











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkMalaria persists as the major global public health problems. Traditionally, solutions have centered on biological approach, such as treating the parasitic infection and vector control, without taking socio-economic and environmental factors into account. This paradigm has proved to be insufficient for advancing control strategies and progressive elimination. The main challenge has been early diagnose and prompt treatment. Unfortunately, failure treatment in clinical cases and adhesion to radical treatment affect the process, outcome and impact indicators of control programs.
In Latin America, the first chloroquine resistance case was registered in Tumaco, Colombia in1960. 1,2. One possible factor contributing to the spread of drug resistance in the region was the frequency of presumptive treatment for all febrile cases without follow up, and not radical treatment for all positive confirmed cases 3,4, by first Eradication Era . More recently the failures treatment are associate to poor treatment adherence and self-medication with natural herbs as a consequence of limited access to health malaria services 5.
New global malaria elimination efforts guided by the WHO’s Global Technical Strategy (WHO, 2015) and Roll Back Malaria Initiatives_RBI’s action and investment framework 6 (RBM 2015) point to several key elements, including better knowledge of malaria epidemiology patterns at different endemic levels, which can be used to estimate the potential impact of novel malaria reduction strategies 7-9.Integrated strategies tailored to specific endemic settings, such as combined therapies, intermittent preventive treatments (IPT),and rapid diagnostic testing 10, have been shown to reduce case-fatality rates associated with P. falciparum.11-13. However, this is not the case for P. vivax, owing to its dormant forms in the liver and the possibility of relapse, and to the reservoir of asymptomatic cases. In addition, the high rates of mixed malaria infections in countries like Colombia limit the possibilities for elimination. Mixed malaria infections are widely correlated with inadequate treatment and self-medication, with limited quality control strategies for blood samples, and with considerable difficulties accessing health services, thereby preventing patient control during the pathogenic period 14,15.
In Latin America, global pre-elimination and elimination strategies have led to the introduction of various integral strategies at three levels: parasite, host, and vector 16,17. In this context, (i) few studies have considered the impact of asymptomatic cases on the basic case reproduction rate (Ro), and (ii) there is still a need to define and quantify the proportion of fever attributable to malaria and its implications for elimination in different endemic settings 18,23. The purpose of this study was to explore the association between malaria infection and fever as a potential way of tracking progress towards malaria control and elimination in low endemic areas and to compare the changes in species’ transmission patterns. The level and distribution of symptomatic and asymptomatic cases was assessed and findings correlated to potential transmission risks as a basis from which to develop improved models of control and elimination in Colombia.
METHODS
The study was conducted in two endemic areas in Colombia: Nariño and Cordoba, Pacific and Caribbean coast. Blood samples were obtained from urban and rural areas in San Andres de Tumaco (1°48′24″N 78°45′53″W) and the Olaya Herrera (2°20′49″N 78°19′32″W), Nariño. This region is endemic for falciparum malaria around 80% and Afro-Colombian population. In Cordoba, the study concentrates on Puerto Libertador (7°53′17″N 75°40′18″W) and the Montelibano (7°58′16″N 75°25′05″W), both endemic areas for vivax malaria and high prevalence of transmission of other vector borne diseases. Cordoba department registers 9% of total positive cases according to the National Malaria Surveillance System of Colombia24.
A complementary qualitative systematic review was conducted, using Embase, Pubmed, and Bireme databases, period 2000-2015. Search terms included asymptomatic, fever attributable to malaria, elimination, eradication and control of malaria in South America and Colombia. Search equations were elaborated to obtain more precise information related to malaria elimination and control indicators. The references were captured in Endnote X7. Duplicate records were eliminated. Each abstract meeting the inclusion criteria were selected for analyses of frequency and association measures.
Cross sectional surveys conducted in 2011 and 2014 were compared to 1995 historical cross sectional survey data for San Francisco village 25. This dataset was presented by the World Malaria Atlas (26), and it was classified as area of high endemic risk (API > 100 per 1000 in habitants); unfortunately, this village, disappeared due the long period of political unrest, making no feasible additional studies 5,27.
Local malaria control program verified village with current evidence of autochthones cases. Each village was invited to participate and after writing consent the study was conducted. Sampling by convenience was done, and participants located in each information post with help of local leaders. Protocols of security for humanitarian mission were activated according to particular conditions. From each volunteer a capillary blood sample was taken one for a thick blood smear, and for Rapid Diagnose Test, RDT, manufactured by Standard Diagnostic Inc. Asymptomatic cases were defined as any person without symptomatology compatible to malaria, but showing a positive RDT. Fever was defined as any patient with more than or equal to 38,0 Celsius degrees according to WHO Guidelines. Treatment of malaria episodes: individuals with malaria infections were treated according to malaria guidelines of the National Control program in Colombia 28,29. In Latin America a case of malaria is defined as all patients with or without symptomatology and positive presence of parasites. The descriptive statistics and association were estimated using Stata 13. The level of significance was at 5 %.
Ethical considerations
The study was undertaken according to the principles of the Helsinki declaration and Resolution 8430 of the Ministry of Health of Colombia, 1993.The study was cleared by the Ethical Committee, of the Faculty of Medicine at the Universidad Nacional de Colombia. Informed consent was obtained from all study participants. For volunteers less than 18 years old, the parents or legal guardian authorized participation (Articles 23 and 24 of Resolution 8430). According to national norms, the investigation was classified of minimal risk (Article 11).
RESULTS
A total of 528 subjects were sampled. Table 1 shows the prevalence of positive cases, defined as infected with or without symptomatology.
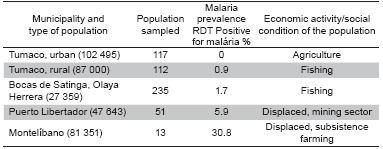
The villages selected for the study experienced intense political unrest and had a high proportion of displaced populations, mainly in Cordoba, on rural areas. According to CODHES, Colombia recorded five million displaced people by 201330. From field observations the self medication was confirmed. The consumption of herbal infusions to reduce fever is very common in all areas. In Tumaco, people prepare infusions of Cinchona Bark while all drug stores close to the temporary field station sold the tonic, “Arquin”, each 100 ml containing 0.566g of chloroquine. Given the limited diagnostic services in the area and the cost of transport to a well-equipped health center, most people with fever or malaria-compatible symptomatology take these available products.
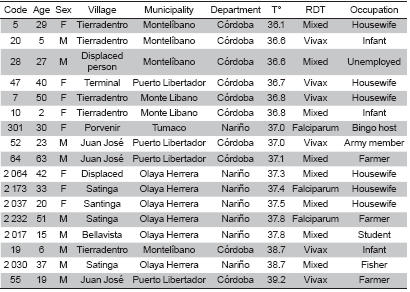
Table 2 shows the demographic and clinical characterization of the detected malaria cases. Prevalence did not differ by sex or occupation. The findings suggest that P.vivax and mixed infections are a key public health problem in those areas. The age distribution of cases kept the historical epidemiology for these areas. The ages affected by the infection and disease are grouped between 15-45 yrs. However, 70 % of infected subjects were asymptomatic and the proportion of fever attributable to malaria was 42 %.
San Francisco Village study: Historical comparison, 1995
This Village was located on Tumaco rural area, over the Rosario River. A total of 1,685 thick blood smears were taken. 41(2.4 %) patients reported fever, i.e. temperature > 38o C, and 151 (8.9 %) tested positive for parasites microscopically (6.2 % P. falciparum and 2.3 % P. vivax). The total proportion of positive cases in febrile episodes was 86 % (19/22) and 8.7 % (132/1,512) in afebrile subjects. The crude odds ratio of the association fever/parasitaemia was 9.9 (95 % confidence intervals, CI, 5.2 %-18.7 %, p-value <0.001). After adjusting for age and sex, the OR was 10.8 (95 % CI 5.6-20.8, p-value <0.001).The crude proportion of fever attributable to malaria (PAF) was a 41.7%(95 % CI 31.3%-55.3 %) and 42 % (95 % CI, 38.1-44.1, p-value<0.001) after adjusting for age and sex 31.
On this particular survey fever due by malaria increased with the level of parasite density and, consequently, the frequency of fever associate to malaria decreases with age 31. After adjusting for age and sex, the odds of fever was 12.1 times higher among individuals exposed to Plasmodium vivax malaria parasites compared to those who were not exposed. Although, a high association was also observed among those exposed to Plasmodium falciparum malaria, OR=11.4, it was slightly lower. However, the proportion of fever attributable to Plasmodium falciparum was 33.2 % higher than the fraction of fever attributable to Plasmodium vivax, where the proportion of fever attributable to malaria was =16.4 %31.
During the last 20 years, there is a slightly reduction of asymptomatic and the PAF. The population of San Francisco was in the middle of all actors in the armed conflict and additional surveys were not possible; however the other regions sampled keep similar epidemiological conditions and same socio-economic factors which affect Tumaco and the Pacific coast endemic areas.
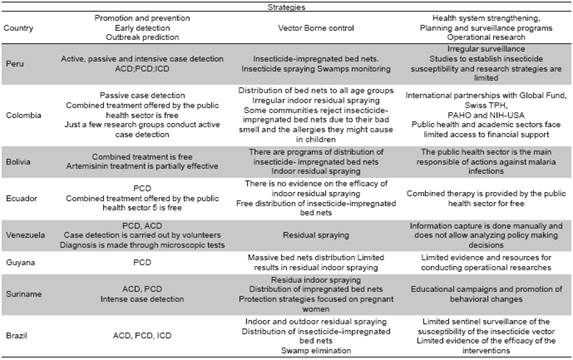
Table 3 presents most relevant aspects of the malaria control program of the eight countries on the same Amazon Region where Colombia also share similar eco-epidemiological conditions. These findings suggest limited actions of surveillance and budget constraint. The case detection in some areas combine intensified active case detection. The activities are responsibility of the public sector, the review do not find the private health sector participation in most of the countries. The surveillance system in Colombia and other countries present data from years before 2013, there is not available data for more recent years. The surveillance system is not opportune and sensible in case detection. It is widely suggest levels of under report around 35 % 15.
DISCUSSION
The findings show that P. vivax malaria is still endemic in Cordoba, while P. falciparum continues to be the main problem in Tumaco. The frequency and distribution of P. vivax and mixed infections indicate a weak effectiveness of malaria treatment in terms of prescriptions, delayed access and limited supervision by health system. As other authors refer, Plasmodium vivax represents de 80 % of clinical malaria cases in Latin America and the Caribbean Island, meanwhile Plasmodium falciparum remains as a main cause of mortality 6 deaths per 100 000 inhabitants 32,43
Policies and strategies for moving from malaria control to elimination require adequate planning to account for transmission levels and for the structure of health and social systems. Identification of asymptomatic and imported cases is key elements for malaria control planning. Assessing surveillance capacity and selecting relevant indicators for surveillance and monitoring are key preparatory issues that help to understand how the health and social systems function in a given place. Endemic countries must work in redefine and unified clinical malarial guidelines and protocols for malaria transfusion at both rural and urban areas. It is important establish algorithms and diagnose criteria between semi immune population and immune populations from non-endemic and endemic regions. The impact and cost of malaria treatments due to inadequate management and implementation could be reduced by additional research to identify state of drug resistance and permanent sentinel surveillance systems44,45.
The monitoring and evaluation of strategies of malaria elimination must be permanent. Definition of what would contribute to forecast outbreaks and epidemics. The early detection of clinical failures in treatments will reduce the cost of changing treatments.
Latin America, has recorded contrasting evidence about the association of malaria and fever as a main symptom17,23. In similar regions, authors present contradictory results about the prevalence of asymptomatic infections, ranging from 4.2 % to 96 % 18,19,21,22,46. In Colombia, two studies conducted in Chocó and Cordoba showed similar trends to those mentioned above. The study in Quibdo, highly endemic for P. falciparum, showed the absence of asymptomatic cases among schoolchildren47. Meanwhile in Tierralta, an area endemic for P.vivax, the study found 14.6 %of cases were asymptomatic 23. These findings coincide with our results, showing exposure differences by sex and age, as well as the different symptomatic behavior patterns of the two species P. falciparum and P. vivax. Therefore, the differences in age and sex between the febrile and afebrile cases cannot be just a chance finding and merits further exploration.
These results are consistent with previous findings from other authors on the same region 11,48,49. However, it must be noted that the proportion of fever attributable to malaria appears stable at around 39-42 %. The degree of self-medication in some areas remains an important challenge to national efforts towards developing effective surveillance systems (SIVIGILA and INVIMA)
The findings of this study have implications on malaria elimination program. Currently, a malaria case is defined as any case that tests positive for parasites by thick blood smear and/or RDT. Presently, clinical cases are detected by passive case detection (PCD). Active case detection has been reduced due to costs, such as those associated with transport to endemic areas. In Colombia, the priorities are: (i) to develop strategies for surveillance-response systems adapted to a given endemic area and (ii) to adapt new strategies for primary and secondary preventive actions which consider inter sectorial partnerships.
The systematic narrative study and fieldwork show how the evidence between countries varies. There is not enough temporal and spatial information to indicate the real status of malaria elimination and pre elimination efforts in Latin America, mainly in the Amazon region. Any attempts to discuss progress towards malaria elimination will first have to elucidate and define parameters for statistically significant comparisons. Mathematical models offer a way to predict the value of progress indicators, while related informatics systems can help to evaluate the impact of elimination and control efforts considering variables of place, time and person. Tracking these epidemiological markers from infection to illness, plus setting a new threshold of fever, must be evaluated in both the short- and long-term to really have an impact on the malaria elimination strategy and redefine new programs. Finally, sentinel surveillance systems to measure and establish the state of native cases versus imported is also required between countries. The weekly report must be mandatory to forecast epidemics and prevent early presence of imported cases and avoid the malaria reintroduction in areas with Reproductive Rate close to Zero.

