución WHA57. 17 World Health Organization. 2004. [ Links ]
7. Rena K. The epidemic of obesity in children. Cent Eur J Publ Health 2006; 14(4): 151-159. [ Links ]
8. Hawkins SS, Law C. A review of risk factors for overweight in preschool children: a policy perspective. Int J Pediatr Obes 2006; 1(4): 195-209. [ Links ]
9. Margot S. Overweight and obesity among children and youth. Health Reports 2006; 17(3). [ Links ]
10. Hernández J, Herazo Y, Valero M. The frequency of cardiovascular disease-associated risk factors in a university student population. Revista de salud pública 2010; 12 (5): 852-864. [ Links ]
11. Tovar R, Jimenez A, Perez ME, Armendariz AL, Bacardi M. Intervention programs to promote physical activity in school children: systematic review. Nutr Hosp 2011; 26(2): 265-70. [ Links ]
12. Higgins JPT GS. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration, 2011; [Internet]. Available in: http://www.cochrane-handbook.org/. Consulted december 2014. [ Links ]
13. (Ed.) LJ. EpiData Software - 2008. [Internet]. Available in: http://www.epidata.dk/credit.htm. Consulted december 2014. [ Links ]
14. Benson AC, Torode ME, Fiatarone Singh MA. The effect of high-intensity progressive resistance training on adiposity in children: a randomized controlled trial. Int J Obes 2008; 32(6): 1016-27. [ Links ]
15. Savoye M, Shaw M, Dziura J, Tamborlane WV, Rose P, Guandalini C, et al. Effects of a weight management program on body composition and metabolic parameters in overweight children: a randomized controlled trial. JAMA 2011; 297(24): 2697-704. [ Links ]
16. Jones RA, Collins CE, Morgan PJ, Steele JR, Warren JM, Baur LA, et al. The HIKCUPS trial: a multi-site randomized controlled trial of a combined physical activity skill-development and dietary modification program in overweight and obese child. BMC Public Health 2007; 31(7): 1-9. [ Links ]
17. Daley AJ, Wright NP, Wales JK. Sheffield Obesity Trial (SHOT): a randomised controlled trial of exercise therapy and mental health outcomes in obese adolescents. BMC Public Health 2005; 5(113): 1-9. [ Links ]
18. Carrel AL, Clark RR, Peterson SE, Nemeth BA, Sullivan J, Allen DB. Improvement of fitness, body composition, and insulin sensitivity in overweight children in a school-based exercise program: a randomized, controlled study. Arch Pediatr Adolesc Med 2005; 159(10): 963-68. [ Links ]
19. Nemet D, Barkan S, Epstein Y, Friedland O, Kowen G, Eliakim A. Short- and long-term beneficial effects of a combined dietary-behavioral-physical activity intervention for the treatment of childhood obesity. Pediatrics 2005; 115(4): 443-49. [ Links ]
20. Ferguson MA, Gutin B, Le NA, Karp W, Litaker M, Humphries M, et al. Effects of exercise training and its cessation on components of the insulin resistance syndrome in obese children. Int J Obes Relat Metab Disord; 1999; 23(8): 889-95. [ Links ]
21. Owens S, Gutin B, Allison J, Riggs S, Ferguson M, Litaker M, et al. Effect of physical training on total and visceral fat in obese children. Med Sci Sports Exerc 1999; 31(1): 143-48. [ Links ]
22. Sacher PM, Kolotourou M, Chadwick PM, Cole TJ, Lawson MS, Lucas A, et al. Randomized controlled trial of the MEND program: a family-based community intervention for childhood obesity. Obesity (Silver Spring) 2010; 18 Suppl 1: 62-68. [ Links ]
23. Johnston CA, Fullerton G, McFarlin BK, Poston WS, Haddock CK, Reeves RS, et al. Effects of a school-based weight maintenance program for Mexican-American children: results at 2 years. Obesity (Silver Spring, Md.) 2010; 18 Suppl 3: 542-547. [ Links ]
24. Yackobovitch M, Nagelberg N, Phillip M, Ashkenazi L, Hershkovitz E, Shalitin S. The influence of diet and/or exercise and parental compliance on health-related quality of life in obese children. Nutr Res 2009; 29(6): 397-404. [ Links ]
25. Shalitin S, Ashkenazi L, Yackobovitch M, Nagelberg N, Karni Y, Hershkovitz E, et al. Effects of a twelve-week randomized intervention of exercise and/or diet on weight loss and weight maintenance, and other metabolic parameters in obese preadolescent children. Horm Res 2009; 72(5): 287-301. [ Links ]
26. Berntsen S, Carlsen KH, LødrupCarlsen KC, PollestadKolsgaard ML, Joner G, Anderssen SA. Obese children playing towards an active lifestyle. Int J Pediatr Obes 2010; 5(1): 64-71. [ Links ]
27. Farpour NJ, Aggoun Y, Marchand LM, Martin XE, Herrmann FR, Beghetti M. Physical activity reduces systemic blood pressure and improves early markers of atherosclerosis in pre-pubertal obese children. J Am Coll Cardiol 2009; 54(25): 2396-406. [ Links ]
28. Weigel C, Lederer P, Dötsch J, Rascher W, Knerr I. Childhood obesity: concept, feasibility, and interim results of a local group-based, long-term treatment program.: J Nutr Educ Behav 2008; 40(6): 369-373. [ Links ]
29. Huang SH, Hsieh KS, Ou SF, Lin CC, Chien KJ, Liu PY, et al. Effects of a classroom-based weight-control intervention on cardiovascular disease in elementary-school obese children. Acta Paediatr Taiwan 2007; 48(4): 201-206. [ Links ]
30. Weintraub DL, Tirumalai EC, Haydel KF, Fujimoto M, Fulton JE, Robinson TN. Team sports for overweight children: the Stanford Sports to Prevent Obesity Randomized Trial (SPORT). Arch Pediatr Adolesc Med 2008; 162(3): 232-37. [ Links ]
31. Parente EB, Guazzelli I, Ribeiro MM, Silva AG, Halpern A, Villares SM. Obese children lipid profile: effects of hypocaloric diet and aerobic physical exercise. Arq Bras Endocrinol Metabol 2006; 50(3): 499-504. [ Links ]
32. Maddison R, Foley L, Ni Mhurchu C, Jiang Y, Jull A, Prapavessis H, et al. Effects of active video games on body composition: a randomized controlled trial. Am J Clin Nutr. 2011;94(1):156-63. PubMed PMID: 21562081. Eng. [ Links ]
33. McGovern L, Johnson JN, Paulo R, Hettinger A, Singhal V, Kamath C, et al. Clinical review: treatment of pediatric obesity: a systematic review and meta-analysis of randomized trials. J Clin Endocrinol Metab 2008; 93(12): 4600-605. [ Links ]
34. Slentz CA, Johnson JL, Bateman LA, Tanner CJ, McCartney JS, Duscha BD, et al. Inactivity, exercise training and detraining, and plasma lipoproteins. STRRIDE a randomized, controlled study of exercise intensity and amount of publication. J Appl Physiol 2007; 103(2): 432-442. [ Links ]
