











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkHealth conditions in migrant agricultural workers (MAW) in low-income settings are characterized by high levels of morbidity and mortality, being mental disorders, drug abuse, sexually transmitted infections (STI), and human immunodeficiency virus (HIV) infection common public health problems 1.
MAWS are vulnerable to STIS and HIV infection due to poor living conditions, labor exploitation, lack of social support, risky behaviors (e.g. multiple sexual partners, use of illegal drugs, and condomless sexual intercourse), and limited access to basic preventive services 2.
Sexual risk practices in MAWS leading to STI and HIV infection are associated with poverty and segregation, especially in Latin American indigenous populations with poor information about these diseases. Among these groups, the use of alcohol and drugs is also common; sexual violence and social stigma that lead to feelings of resistance, or beliefs that deter preventive measures such as the use of condoms, are also prevalent 3.
In Mexican indigenous MAWS, the spread of STIS and HIV is associated with a change of lifestyle after migrating to the United States or to domestic agro-industrial locations. While travelling, workers engage in unsafe sexual practices with infected partners in environments with limited access to health care 4,5.
Studies on STIS and HIV rates in Mexican indigenous maw are still limited and tend to underreport cases. This is largely due to the marginalization and social exclusion conditions prevailing during their seasonal migratory experience 6. The 0.29% and 0.11% prevalence of STIS and HIV/AIDS, respectively, reported in 2014 among MAWS in the United States can be used as an approximation to illustrate the epidemiological impact, as nearly 90% were Hispanic migrants, mostly Mexicans, of which a third had indigenous origin 7. While there is no accurate information about the prevalence of these diseases among indigenous MAW in Mexico, exploratory data suggest that it could be higher than the national average, and that both epidemics may interact 8.
Network of sexual partners and the spread of infections
In the social network framework, sexual relationships are conceived as the physical interaction of two or more individuals within a sociocultural context that regulates its dynamic. If such relations are grouped, they constitute a network of sex partners that can spread infections. Thus, one infected person can pass on a disease to a susceptible sex partner disseminating the infection to an extent that depends on the number of partners of the infected individual, and the new partners of recently infected partners 9.
In the traditional sexual network analysis, the risk of STIS and HIV infection is constrained by people's position within the social structure. Therefore, local (egocentric) and global (sociometric) structures become determinants of the risk of infection 10. The two local structures needed to understand the transmission of STIS and HIV within the context of a network of sex partners include the mixed selection of partners and concurrent partners.
The mixed selection of partners implies two alternatives: 1) choosing sexual partners from close or assortative networks (e.g. partners of the same ethnicity), or 2) from external or disassortative networks (e.g. different ethnicity partners or non-indigenous partners). The rationale behind this model relates to the type of partner selection, which will impact the transmission of the infection based on condomless sexual intercourse. Consequently, if selection is assortative, it will lead to higher infection rates in a community, in contrast with disassortative selection, which will function as a bridge for the transmission of infections across communities exposed to different risk levels 11.
A classic finding regarding the transmission of STIS in assortative indigenous networks was documented in 1998 when analyzing the contact tracing system of 4 544 infected people and their sexual partners in Manitoba, Canada 12. It was found that indigenous networks were made of sex couples with a linear structure (i.e. frequent change of partners and a high number of couples) and ethnic assortativity, resulting in high rates of syphilis and gonorrhea within the same community, contrasting with non-indigenous people that conformed radial networks, fewer number of couples, and lower STI rates.
Concurrent partnerships imply having simultaneous partnerships leading to direct or indirect relations among partners connected to the same sexual network, increasing the risk of infection for the partners, but not for the index case; therefore, the presence of concurrence is expected to speed up the non-linear transmission of infections 13.
Sub-Saharan Africa is a drastic example of how the high prevalence of concurrent sexual partnerships has led to the largest regional epidemic of HIV/AIDS. Differences in levels of sexual partnership concurrence between various racial or ethnic groups could explain the HIV epidemic seen in the black South African population 14.
The combination of both factors (i.e. assortative selection of sex partners and concurrence) can further increase the prevalence of STIS and HIV, as is the case among young people in Afro-American communities of the United States, where a high proportion of assortative and concurrent sexual partnerships leads to a high prevalence of HIV 15.
Network of sex partners and condom use among MAWs
Studies on MAWS have reported various associations between the structure of sexual partnerships and the use of condom in the context of labor mobility:
a) .MAWS increase their sexual activity, get involved with different types of partners, and have low frequency of condom use 16; however, condom use is higher with casual partners and sex workers than with primary partners 17.
b) .MAWS have an increased interaction with sex partners exposed to higher risks of infections in social environments where drug abuse is frequent, as well as to STIS and HIV in locations with poor access to preventive services 18.
c) .MAWS tend to form assortative sex partnerships where condom use is rare, especially if drug use is involved 19.
d) .MAWS are less likely to form concurrent partnerships where unprotected sex predominates 20.
In the light of the existing literature, this study aimed at identifying if mixed sexual partner selection, based on ethnicity, and the concurrence of sex partners were independent predictors of condom use among indigenous migrant workers in an agro-industrial Mexican context. If such is the case, these workers and their sex partners could be more vulnerable to the transmission of STIS and HIV.
The use of condom is emphasized here, as it is the most important method to prevent the transmission of STIS and HIV 21, and the most accessible for indigenous populations, which are usual beneficiaries of preventive campaigns of the Mexican health sector.
METHODS
This was an analytical cross-sectional study that used an egocentric approach to sexual networks. In this approach, the index subject (individual A or ego) names his or her sex partners (individuals B, C, D or alters) and provides information of behaviors and attributes for each of them, thus characterizing subject A's personal or egocentric sex network (no data was collected from the partners themselves). In epidemiological terms, egocentric risk-prone networks are potential sources of infections. Thus, the effects of large-scale sex networks on individuals occur partially through their immediate sex partners 22.
Participants and setting
A total of 192 indigenous MAWS were interviewed. They were active workers during the sugarcane harvest of the year 2011 in the Cuauhtémoc municipality, State of Colima, in western Mexico, where they have been employed in the production of cane sugar since the 1960s 23. Workers come from marginalized areas of the southern states of Guerrero, Oaxaca and Chiapas, where the incidence of AIDS is higher than the national average 24.
Interviewees were selected from a census of indigenous maws and their families. They lived in one of the four laborer shelters situated in the localities of Cobano, Trapiche and Quesería. Residents comprised 941 individuals, including 480 male workers, of which 213 fulfilled the following inclusion criteria: being a sexually active Nahua or Amuzgo male aged 18-29 years, employed as MAW for at least three harvest years, who lived in a sugarcane boarding facility of the Cuauhtémoc municipality. This age range was chosen as most maws were young adult men, who started their sex life at age 13-14 on average. The 3-year criterion of migratory experience assumed cumulative sex practices of risk in various working environments. Exclusion criteria involved being unable to speak in Spanish during the interview due to lack of knowledge, or to alcohol or illicit drug consumption.
Workers were contacted in the shelters and asked to participate. From 213 eligible people, 192 interviews were conducted; 12 did not speak Spanish, five had used alcohol or illicit drugs, and four refused to participate, resulting in a refusal rate of 1.8%. No women were included due to the small number of working females (n=5), and because of the high social control of their male partners within the boarding premises.
Data collection
Data was collected between March and June 2011. Community health interviewers administered a structured questionnaire in Spanish with the assistance of a trained indigenous educator, who built rapport with interviewees and helped answering questions and concerns. The interviewers, who were well-known for their preventive work in the community, were trained in the administration of the egocentric network instrument. This helped achieving a positive response from maws when approaching sex topics. Interviews were conducted in private areas of the shelter, and lasted 25 minutes on average (range 18-29).
Participants were informed about the objectives, risks and benefits of the study. Participation was voluntary and written consent was obtained. All interviews were confidential and anonymous. Participants were given preventive information about sex counseling and reproductive health services. The study was approved by the Local Research Committee of the Mexican Institute of Social Security in the State of Colima (register number R-2010-601-2).
Questionnaire and variables
The validated and adapted version of the UNAIDS structured questionnaire (United Nations' tool for tracing sexual networks) was used 25. This instrument contains 40 items distributed into four sections: attributes of socio-demographic workers (age, ethnicity, marital status, education, occupation, religion and migration experience), anonymous listing of up to eight sexual partners within the last year prior to the interview, socio-demographic attributes of the sex partners (age, mix selection by ethnicity, sex, marital status, schooling, main occupation and type of partner), and characteristics of the sexual intercourse with partners (concurrence, frequency of condom use, alcohol and illegal drug use frequencies during sexual intercourse, and coital frequency).
Data management and analysis
Egocentric sexual network data can be analyzed using the subjects' attributes as well as sets of relationships. Data was organized using a matrix where rows corresponded to workers and columns to attributes of workers, partners and sexual relationships. The matrix was converted into a dyadic format where rows were transposed into columns, allowing analyses of combined attributes of workers (n=192) and sex partners (n=360). This format was used for relational analyses between attributes of the workers and those of their sex partners. The conversion was done using the software for the analyses of egocentric networks E-NET V.0.024 26; the resulting matrix was exported to SPSS v.20 for statistical analyses.
Pearson Chi2 tests were used to identify differences in proportions between nominal data. Student t-tests and ANOVA were used for mean differences between groups in normally distributed variables, and Mann-Whitney and Kruskal-Wallis non-parametric tests for those not normally distributed. P values below 0.05 were considered statistically significant.
Factors associated with the steady use of condom were identified using binary logistic regression: unadjusted odds ratios (OR) and adjusted or with 95% confidence intervals (95% CI) were computed.
Steady use of condom, dichotomously defined 27, was the dependent variable. Mixed selection of sex partners by ethnicity 28, presence of concurrent partnerships 13, frequency of drug use during sex, and number of partners were independent variables. Variables were included in the model based on marginal statistical significance seen in bivariate analyses (p<0.10). Operational definitions can be seen in Table 1.
Table 1 Operational definitions and coding of variables included in the binary logistic regression analysis
| Variables | Definitions and questions | Codes |
| Dependent Steady use of condoma | Frequency of use in the previous year How often did you use a condom with your sex partner [number 1-8]? | 0=Sometimes or never 1=Always |
| Independent Mixed sex partner selection ethnicityb | Indigenous or non-indigenous origin of sex partners What was the ethnic group of your sex partner [number 1-8]? | 1=Same ethnicity (assortative) 2=Other ethnicity (disassortative) 0=Non-indigenous (disassortative) |
| Concurrencec | One or more simultaneous sex partners in the last year Did you have any additional sex partner during the time that you and [partner number 1-8] were having a sexual relationship? | 0=Definitely no, unsure 1=Yes, definitely |
| Illicit drug use | Drug use during sexual intercourse in the preceding year How often did you use drugs with your sex partner [number 1-8]? | 0=Never 1=Always or sometimes |
| Number of sex partners | Estimated no. of ego/alter sex partners in the last year | 0=1 sex partner 1=2 2 sex partners |
a Defined and coded based on 27; b Defined and coded based on 28; c Defined and coded based on 13
Model fit was assessed using the Hosmer-Lemeshow goodness-of-fit test; a good model was indicated by a non-significant Chi2 value (p>0.05). The magnitude of the variance inflation factor (VIF) was used to explore co-llinearity across independent variables; multicollinearity was defined when VIF values were above 3. Nagelkerke pseudo-R2 was used to determine the proportion of the variability explained by the model.
RESULTS
Characteristics of indigenous migrant workers and their sex partners
A total of 80.2% of the respondents belonged to the Nahua ethnicity, and the remaining 19.8% were Amuzgo. Mean age was 23.7 years (range 16-29); 64.5% were married or cohabiting (33.3% single, 2.1% divorced); 78.1% had primary school education or less (21.9% secondary school), and 65.6% were Catholics (13.5% non-Catholic Christians, 20.8% no religion). Within the last three years, 63.5% had migrant labor experience in Mexico, and 19.8% in agricultural fields from the United States.
Workers reported 360 sex partners (mean 2.3), from which 99.4% were women (mean age 22.5 years); 74.8% had primary education or less; 55.1% were married; 38.9% worked at home without salary; 64.5% were indigenous from the same ethnic group of the worker; 20.5% belonged to other groups, and 15.0% were non-indigenous.
Table 2 presents sociodemographic characteristics by ethnicity of sex partnerships. Nearly half of the partners were married when belonging to either the same (47.5%) or another (45.9%) ethnic group compared with 18.5% of non-indigenous partners. Education was similar for indigenous partners (comparisons were not possible for non-indigenous, as data was lacking in 59.3%). Most non-indigenous partners were sex workers (70.4%), compared with 2.6% and 13.5% of partners of similar and different ethnicity, respectively. Casual sex partners were more common with non-indigenous (77.8%) than with indigenous partners (same 27.6%, other ethnicity 43.2%). Mean partner's age was similar across groups, ranging from 21.9 in partners of the same ethnic group to 23.7 among those from another.
Table 2 Comparison of selected characteristics of sex partners in indigenous migrant workers by ethnicity
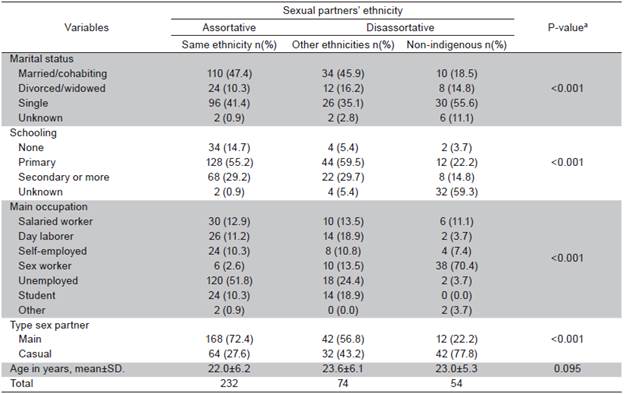
a Pearson Chi2 test was used for nominal data and ANOVA for continuous data
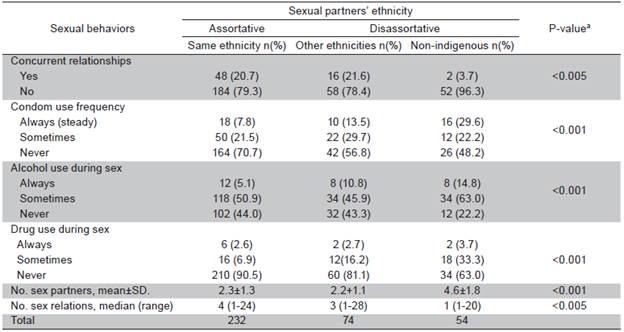
Sex behavior of indigenous maws by ethnicity of their sex partners
Table 3 shows that sexual concurrence (simultaneous existence of sexual partnerships) occurred almost exclusively among indigenous partners, with 20.7% belonging to the same ethnic group, 21.6% to a different ethnic group and 3.7% to the non-indigenous group. The proportion of steady use of condom was higher in non-indigenous partners (29.6%) than in indigenous partners (7.8% same and 13.5% different ethnicity). Alcohol and illicit drug use during sex tended to be higher in non-indigenous partners than among indigenous partners. The mean number of sex partners reported by the worker during the year prior to the interview was also higher in non-indigenous than among indigenous partners regardless of ethnicity (4.6% vs. 2.3%, p<0.001). Finally, the monthly median number of sexual relationships was higher among indigenous than in non-indigenous partners (p<0.005).
Factors associated with the steady use of condom
Table 4 shows the logistic regression model. Adjusted ORS (CI 95%) for steady condom use were lower within partnerships of same indigenous ethnicity (assortative) than in other partnerships (0.30; 0.17-0.53), in partnerships that were concurrent to other partnerships (0.27; 0.15-0.50), and in partnerships that used illegal drugs during sex to other partnerships (0.23; 0.11-0.49). Consequently, assortative partnerships, concurrent partnerships and illegal drug use were associated with increased risk (occasionally or never using condoms), and therefore exposures were unprotected. The unadjusted positive effect for the number of sex partners was lost in the adjusted analysis. The model fit well (p=0.26) and VIF was 1.21, indicating no collinearity. The final model explained 19% of the total variability.
Table 4 Logistic regression models of factors associated with the steady use of condom during sexual intercourse by indigenous migrant workers with their partners
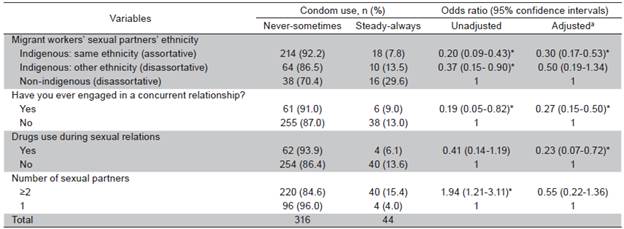
Hosmer & Lemeshow goodness-of-fit test: Chi2=8.8 (p=0.26); Nagelkerke R2=0.19; variance inflation factor=1.21; aAdjusted for all variables in the table; * p<0.05.
DISCUSSION
The adjusted ors for steady condom use were lower in sexual partnerships that were assortative and concurrent than in other partnerships and in those that used illegal drugs during sex.
Our findings support the proposed link between assortativeness and concurrence with the vulnerability to STI s and HIV infection mentioned in the sexual network theory. By hindering the constant use of condom, these variables contribute to a faster transmission and accumulation of infections in the indigenous community, speeding up the non-linear transmission of infections 11,20,29.
The use of illegal drugs also hindered the steady use of condom. This coincides with earlier studies on maws who migrated to agro-industrial environments where the use of drugs is prevalent 30, inciting workers to start using drugs or to increase their consumption.
The associations found can be interpreted as the expression of a sexual culture strongly influenced by a context of marginalization and extreme poverty, which in the case of Mexican indigenous maws, is characterized by very precarious working and living conditions with high rates of morbidity, mortality, violence, and drug abuse, as well as limited access to health and education 31. These conditions enable the development of networks of sexual partnerships that incur in risky practices that lead to STIS and HIV vulnerability, as it has also been reported among migrant workers worldwide 2.
The lower proportion of steady use of condom with indigenous sex partners also coincides with the lower frequency seen among young indigenous groups from Latin America, stressing the higher vulnerability of indigenous people compared with the general population 32. This has also been reflected in a higher prevalence of infections in global indigenous populations 33.
Various limitations should be stressed: 1) the cross-sectional design used limited the assessment of partnership formation and the trends in condom use during sex practices, which can only be assessed using longitudinal designs; 2) the use of structured questionnaires for interviews could have led to bias and measurement errors when estimating the characteristics of sex practices, including the limit to eight sex partners to reduce inaccurate recall and participant fatigue; this was reduced by using a validated and pilot-tested instrument and by training the interviewers; 3) since the study was limited to young male workers, future efforts should be made to explore the perspective of minorities in this sector, namely women, older adults, and seniors, possibly using qualitative methodologies; 4) in the interviewed group, only two workers referred having male sex partners; this could be an underestimation of the true proportion of same sex relationships resulting from a response bias given the homophobic attitudes prevalent in the Mexican indigenous sexual culture, which can be associated with fear of discrimination and violence for having partners of the same sex 34, therefore, risk practices in men who have sex with other men need to be further investigated; 5) steady use of condom was dichotomously coded to obtain a robust indicator of consistent use; however, this measure should be further complemented with questions dealing with adequacy of use; 6) the variable "concurrence" focused on workers' reports on simultaneous sexual partnerships within the last year as an approximation to the risk of transmission in the partner, yet this measure could be improved using other two complementary measures: perceived concurrence among regular partners, and perceived concurrence based on temporal duration; and 7) findings cannot be generalized to other populations, as the study only dealt with asugarcane agro-industrial context and two ethnic groups, while the real population of migrant workers comprises many indigenous groups; thus, results can only be extrapolated to workers of similar ethnic, migration, social, and working characteristics.
In spite of the limitations, the study concludes that two egocentric sex network variables (assortative and concurrent partnerships) favor the low frequency of steady condom use, increasing the vulnerability of STIS and HIV transmission. The negative impact of illegal drug use, which appears to be growing among indigenous MAWS, needs to be considered.
In terms of preventive actions targeted to indigenous MAWS, these results could lead to the implementation of STIS and HIV risk reduction measures using complementary schemes through a structural approach aimed at improving socioeconomic and sanitary conditions in working places, including access to intercultural services of sexual, reproductive and mental health 35, and by developing culturally-contextualized preventive strategies for condom use in partners with assortative and concurrent sexual partnerships 15 ♦

