











 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkAccording to UNAIDS, in 2013, there were 35 million people infected by HIV around the world, and 19 million of them were not aware of being seropositive 1. Brazil, in the global context of the prevention of HIV transmission and the implementation of strategies to counter its rapid spreading, stands out for its fast response and having implemented cutting-edge strategies since the epidemic started, by promoting an innovative approach that involves political commitment and scientific evidence, which in turn contributes to the understanding of the social-sanitary impact caused by HIV from a human rights perspective 2,3. In spite of this, Brazil ranks as one of the four Latin American countries with most cases of HIV, as 47% of Latin Americans with HIV live in this country 1.
In Rio Grande do Sul state, in south Brazil, and in particular the city of Porto Alegre, a high number of AIDS cases keeps being reported. In 2013, aids incidence rate in the state was 41.1 cases per 100 000 people, twice the national average. In addition, Porto Alegre presented more alarming rates, with 93.7 cases per 100 000 people 4.
In Brazil, approximately 41% of AIDS patients begin treatment in advanced stages of the disease 5. In this sense, the available literature emphasizes that the more time passes to start treatment, the more difficult to restrain the development of the disease, which causes both an increase in mortality rates, and VIH transmission rates, as well as higher costs to be assumed by the State as treatments in advanced stages of the disease are more expensive 6-11. Failure to start treatment in the early stages of the virus transmission is mainly caused by the fact that infected people are not aware of being seropositive, which has been associated with factors such as health care access barriers (which includes diagnosis) and by people's beliefs on the disease, for most of the times they don't think they are at risk of being infected with the virus or they fear discrimination 12.
In order to reduce late diagnosis, some actions have been carried out to increase access to HIV tests, mainly by using rapid HIV testing. The implementation of rapid VIH tests is supported by its efficiency and reliability, but also by its cost-benefit ratio 13,14. Another advantage it offers is the possibility to provide immediate care to HIV infected people in the Brazilian public health care service (SUS for its acronym in Portuguese) 15. Several studies have assessed the cost-effectiveness rate of rapid tests in several countries 14,16,17, confirming the effectiveness of this option for all types of population 16,18 and suggesting state health systems should focus on using these tests in population groups deemed as vulnerable 17.
The Brazilian Ministry of Health 19 stresses that the main advantage from changing from traditional to rapid testing is time reduction between collecting the samples and getting the results. Furthermore, in order to strengthen the advantages rapid tests offer, it is necessary to use health strategies such as counseling and education in order to bring closer health service users and health professionals 20,21. Some of the goals to be achieved through counseling include reducing stress levels, reflecting on infection risks and the adoption of safer practices, reinforcing adherence to treatment, and developing communication channels with sexual and injectable drugs partners.
One of the benefits of Rapid VIH Testing is that population groups with higher epidemiological vulnerability to HIV, syphilis, and hepatitis B and C infections, such as trans people, young gay adults, sex workers, drug users, homeless people, and people with other sexually transmitted diseases (STD), have larger probabilities to access diagnosis of the disease or the virus infection by means of this testing method 4,22-24. In this regard, some studies have reported that these population groups face challenges when accessing health care services due to the prejudice and discrimination they are subjected to 25,26, therefore, these individuals frequently express their preference for attending specialized centers, where they think health care professionals are better prepared for their needs 25.
The objective of this paper is to analyze how health professionals and health service users asses counseling on Rapid HIV Test, as well as its implementation, focusing on positive aspects, barriers, and limitations, and analyzing the possible meanings that are assigned to STD, and HIV/AIDS. Besides, as Rapid HIV Testing is a new technology, still under implementation in other contexts, the Brazilian experience could be used as a parameter for its implementation in other countries.
METHOD
This is a qualitative, exploratory and descriptive study carried out at one of the first Counseling and Testing Centers (CTC) designed to implement Rapid HIV Tests in Brazil, located in Porto Alegre, Rio Grande do Sul. Data collection was made through semi-structured interviews administered to 14 health professionals and 27 users of the CTC who were tested through rapid testing technology for HIV, syphilis, and hepatitis B and C diagnosis, and who were considered as vulnerable population. In order to guarantee data confidentiality health professionals' socio-demographic characteristics will not be disclosed, and they will be identified as P1, P2, etc. Service users' socio-demographic information is presented in Table 1.
Table 1 Socio-demographic characteristics of the interviewed users
a MSM: Men who have sex with men; b STD: Sexually Transmitted Disease
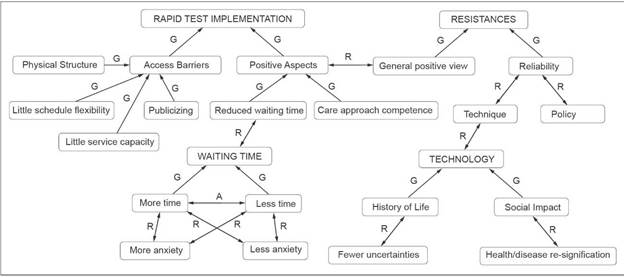
Each participant answered a 30 minutes semi-structured interview, which was audio recorded, transcribed, and digitalized, obtaining a unique textual corpus 27. A coding process (Figure 1 - Axial Coding) was set up as proposed by Flick 28. An initial stage of open coding generated 20 categories that were organized a posteriori in axes. Axial coding was the next analysis step when relationships between them were identified, and established on 4 axes. Finally, a selective coding was performed by integrating the data according to literature findings in this regard 28.
In this research, ethical considerations were ensured. The project was submitted to and approved by the Research Ethics Committee of the Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS). All participants signed a free and informed consent form.
RESULTS
Results are presented under the following theme-based categories: Positive aspects of the technology; access barriers; people's resistance to new technologies; waiting I got here and realized it was a rapid test, I was very surprised. I time; social impact. thought it was very good." (U1).
Positives aspects of the technology
All participants considered that changing from conventional to rapid testing was a positive aspect, and emphasized the benefits of a reduced waiting time for obtaining the test results: "Go there and get tested, because it's good and fast, and you can make it in just a day. All other times I went to the lab I had to wait three or four days, even seven days, and waiting for the results feels just like hell." (U11).
The association between waiting time and the possibility to make adjustments to the service provision taking into account users' needs and daily routines was pointed out as one of rapid testing advantages: "[…] because of the service, its promptness, its quality, and the results you will obtain; besides, instead of wasting time sitting around and going back and forth between different places, you are able to do something fast and you get the results right away, so you can treat it faster, right?" (U2). Health workers also highlighted the time reduction as an important aspect that helps increasing effectiveness in relation to the assistance that is provided to users: "About 20% of the people tested didn't come back to get the results […] (in relation to the prior HIV test in which 30 days were necessary for receiving the results) (P13).
Likewise, some participants stated they considered rapid testing as an example of provision of health care services in which Brazil's public health system (SUS for its acronym in Portuguese) exceeded the provision time of private health care providers: "Even in private health care service provision you can't get it so fast, can you? I wondered how it was going to be if the service was provided by the SUS. So, when I got here and realized it was a rapid test, I was very surprised. I thought it was very good.” (U1).
Access barriers
Respondents reported several access barriers, including poor physical infrastructure, the need to provide more information to the general public on both rapid testing and the service itself, the need to achieve and provide more service capacity, and to do it in alternative hourly schedules, and the need to offer better guidance right after the arrival at the location where rapid testing is offered: "[…] Infrastructure here is really poor. If you look closely, the furniture and other stuff are really old and damaged. But this is on the Brazilian government; it has nothing to do with the service itself." (U4).
The poor condition of physical infrastructure was an aspect that was stressed by almost all health care professionals. In this regard, participants stated that a reorganization of the services implementing rapid tests was necessary, mainly because there are two moments involved in HIV rapid testing: counseling and testing, both requiring a private area to be performed. Therefore, during this process, the initial situation was "unstable", as emphasized by one health care worker: "[…] a room with no windows, nor natural light, which is totally inadequate to perform rapid testing" (P13). This situation may lead to difficulties in performing the test, such as damages to the collection and reading materials, users' blood pressure increase and breathing difficulties, factors that can be easily avoided with a proper planning.
It is important to have in mind that no physical infrastructure changes were made in this CTC when it was decided to shift from conventional testing to rapid testing. As a result, some users and professionals considered daily service provision capacity as an access barrier: "the service should also be offered in different time frames, taking into account workers, as rapid testing, even if it is fast, requires some time. Also, there are not enough daily tickets to be given for accessing the service, right? [...] I think there should be more tickets." (U7).
Another aspect was the need to improve the service provision publicizing strategies: "There should be better publicizing strategies, right? Now we have rapid testing, ok, and then what? When do you have to take the test? Where do you go? How will you proceed? Where is it offered? Can you go?" (U11).
An important negative aspect reported by health professionals was the lack of communication among them during the implementation process of rapid testing. "It can be done one way or another, but we health professionals have to communicate with each other." (P9). Rapid testing produced a series of changes in the CTC professionals' working process, as well as in other departments. Changes in the workflow can cause staff transfers, resistances, and adjustments: "[…] It was a year where many changes were made, from the tags we print to our relationship with coworkers, in particular the lab staff, who would be in charge of processing the HIV and syphilis tests here in the lab." (P13).
People's resistance to new technologies
Changes in HIV testing process in Brazil have caused some people to distrust this new technology, along with the benefits of increasing access coverage to determine serostatus in the general population. The implementation of this new technology in health facilities was followed by fear, since promptness could be associated with results of inferior quality. Some of the health professionals that were interviewed, with the exception of counselors, showed some levels of uncertainty in this regard: "Is it as reliable, I mean, rapid testing, as the conventional one? Whether it's reliable or not, I am not sure, it could be 50%, γ0%... I don't know." (P1).
However, it seems this uncertainty was caused by the lack of information and communication between health professionals, provided that those who were not involved in administering HIV rapid tests did not have information on the quality or reliability of this technology: "[…] To be honest, I believe it is more (effective) than the traditional test, for there is the window period issue, as in traditional tests seropositivity is detected in a 14 days period." (P10).
Also, a level of uncertainty regarding rapid testing was observed in some users: "The difference, actually, is time reduction, as it is more practical, but I still have doubts about the diagnosis quality, even though I know things are improving more and more every day." (U14). Nevertheless, the lack of trust in this new technology did not make the interviewees to state their preference for other testing technologies. In these interviews, opinions on getting the result in just 30 minutes as an advantage for diagnosis were mixed, as some levels of insecurity were observed. In one particular case, a participant distinguished rapid testing trust levels between the service offered in the CTC and the health care center, while she referred to some comments she had listened to: "The rapid test offered here, in the public health care center is not reliable. They told me that. That's why they came here today to take the test here. I heard about this in the corridor." (U24).
Waiting time
During the interviews, users perceived results waiting time as a difficult and distressing moment: "It was tense. It was very hard, because it's scary, right? I had a lot of doubts, so I was really afraid." (U18). Likewise, it is possible to conclude that perceptions regarding waiting time were linked to users' seropositive results: "It's good waiting this time there, I mean, that half an hour. […] But it was hell. I swear it, when I entered the room I almost asked them not to let me know (the result). I used to take the test (in private labs,) and there you had to wait, and maybe anxiety was not so high." (U11).
On the other hand, health professionals also commented that the implementation of this new technology reduces anxiety: "[…] What I know is that it has come (rapid testing) for the best. Before, people had to wait for a long time, and now they leave the facility with everything in their hands. I think that's important. [...] (Before, it used to take) up to 20 or 25 days for receiving the results. People felt distressed while waiting for the results." (P7).
Social impact
In general, users did not show deeper thoughts about rapid testing or HIV, and they limited themselves to assess it in a more personal context, directly involved in their own lives, and mainly focused on the advantages getting the test results on the very same day would represent. Only four respondents talked about possible new meanings for the disease due to technological advances: "I believe that in the future people will have a very different opinion on HIV. Of course it can be treated without facing major difficulties; it's something that will not scare you so much." (U1). Health professionals also reported that this way of accessing HIV testing can help overcoming the stigmas related to being diagnosed with HIV, as shown in the following excerpt: "I think it also serves to break this stigma and demystify the disease, as it is something simpler and closer, if you think about it…" (P10).
On the other hand, it is necessary to be careful not to trivialize rapid HIV tests, even if it is to facilitate the access to HIV testing and starting its proper treatment, as reported by an user: "I think that attitudes change because the test becomes a routine, for example, I get off work, and now I'm going there to take it (the test) as if I went in the bakery to eat a biscuit, something like this, or as if I were to pee for a urine test." (U14). For this reason, it is required that during the counseling process the health professional discusses the importance of prevention with the user.
DISCUSSION
It is important to note that one of the main problems of the HIV/AIDS epidemic in Brazil is that nearly 41% of people diagnosed with it begin treatment in advanced stages of the disease 5,19. Therefore, rapid HIV test implementation may result in patients getting a faster and more effective access to treatment, as it allows referring users to treatment right after they are diagnosed. Moreover, the fact that Brazil is one of the first countries in Latin America to implement rapid HIV testing for all users may contribute to the assessment and implementation of public policies aiming to reduce aids transmission rates in other countries.
Regarding the positive aspects of the technology, results show that the CTC users reported a high level of satisfaction with the testing service. In this sense, another study carried out in 12 CTCS of Rio de Janeiro stated that users were very satisfied (58%) and satisfied (38%) with the assistance they were given, which represented a total satisfaction of 96% 29. In addition, Paltiel et al. 16 reported an association between the provision of rapid tests and an increase in the number of people who were voluntary seeking for options to take the test in the United States.
From the users' perspective, the assistance received in the CTC (administered by the SUS) had a better quality than the service provided by private institutions. These opinions are contrary to advanced capitalism ideologies, where the idea that private services are better than public ones prevails. Strategies like these stress the innovation capability of the Brazilian health system to face the HIV/AIDS epidemic, as the sus ability to diagnose and treat patients with HIV in the public health system has been proved over time.
One of the access barriers reported by the users interviewed here was the lack of information on rapid HIV testing and its poor dissemination. Another concerning issue was that they felt exposed at the reception of the facility where the service was being provided. This issue has already emerged in previous studies as a challenge to overcome for achieving a more humanized health care service assistance at the moment of performing HIV testing 25. Due to the prejudices and discrimination that are still associated with HIV and other STDS, users expressed their need to feel the least possible exposed when taking the test.
The condition of the physical infrastructure where Rapid HIV tests were performed was reported as a dissatisfaction factor by participants included in this study, which is an aspect that has also been described in prior studies 25,29. Both, health professionals and users, reported their highest level of dissatisfaction was related to the condition of the facilities, who expressed that the lack of adequate facilities and materials to administer the test was evident, and that a renovation process was required 29.
Regarding resistance to rapid HIV testing technology, users were provided with counseling on their doubts and insecurities. Telles-Dias et al., 22 in a study on rapid test acceptability, addressed this issue and reported that a small number of their respondents (4.5%) expressed they might had not taken the test for they were not prepared for the result or simply because they did not consider the test as reliable. Therefore, this situation requires health professionals to provide proper counseling by using detailed information and in a responsible way.
Rapid HIV test implementation had a great impact on the CTC. A prompt and precise diagnosis may reduce patients' anxiety levels as they don't have to wait much for getting the test results. Consequently, one of the strengths of this technology is that it reduces waiting time considerably, as results are obtained almost immediately. In this sense, Diaz-Bermudez 15 concludes that the potential advantages of rapid tests strengthen the importance of their promptness, practicality, and easiness, and that most users believe waiting time reduction is a positive aspect, since by removing the long waiting times for getting the results most of them are relieved from suffering a long "emotionally stressing" waiting period 22. Therefore, waiting time reduction has required counselors to make certain changes in their activities, as now they must prepare users for the test, provide them with detailed information, and make sure they are ready to get the results in a very short period of time 22. Other studies carried out in different contexts suggest using this waiting time for implementing educational interventions 15,30,31.
On the other hand, shorter waiting times between taking the test and getting the results may decrease HIV stigma. As Girardi et al. 14 argue, an early treatment, together with proper counseling and mutual understanding between partners, might help reducing the occurrence of secondary transmission of the virus by newly infected people. HIV/AIDS incidence determination by conventional methods is complex and expensive, which highlights the importance of using rapid tests 14.
Perceptions on HIV-related stigma or conventional testing access barriers are factors stressing the need to implement different action strategies, such as keeping the provision of these specialized services, and using new technologies in the provision of health services 30,32.
Likewise, chronic diseases self-management and self-management support are fundamental for daily care. On the other hand, there seems to be a tendency to pay more attention to significant advances in the effectiveness of interventions addressing HIV physical effects, than those dealing with the psychological or social issues arising from being infected with the virus, i.e. those factors that have a negative impact in patients' personal lives, for example being stigmatized, facing sexual intercourse challenges and trying to conceal their condition (anonymity) 30,32.
However, health care professionals must be alert and sensitive to reach people's needs, since this disease affects both social and private life; HIV/AIDS carriers face greater stigmatization and discrimination than other population groups, and some end up by abandoning proper treatment 33. Therefore, lack of proper support reduces the users' ability to maintain their current physical condition, which highlights the importance of health professionals' involvement with users in terms of achieving better health conditions 34.
Finally, the results obtained here allow concluding that the implementation of rapid HIV tests offers some advantages from the perspective of both health professionals and users, for example a considerably reduced waiting time, which translates into reduced anxiety levels. Both users and professionals emphasized that rapid testing is an effective care strategy, given that once users are given their results, they can be promptly referred to start proper treatment, so that immediate care is achieved. In this regard, it's worth noting that, based on the interviews made to health professionals in this research, about 20% of users did not wait or return to the facility to get their results (in relation to the traditional test administered before rapid HIV testing implementation), which may represent a risk factor for delayed treatment.
One weakness of rapid tests implementation is that some users and health professionals still question their efficacy, quality, and reliability. Therefore, it is important to develop strategies to disseminate, in an effective way, information on the reliability of this technology to both the general public and all health care units staff members.
Users also stressed the fact that there was no need to schedule the test, as well as the attention received. Likewise, they also considered health professionals' proper care approach before and after the test, and individual counseling as positive aspects of the test implementation. Considering that this study focused on users who may be considered as part of vulnerable population groups, the possibility of receiving personalized attention, in which they or their actions are not judged, was deemed as a factor encouraging self-care.
It is possible to conclude that the integration of the perspectives of professionals and users on this policy will help improving rapid HIV tests implementation in other CTCS. As Barroso 35 mentions, the relevance of studies carried out in health care centers is the production of knowledge regarding their operation, ways to improve their performance, and how do they contribute to the design and execution of public policies. Thus, by improving the quality of health care and by increasing access opportunities to it, it is possible to re-signify perceptions on health and disease, mainly in relation to HIV/AIDS stigmas 34.
The 30 minutes waiting time can be used to implement adherence strategies regarding treatment, preparation, and psychological support to receive the results. The experience reported here could be used as an example to encourage other CTCS to implement rapid HIV testing provision to all users. This study provided weaknesses and strengths of this policy implementation 

